4006
Evaluation of imaging features and prognosis of CK19-positive small hepatocellular carcinoma patients based on gadoxetic acid enhanced MRI1Affiliated Nantong Hospital 3 of Nantong University, Nantong, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Hepatobiliary, Biliary
Motivation: HCC expressing CK19-positive has a poor prognosis, and accurate preoperative prediction of CK19 is essential for determining the prognosis and treatment options for HCC patients
Goal(s): To explore the prognostic factors of CK19-positive small HCC
Approach: In this study, a nomogram to predict C19-positive small HCC was successfully constructed, and predictive factors for early recurrence in patients with C19-positive small HCCwere clarified.
Results: Rim APHE may help to predict early (2 years) postoperative recurrence in patients with CK19-positive small HCC (≤3 cm).
Impact: In this study, a nomogram to predict CK19-positive small HCC was successfully constructed, and predictive factors for early recurrence in patients with C19-positive small HCC were clarified.
Introduction
Liver cancer is the 6th most common cancer and the 2nd leading cause of cancer-related death worldwide[1-2]. Cytokeratin 19 (CK19) is one of the stem cell markers of HCC and is usually expressed in hepatic stem cells and bile duct cells but not in hepatocytes[3]. In HCC (HCC) patients, CK19-positive patients usually have a worse prognosis, a higher recurrence rate and lymph node metastasis[4-5]; therefore, when HCC patients are positive for CK19, the resection of tumor foci should be expanded to reduce postoperative recurrence and the metastasis rate. Therefore, the aim of this study was to compare the preoperative imaging findings of CK19-positive patients with HCC less than 3 cm with those of CK19-negative patients with small HCC to determine the prognosis of patients with CK19-positive small HCC after radical resection.Materials and methods
A retrospective analysis of 58 patients with CK19-negative HCC and 31 patients with CK19-positive HCC who underwent radical resection was performed. Two radiologists evaluated the preoperative MRI findings. The important findings for distinguishing the two groups were identified in univariate and multivariate analyses. Intragroup correlation coefficients and Kappa values were used to compare the agreement between the two observers. Postoperative recurrence-free survival rates were also compared between the groups.Result
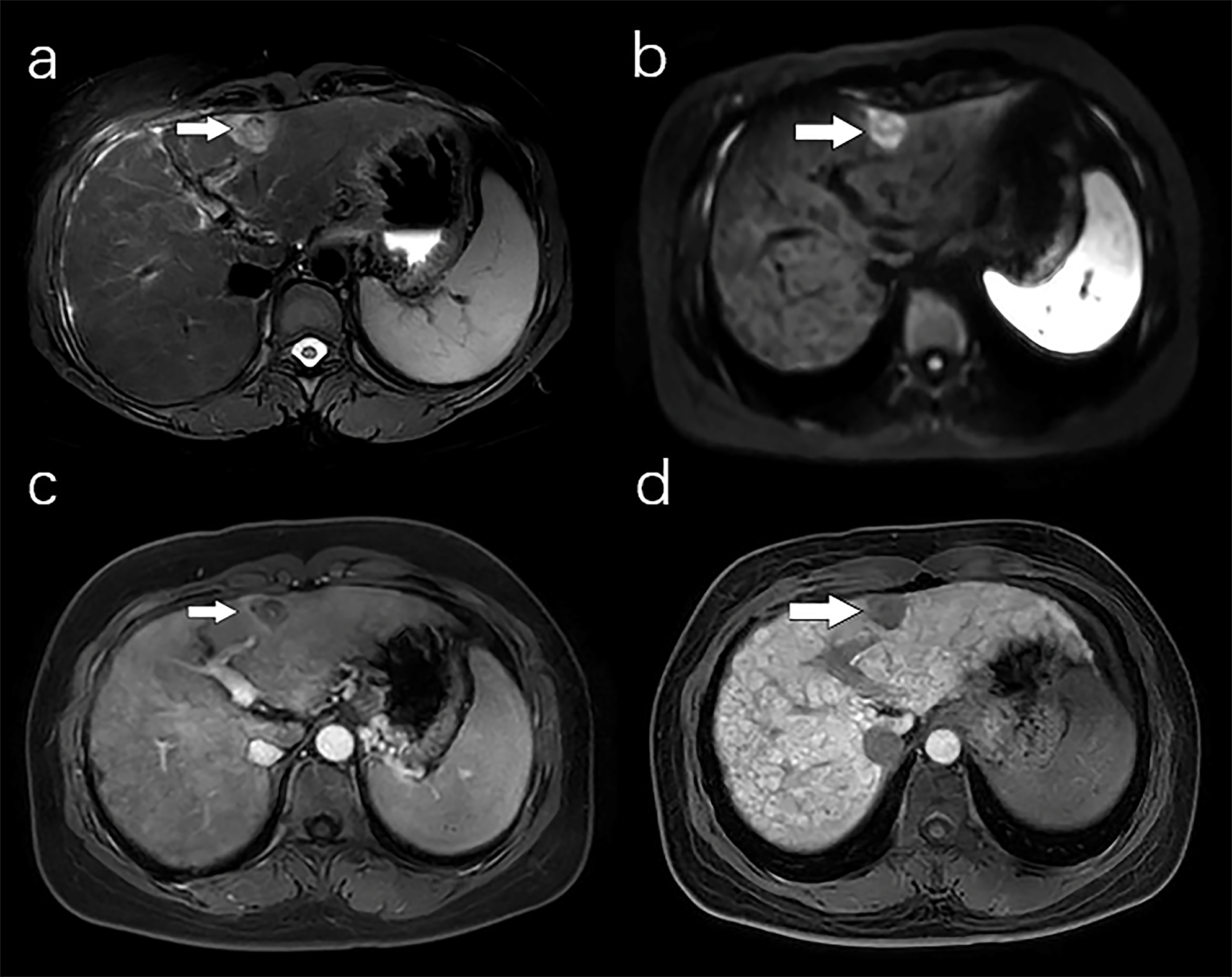
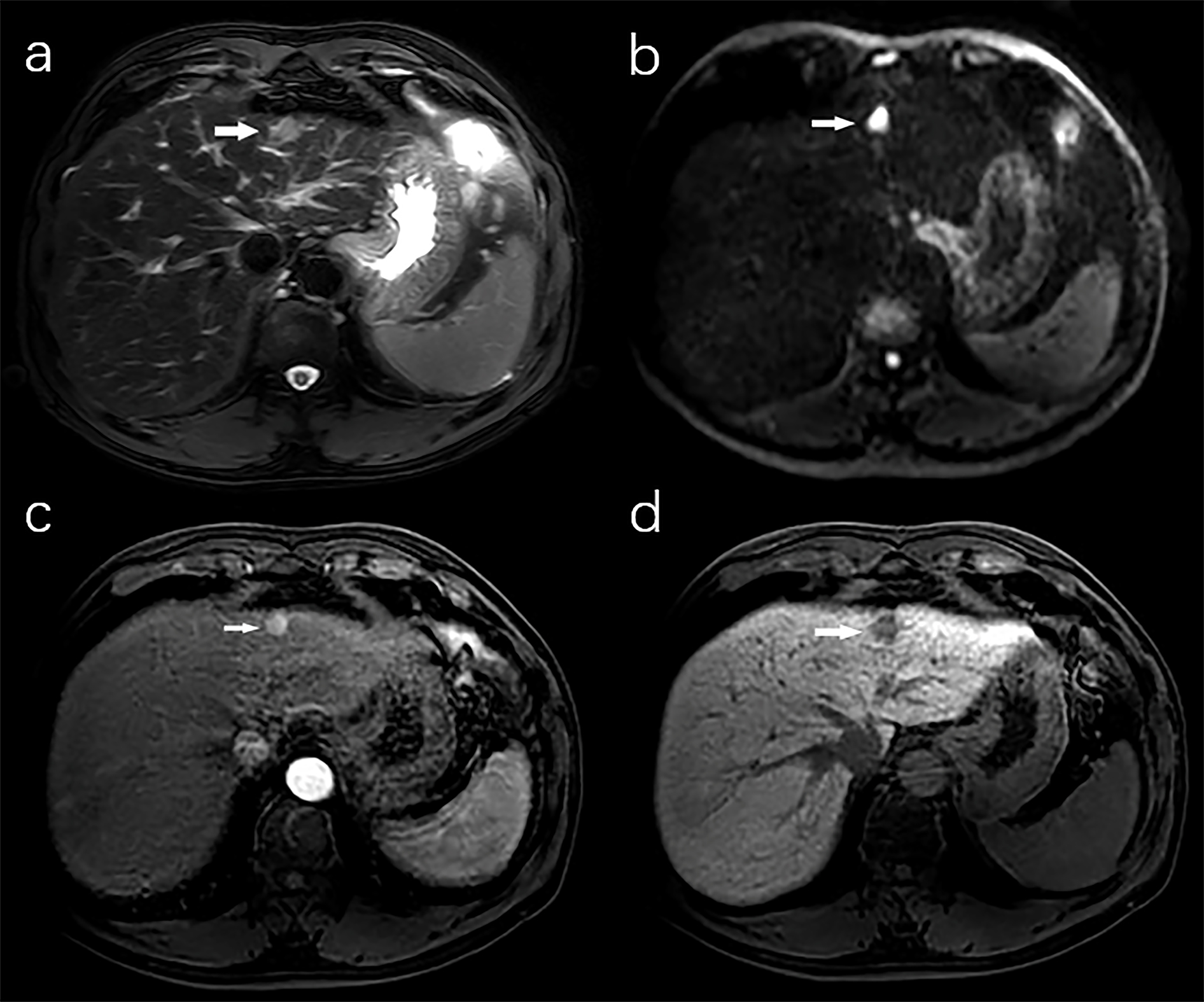
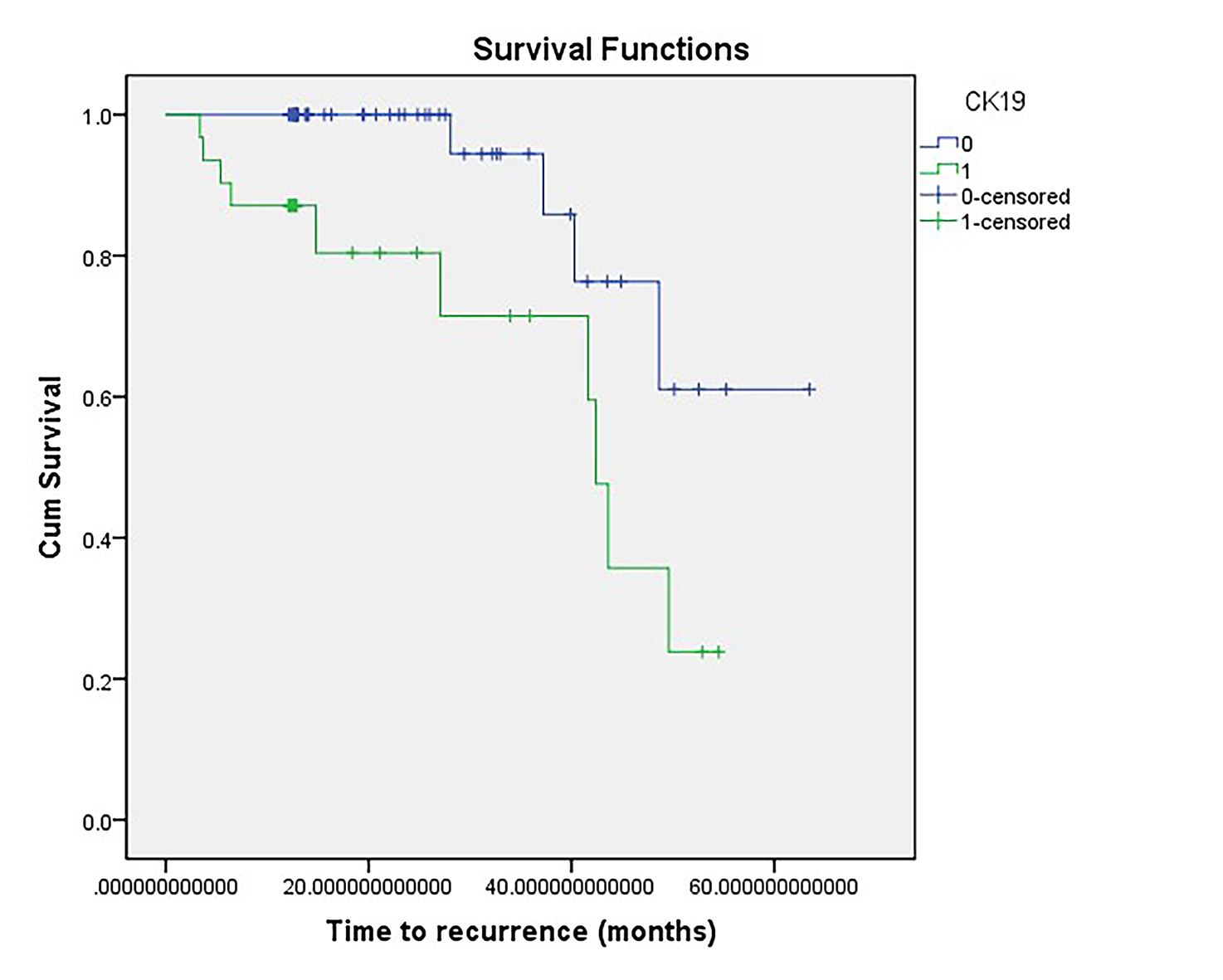
In the univariate analysis, statistically significant differences were observed in terms of AFP elevation, Rim arterial phase hyperenhancement (Rim APHE), peritumoral enhancement in the arterial phase, Targetoid restriction and the lesion to liver contrast ratio in hepatobiliary phase (LLRhp) reduction. Cox survival analysis showed that Rim APHE was associated with recurrence after hepatectomy (HR=22.16, p=0.001). Kaplan–Meier survival analysis showed significantly lower recurrence-free survival in the CK19-positive group than in the CK19-negative group after radical resection (1-year 87.1% versus 100.0%, 2-year 71.5% versus 94.4%, and 3-year 59.6% versus 85.9%, P=0.006).Conclusion
Rim APHE in gadoxetic acid-enhanced MR imaging may help to predict early (2 years) postoperative recurrence in patients with CK19-positive small HCC (≤3 cm).Discussion
In this study, we found that imaging signs such as Rim APHE, peritumoral enhancement in the arterial phase, Targetoid restriction, lower LLRhp and elevated AFP are associated with CK19 expression, among which Rim APHE is a risk factor for recurrence in patients with HCC. Rim APHE and DWI target signs were closely associated with CK19 expression in HCC; The reason was that Rim APHE and DWI target signs are important independent signs for predicting intrahepatic cholangiocarcinoma (ICC) [6], and these two signs are associated with pathological patterns of hyperproliferation around the ICC tumor and central interstitial fibrosis [7]. CK19-positive HCC is pathologically prone to form intratumoral pro-fibroplastic interstitium, which has pathological similarities to ICC and is more commonly found in CK19-positive HCC than in typical HCC. CK19-positive HCC patients had a lower LLR in the hepatobiliary phase than CK19-negative patients, The reason was that SI on HBP images was negatively correlated with the histological grade of HCC; this negative correlation was also associated with the gradual decrease in organic anion transporting polypeptide (OATP, including OATP1B1/3) expression[8]. Peritumoral enhancement in the arterial phase is more frequently seen in imaging manifestations of small liver cancer patients with CK 19 positive, The reason was that that with the development of HCC, tumor drainage shifts from the hepatic vein to the peri-neoplastic blood sinusoid or portal vein in the fibrotic capsule of the lesion due to early occlusion of the hepatic veins either intratumorally or extratumorally[9].Acknowledgements
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.References
1. Bailey A, Shah SA. Screening high risk populations for cancer: hepatobiliary. J Surg Oncol 2019;120:847–50.
2. Kim TH, Yoon JH, Lee JM. Emerging role of hepatobiliary magnetic resonance contrast media and contrast-enhanced ultrasound for noninvasive diagnosis of hepatocellular carcinoma: emphasis on recent updates in major guidelines. Korean J Radiol 2019;20:863–79.
3. Lei Z,Li J,Wu D et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis B virus- related hepatocellular carcinoma within the milan criteria. JAMA Surg 2016;151(4):356-363.
4 Kierans AS, Leonardou P, Hayashi P et al. MRI findings of rapidly progressive hepatocellular carcinoma. Magn Reson Imaging 2010;28(6):790–796.
5. Ariizumi S, Kitagawa K, Kotera Y et al. A non-smooth tumor margin in the hepatobiliary phase of gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance imaging predicts microscopic portal vein invasion, intrahepatic metastasis, and early recurrence after hepatectomy in patients with hepatocellular carcinoma. J Hepatobiliary Pancreat Sci 2011;18(4):575–585.
6. Park HJ,Kim YK,Park MJ et al. Small intrahepatic mass- forming cholangiocarcinoma:target sign on diffusion- weighted imaging for differentiation from hepatocellular carcinoma. Abdom Imaging 2013;38(4):793-801.
7. Ni T,Shang XS,Wang WT et al. Different MR features for differentiation of intrahepatic mass-forming cholangiocarcinoma from hepatocellular carcinoma according to tumor size. Br J Radiol 2018;91(1088):20180017.
8. Kim JY, Kim MJ, Kim KA, Jeong HT, Park YN. Hyperintense HCC on hepatobiliary phase images of gadoxetic acid-enhanced MRI: correlation with clinical and pathological features. Eur J Radiol 2012;81(12):3877–3882.
9. Kitao A, Zen Y, Matsui O, Gabata T, Nakanuma Y. Hepatocarcinogenesis: multistep changes of drainage vessels at CT during arterial portography and hepatic arteriography radiologic pathologic correlation. Radiology 2009;252:605–614.
Figures