3998
Differentiation of hepatocellular adenoma and well-differentiated hepatocellular carcinoma using MRI and clinical-based nomogram model1National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, Shanxi, China
Synopsis
Keywords: Liver, Tumor
Motivation: Hepatic hyperintense lesions, has been shown to be difficult for differential diagnosis in clinical.
Goal(s): Multiple parameters MRI can potentially provide whole insights into hepatic lesion diagnosis.
Approach: 144 patients based on hepatic hyperintense lesions (HCA and WDHCC) with presurgical MRI to investigate the differential diagnosis.
Results: Results demonstrated that MRI signal model can provide more effective information for the differential diagnosis of hepatic hyperintense lesions especially for HCA and WDHCC.
Impact: Differentiating Hepatocellular adenomas (HCA) and well-differentiated hepatocellular carcinoma (WDHCC) via MRI signal-based model could offer a more comprehensive diagnostic approach than clinical factors-based model and combined MRI signal plus clinical factors-based model.
Introduction
Hepatocellular adenomas (HCA), are benign, solid liver lesions that develop in otherwise normal livers, often in the setting of increased estrogen levels. While considered a benign tumor, there is a risk for substantial complications such as hemorrhage and malignant transformation (1). While hepatocellular carcinoma (HCC) develops on a background of chronic liver disease in 70–90% of all patients such as hepatitis B virus (HBV) infection, non-alcoholic liver disease (NAFLD), etc. The Edmondson grading system is used to classify the different histological grades of HCC into 4 categories, generally corresponding to well-differentiated, moderately-differentiated, poorly-differentiated, and undifferentiated (grade I-IV, respectively). Studies have shown that multiphasic MRI performed with contrast agents remains the best method to noninvasively detect, characterize, and monitor HCAs and HCC (2). Still, it is difficult to differentiate the HCA and WDHCC because both perform hyperintense enhancement. Given this context, our study aims to assess the qualitative analysis of MRI and clinical features to differentiate HCA and WDHCC. We hope this study can provide more well-established quantitative features for differentiating HCA and WDHCC noninvasively.Methods
This retrospective study was approved by the local ethics committee. One hundred and forty-four patients pathologically proven HCA (n=35) or WDHCC (n=109) underwent contrasted MRI were enrolled. Univariate and multivariate logistic regression analysis was included to determine the independent predictive factors and establish the regression equation. One retrospective set (n=101) was used to develop and internally validate the predictive model. The clinical, radiological and laboratory features were collected and subjected to logistic regression analyses. The primary predictive model was displayed as a nomogram and then modified into the externally validated in an independent set (n=43). On this basis, the nomogram prediction model was constructed. The discrimination, clinical efficiency of the nomogram were assessed using area under the curve (AUC), decision curve analysis (DCA) and clinical impact curve. Statistical analysis was performed by using R software (version 4.2.0, www.r-project.org). A two-sided p value less than 0.05 was considered to indicate statistical significance.Results
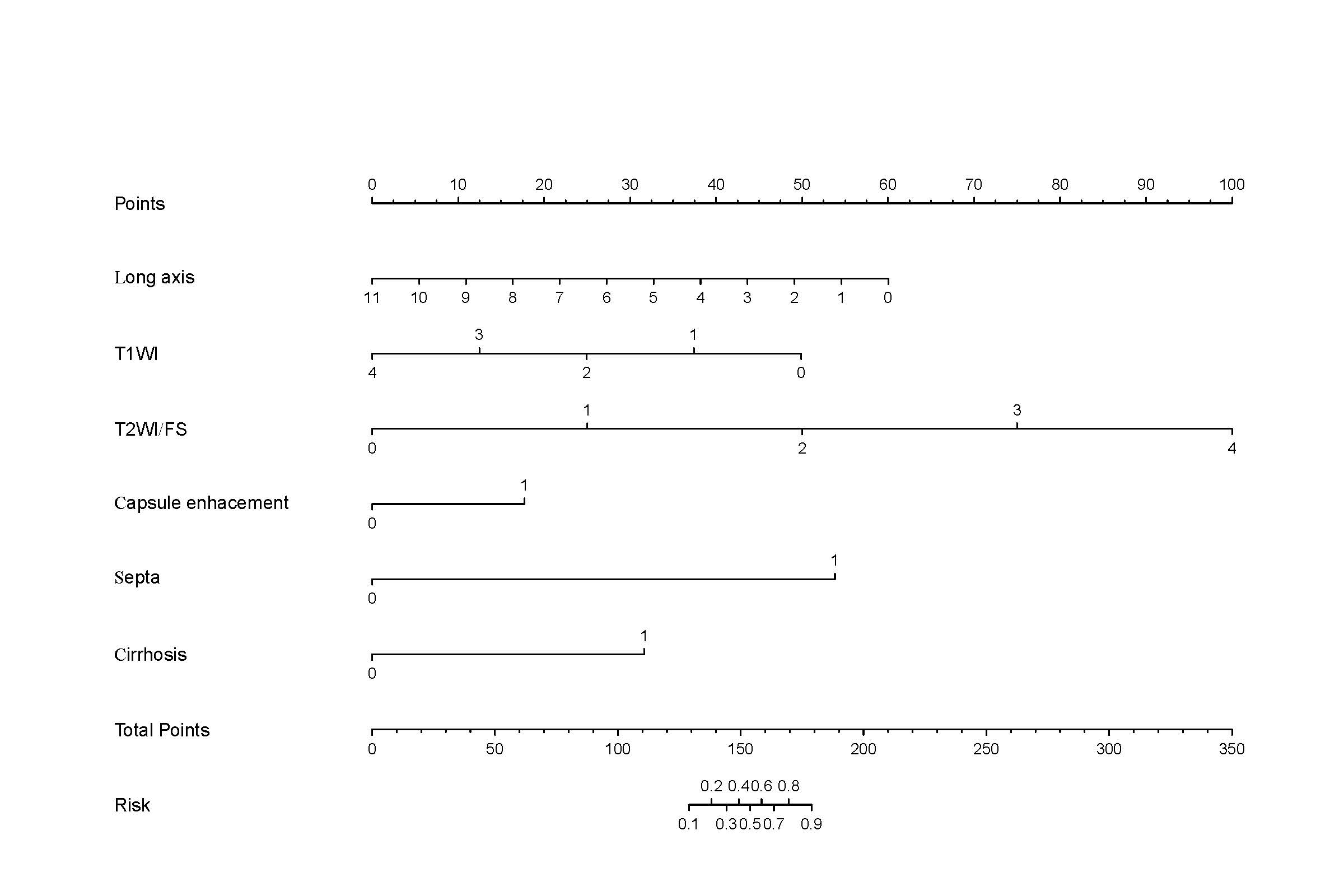
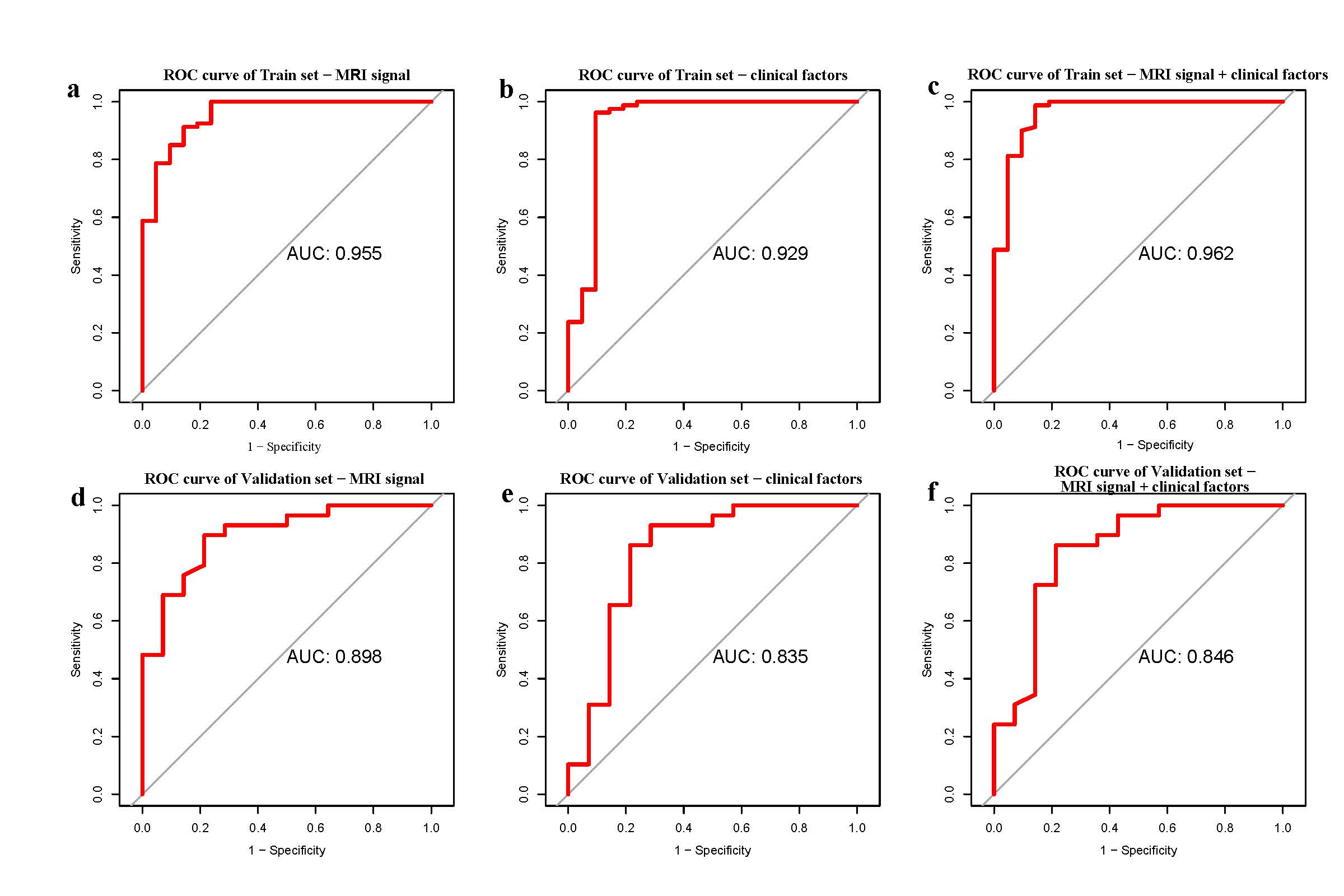
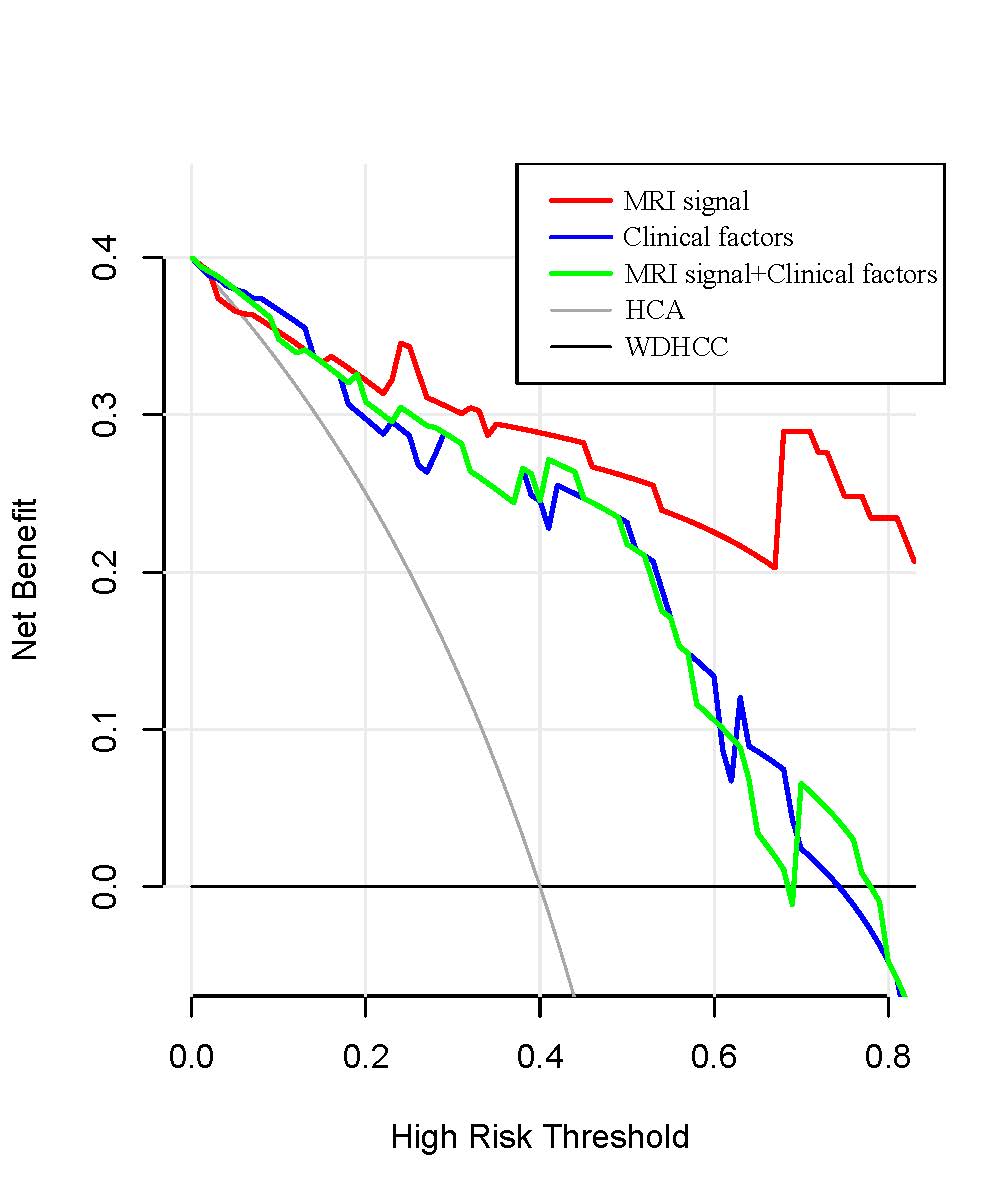
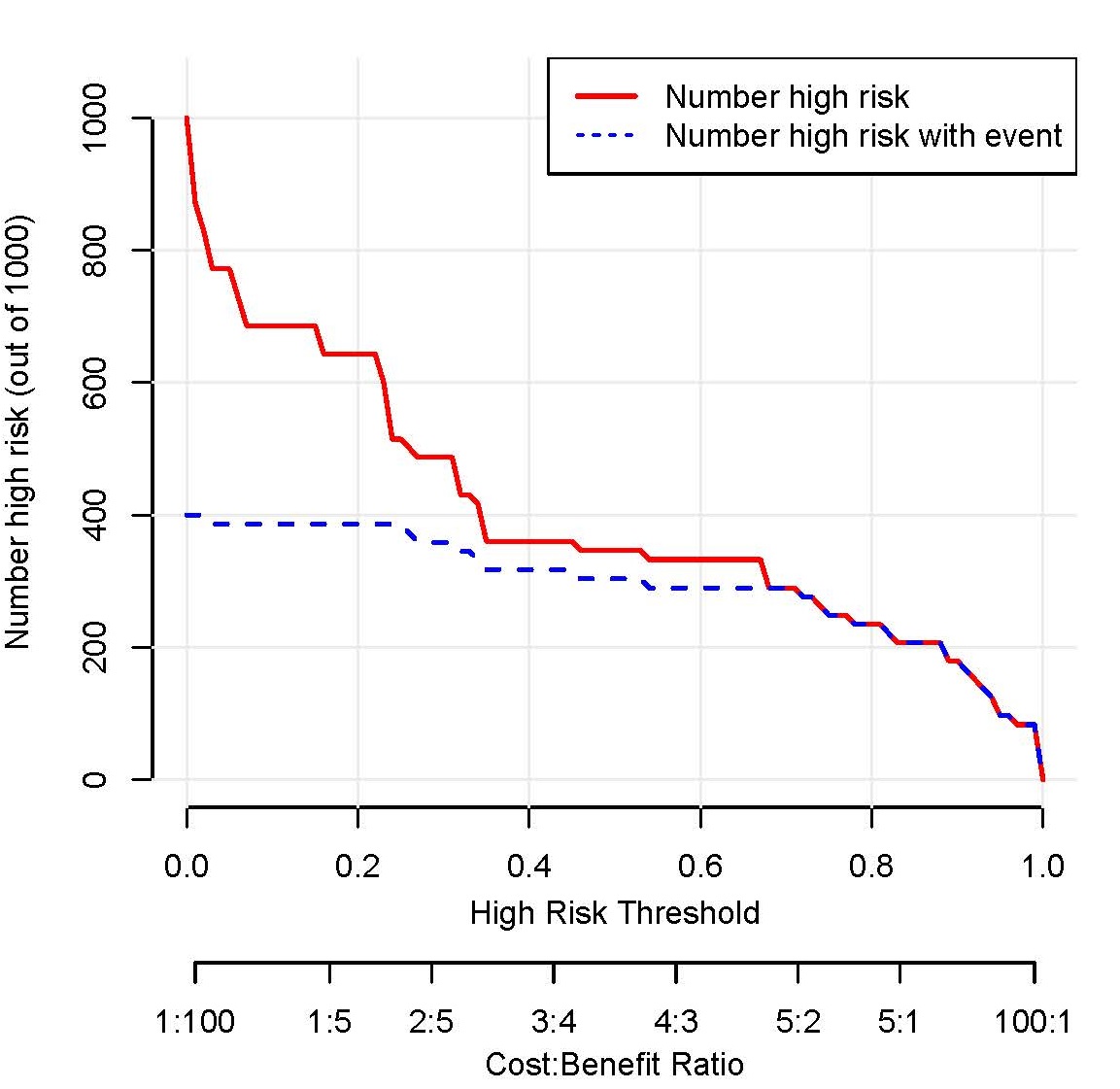
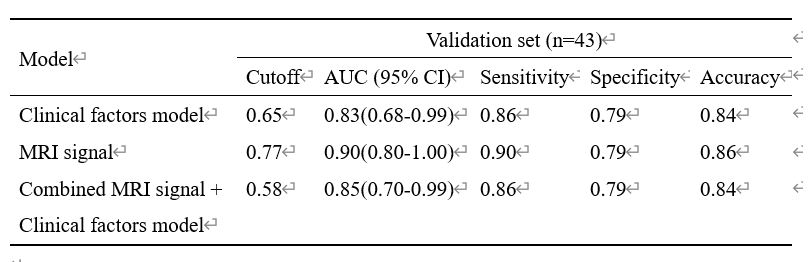
One hundred and forty-four patients (117 men, 25 women, mean age, 56.3 years; age range, 28–83 years) met the inclusion criteria, with a total of 35 HCAs and 109 WDHCCs. In the training set, most of the indexes (23/37) included in this study were significantly different between HCAs and WDHCCs. Moreover, 10 parameters remained significant after the univariate regression analysis. To construct a highly accurate predictive model, the significant parameters were further subjected to a multivariate regression model. Six valuable factors (long axis, T1WI, T2WI/FS, capsule enhancement, septa, and cirrhosis) were selected to establish the diagnostic model. Then, a nomogram (Fig. 1) to discriminate HCA from WDHCC was built on the basis of a multivariate logistic regression model. Fig. 2 indicates the AUC of the MRI signal model, the clinical factors model, and the combined model of MRI and clinical factors in training sets and validation sets are 0.955, 0.929, 0.962, and 0.898, 0.835, 0.846, respectively. DCA (Fig. 3) and clinical impact curve (Fig. 4) was applied to assess the clinical utility of the diagnostic nomogram. Based on the DCA, the MRI signal provided a greater net benefit than both the clinical factors model and the combined model of MRI and clinical factors. MRI signal-based model with a threshold of 0.77 provided the highest diagnostic performance with AUC was 0.90 (95% confidence interval 0.80–1.00) (90% sensitivity, 79% specificity, and 86% accuracy) to differentiate HCAs from WDHCCs (Table 1).Discussion
The distinction of HCA from WDHCC can be difficult in some cases, because of similar imaging characteristics and histopathological features, and pose significant diagnostic issues (3,4). As HCA is difficult to discriminate from WDHCC, it is important to have markers to identify high-risk adenomas. The differentiation between HCA with benign or malignant characteristics is important to define the treatment and surveillance strategy, because of the risk of disease progression. For this reason, a case of HCA with atypical characteristics raises doubts and difficulties about the nature of the tumor, with treatment implications. HCC developing from HCA is thought to behave less aggressively and the long-term prognosis for HCA with malignant transformation who undergo resection is generally good, and recurrence is uncommon (5). Beta-catenin, GPC-3, and HSP-70 are promising markers to identify higher-risk adenomas. Therefore, all HCAs must be discussed at multidisciplinary liver tumor boards that include specialized radiologists, pathologists, and hepatologists to determine the most suitable patient-oriented treatment strategy.Conclusion
MRI signal-based model provides high diagnostic performance as demonstrated in quantitative and qualitative analysis in the differentiation of HCA and WDHCC, supported by a nomogram model.Acknowledgements
This study is funded by the National Natural Science Foundation of China (82102029).References
1.Renzulli M, Clemente A, Tovoli F, Cappabianca S, Bolondi L, Golfieri R. Hepatocellular adenoma: An unsolved diagnostic enigma. World J Gastroenterol. 2019 May 28;25(20):2442-2449.
2.Kim TH, Woo S, Ebrahimzadeh S, McInnes MDF, Gerst SR, Do RK. Hepatic Adenoma Subtypes on Hepatobiliary Phase of Gadoxetic Acid-Enhanced MRI: Systematic Review and Meta-Analysis. AJR Am J Roentgenol. 2023 Jan;220(1):28-38.
3.Stoot JH, Coelen RJ, De Jong MC, Dejong CH. Malignant transformation of hepatocellular adenomas into hepatocellular carcinomas: a systematic review including more than 1600 adenoma cases. HPB (Oxford). 2010 Oct;12(8):509-22.
4. Choi WT, Kakar S. Atypical Hepatocellular Neoplasms: Review of Clinical, Morphologic, Immunohistochemical, Molecular, and Cytogenetic Features. Adv Anat Pathol. 2018 Jul;25(4):254-262.
5.Dokmak S, Paradis V, Vilgrain V, Sauvanet A, Farges O, Valla D, Bedossa P, Belghiti J. A single-center surgical experience of 122 patients with single and multiple hepatocellular adenomas. Gastroenterology. 2009 Nov;137(5):1698-705.
Figures