3989
Reduced Field of View Diffusion MRI for Rectal Cancer Response Assessment after Short Course Radiation and FOLFOXIRI1Radiology, Stanford University, Stanford, CA, United States, 2Radiation Oncology, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Treatment Response, Diffusion/other diffusion imaging techniques, Rectal Cancer
Motivation: Rectal cancer response assessment utilizes primarily T2 weighted and diffusion MRI. Reduced field of view diffusion has been shown to have higher imaqe quality and resolution than traditional EPI-based diffusion.
Goal(s): We compare reduced field of view diffusion to mrTRG and sigmoidoscopy for assessment of clinical response.
Approach: 32 patient MRI were evaluated after treatment with short course radiation (30 Gy, 5 fractions), and FOLFOXIRI and assessed with mrTRG system, ADC on reduced field of view DWI, and sigmoidoscopy.
Results: Reduced field of view diffusion is highly accurate for assessment of clinical response nearly matching the performance of mrTRG and surpassing sigmoidoscopy.
Impact: Reduced field of view diffusion should be considered for use in clinical protocols assessing rectal cancer treatment response along with T2 weighted MRI and clinical assessment.
Introduction
Rectal Cancer MRI provides tumor size, location, and involvement of nearby structures for tumor staging1. This information guides treatment planning, including decisions about surgery, radiation therapy, and chemotherapy. Neoadjuvant therapy, which includes chemotherapy and radiation therapy administered before surgery, is often used to shrink tumors, improve surgical outcomes, and recently has been used for organ preservation and avoid surgery in some patients2,3. MRI response is assessed with T2 weighted fast spin echo images and diffusion weighted MRI. Reduced field of view diffusion MRI has been shown to have higher image quality in rectal cancer but it has not been assessed for accuracy of treatment response assessment after treatment with short course radiation and FOLFOXIRI chemotherapy4,5.Methods
Clinical Trial: 37 patients with T2N0 or higher stage rectal cancer were recruited for a trial of organ preservation after short course radiation (30 Gy in 5 fractions) and 4 months of FOLFOXIRI. 5 patients were excluded from the current analysis due to no post treatment MRI, or early treatment failure due to no response to treatment after short course radiation and first chemotherapy cycle. MRI Acquisition: MRI performed pre-treatment, mid-treatment after radiation and 1 cycle of chemotherapy and after completion of all treatment. 3T MRI (GE or Siemens): 2D FSE T2w, 288 x 288 matrix, 18 cm FOV, 3 mm slice thickness, no spacing. DWI MRI with reduced field-of-view, 6 mm slice thickness, acquired b50, b800, synthetic b1500. 3D SPGR with Dixon based fat water separation pre and post contrast, 4 dynamic phases. Delayed phase acquisition acquired at 3 minutes post contrast injection using 3D SPGR with fat saturation (custom written sequence for GE scanners with optimized data sampling for rapid acquisition, Starvibe for Siemens). Patient microenema, 50-150 mL rectal gel placed based on tumor location and IV glucagon prior to axial T2 imaging to reduce peristalsis. MRI and Clinical Assessment: MRI reviewed by 2 radiologists (9 and 16 years experience) in consensus to assess treatment response using the mrTRG system and repeat TNM staging informed by diffusion and post contrast imaging. Sigmoidoscopy and visual assessment was made (grade 1 complete response, 2 near complete, 3 partial or stable response, and 4 progressive disease). Complete clinical response was defined as mrTRG 1 or 2, no residual tumor on direct visualization or negative biopsy, and no palpable tumor on exam. MRI Analysis: Average ADC was measured for a 3 mm round ROI in the center of the tumor or treated tumor area on post treatment MRI by a radiologist with 6 years experience. Statistical Analysis: Two sample T-test (Welch) was used to compared average ADC of patients with complete clinical response to incomplete response at the time of primary outcome assessment (POA) or the MRI prior to surgery. The sensitive, specificity, and accuracy of assessment for response was compared with complete clinical response for mrTRG (mrTRG 1 and 2 considered response, mrTRG 3, 4 and 5 considered persistent tumor), ADC (ADC > 1.1 considered response and ADC < 1.1 considered persistent tumor), and sigmoidoscopy (Grade 1 and 2 considered complete response, 3 & 4 persistent tumor)Results
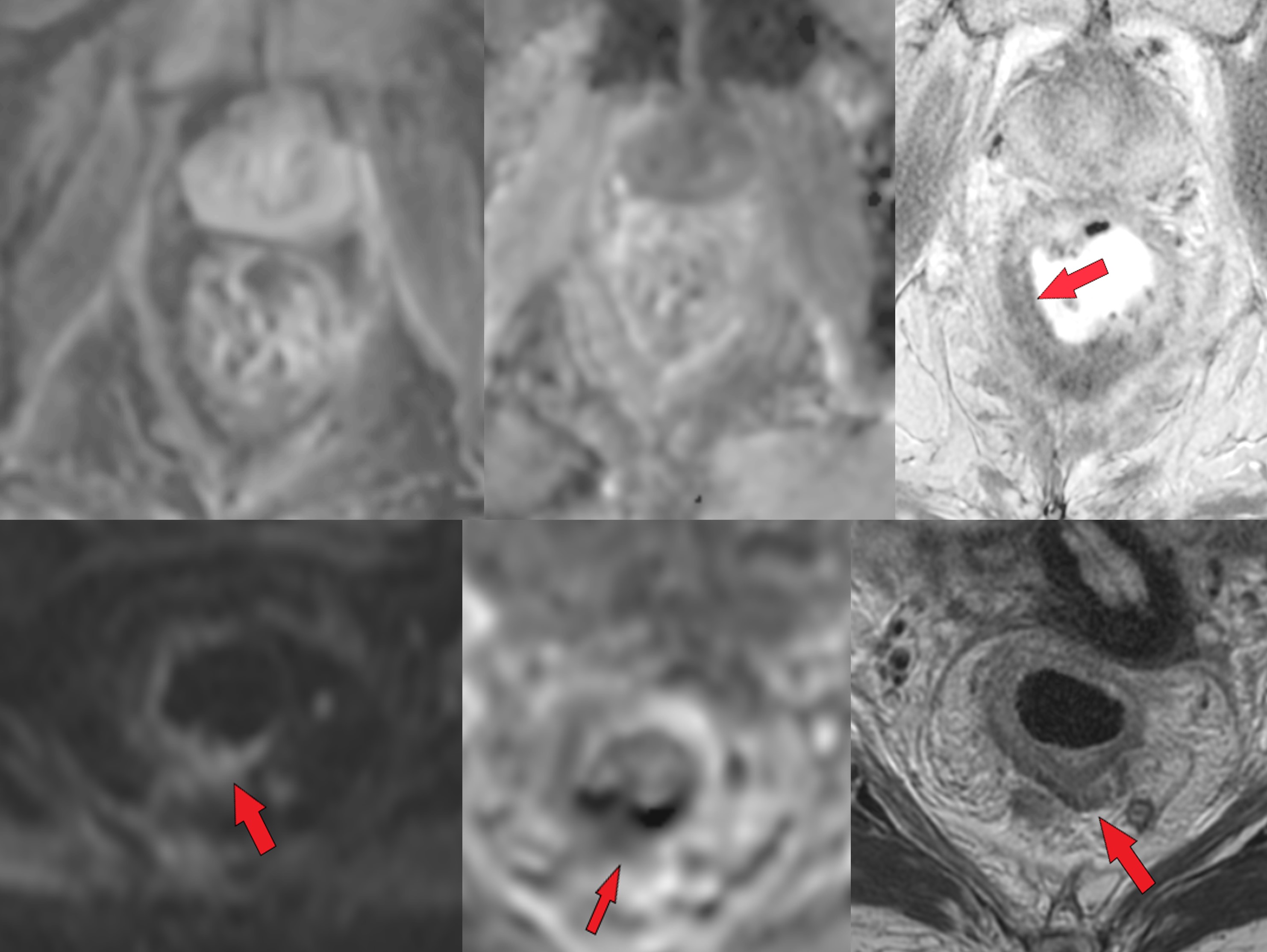
There was a difference in ADC (p=0.005) on MRI at time of POA or prior to surgery with the average in the patients with clinical response ADCavg = 0.95 (n=9) and without response ADCavg = 1.5 (n =23). For ADC cutoff of 1.2, 9 patients had predicted CCR (ADC >1.2) and 23 patients no CCR (ADC < 1.2), sensitivity of 89%, specificity 91% and accuracy of 91%. With mrTRG (1 or 2 was considered complete response, mrTRG > 3 is considered incomplete response), sensitivity was 100%, specificity was 100%, and accuracy was 97%. With flexible sigmoidoscopy where grade 1 and 2 were considered clinical response (3 and 4 considered incomplete/no response), the sensitivity was 47.6% (10/21), specificity 77.8% (7/9), and accuracy 56.7% (17/30). Figure 1 shows an example of complete clinical response versus no complete clinical response.Discussion
This is the first study of assessment of tumor response after short course radiation and FOLFOXIRI neoadjuvant chemotherapy with reduced field of view diffusion MRI. Previously studies have shown reduced field of view diffusion has higher image quality but not assessed or compared accuracy of response assessment. We found that an ADC cutoff of 1.2 had high sensitivity, specificity, and accuracy for response assessment nearly matching the mrTRG grading and exceeding direct visualization with sigmoidoscopy.Acknowledgements
No acknowledgement found.References
1.Patel, U. B. et al. MRI After Treatment of Locally Advanced Rectal Cancer: How to Report Tumor Response—The MERCURY Experience. American Journal of Roentgenology 199, W486–W495 (2012). 2. Garcia-Aguilar, J. et al. Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy. J Clin Oncol 40, 2546–2556 (2022). 3. Fokas, E. et al. International consensus recommendations on key outcome measures for organ preservation after (chemo)radiotherapy in patients with rectal cancer. Nat Rev Clin Oncol 18, 805–816 (2021). 4. Jang, S., Lee, J. M., Yoon, J. H. & Bae, J. S. Reduced field-of-view versus full field-of-view diffusion-weighted imaging for the evaluation of complete response to neoadjuvant chemoradiotherapy in patients with locally advanced rectal cancer. Abdom Radiol (NY) 46, 1468–1477 (2021). 5. Peng, Y. et al. Histological grades of rectal cancer: whole-volume histogram analysis of apparent diffusion coefficient based on reduced field-of-view diffusion-weighted imaging. Quant Imaging Med Surg 10, 243–256 (2020).Figures