3985
The prognostic value of amide proton transfer-weighted and intravoxel incoherent motion imaging for rectal adenocarcinoma.1Affiliated Hospital of Guizhou Medical univeristy, Guiyang, China, 2Philips Healthcare, Shanghai, China, 3Philips Healthcare, Xi’an, China
Synopsis
Keywords: Cancer, Body, rectal cancer
Motivation: To improve the accuracy of rectal cancer staging via imaging techniques.
Goal(s): To explore the correlation between amide proton transfer (APT) imaging, intravoxel incoherent motion imaging (IVIM) quantitative parameters, and the pathological traits and prognostic markers of rectal adenocarcinoma.
Approach: Standard Magnetic resonance imaging (MRI), APT, and IVIM scans were performed on patients with suspected rectal cancer. Following this, APT and IVIM quantitative parameters were derived.
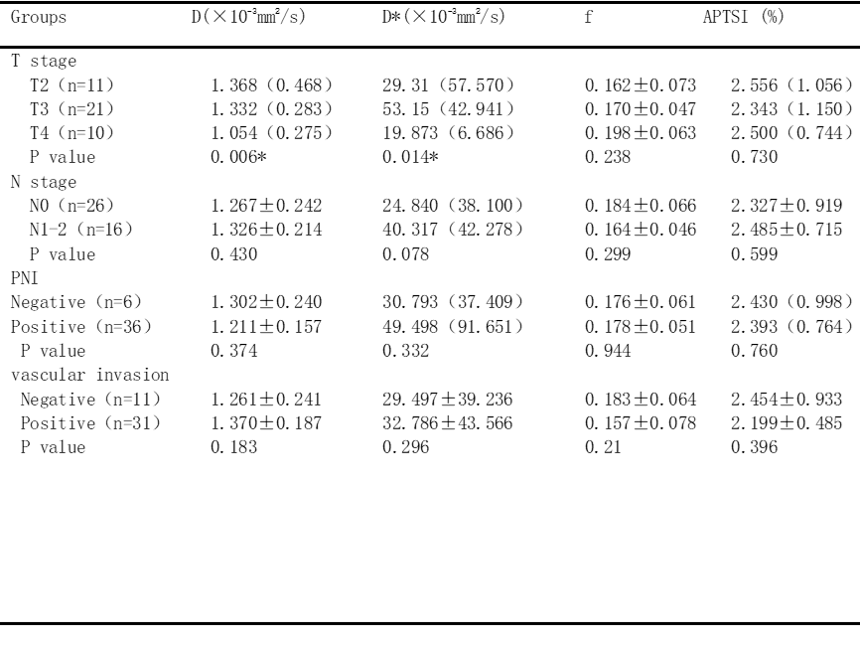
Results: Significant differences in D and D* values were observed across various T stages. However, no substantial variations in APT signal intensity (APTSI), D, D*, f were noted in different N stages, perineural invasion, and vascular invasion.
Impact: The research conducted has significant implications for the clinical staging of rectal cancer. By providing a more detailed and nuanced understanding of the disease's progression, it can aid in developing more precise and individualized treatment plans.
Introduction,Methods,Results,Discussion,Conclusion
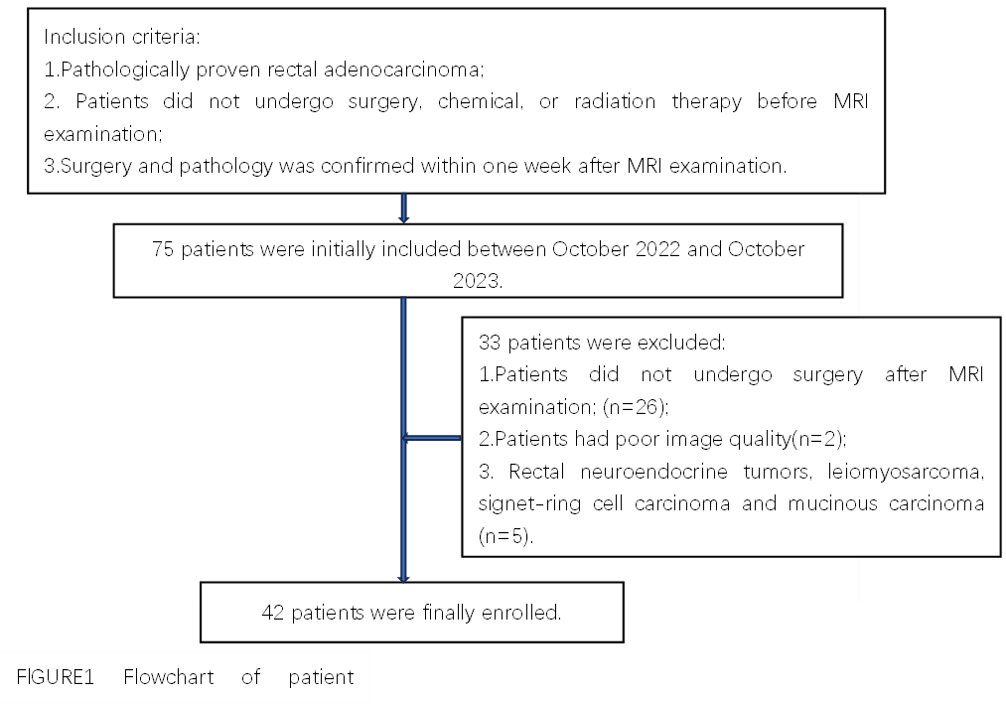
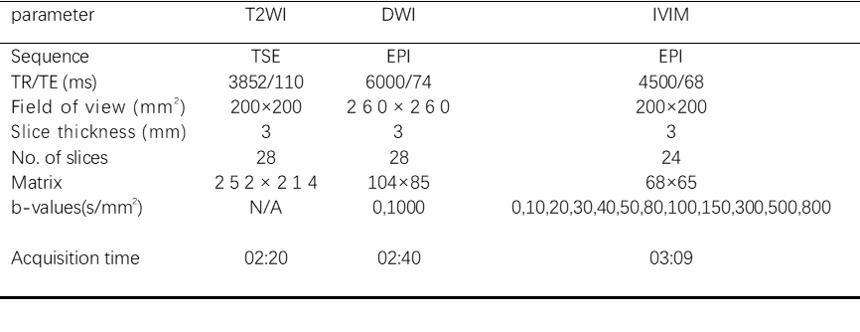
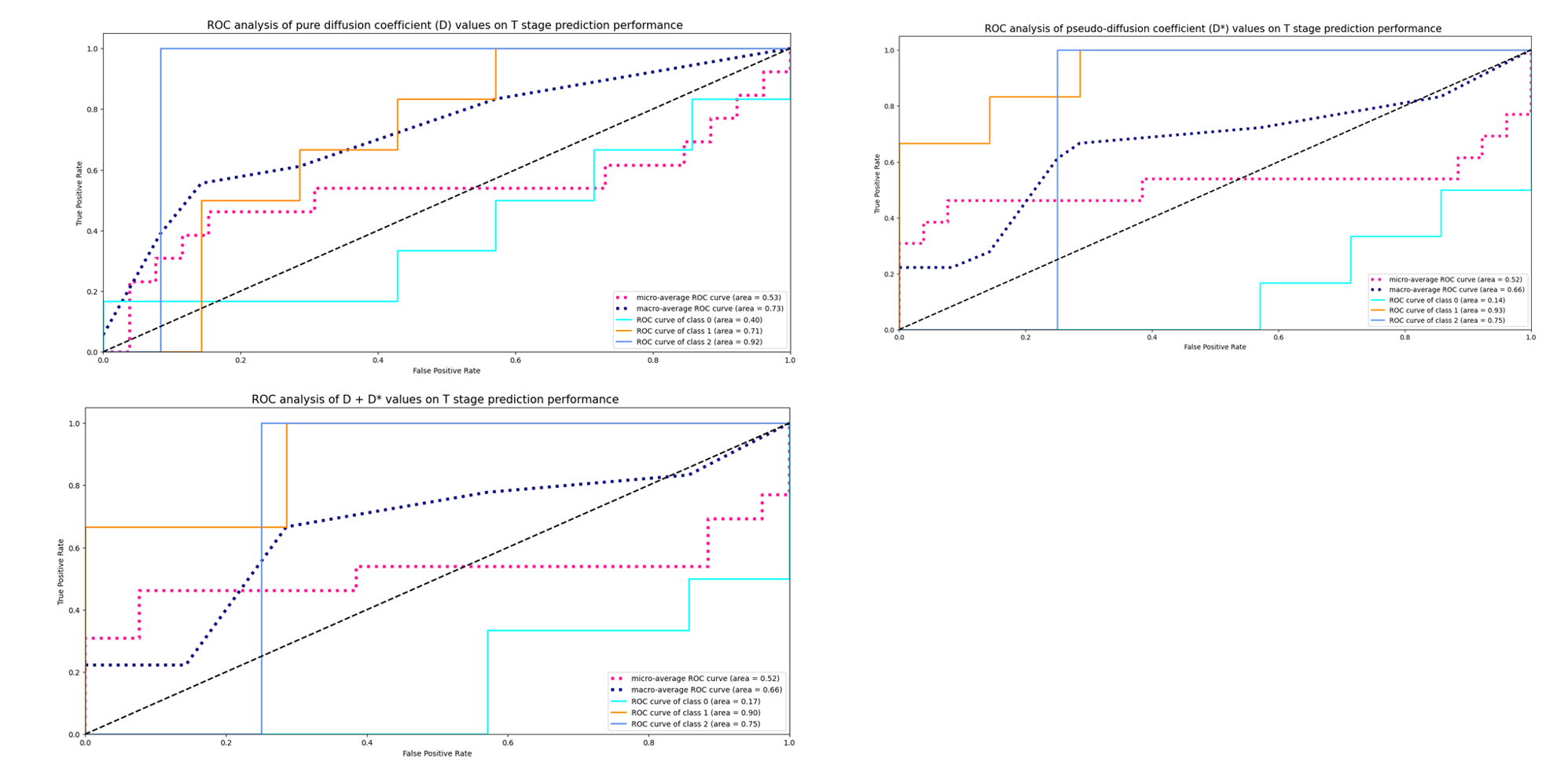
Introduction: As the most common gastrointestinal malignancy, rectal cancer poses a significant threat to human health 1. The multidisciplinary treatment approach for rectal cancer involves local resection or total mesenterectomy for early tumors and preoperative chemoradiotherapy (CRT) for advanced tumors, resulting in a reduction in the rate of local recurrence and distant metastasis. However, accurate preoperative tumor staging based on imaging remains crucial for making precise decisions 2。Key prognostic indicators for rectal cancer include T and N stages, peripheral vascular invasion, and pathological differentiation 3 .This study aims to investigate the correlation between amide proton transfer (APT) imaging, intravoxel incoherent motion imaging (IVIM) quantitative parameters, and the pathological traits and prognostic markers of rectal adenocarcinoma.Methods: A total of 75 patients with suspected rectal cancer (Figure 1) underwent conventional MRI, APT, and IVIM scans on a 3T scanner (Elition, Philips Healthcare, Best, the Netherlands) with a 32-channel phased array coil. The APT and IVIM quantitative parameters were obtained (Table 2). The pure diffusion coefficient (D), pseudo-diffusion coefficient (D*), perfusion fraction (f), and APTSI values were independently measured by two observers. Intra-class correlation coefficients (ICC) were used to test the consistency of measurements by the two observers. Independent-samples T test/Mann-Whitney U test, F test/Kruskal-Wallis H test was performed to analyze the difference of each parameter in different TN stages, perineural invasion, and vascular invasion. Spearman’s rank correlation was applied to depict the correlation of each parameter with risk stratification. The Bonferroni method was used to compare the statistically significant indicators between each group (P<0.05). Receiver operating characteristic (ROC) curves were used to evaluate the diagnostic efficacy, and the corresponding area under the curves (AUCs) was calculated. Results: Significant differences were observed in D and D* values among different T stages of cancer (P < 0.05). The D values showed significant differences between T4 and both T2 and T3 stages, while the D* values showed significant differences between T4 and T3 stages. However, no significant differences were found in APT SI, D, D*, and f values across different T stages, N stages, perineural invasion, and vascular invasion. Detailed results are shown in Tables 2. The D value was mildly negatively correlated with the T stage, but no significant correlation was observed between tumor T stage and D*, f, and APTSI values. According to the ROC curves, the D values had the highest diagnostic performance for the T4 stage, while D* values were most diagnostic for the T3 stage. The AUCs for D values for T2, T3, T4 stages were 0.40, 0.71, and 0.92 respectively, and for D* values were 0.14, 0.93, and 0.75 respectively. In summary, the D value was most effective in diagnosing the T4 stage, while the D* value was most effective for the T3 stage (Figure 3).
Discussion: This study found no significant differences in Amide Proton Transfer (APT) parameters among different tumor stages or between pN1-2 and pN0 stages in rectal adenocarcinoma. This contradicts previous studies, which found higher APT SI in advanced stages and lymph node metastasis4, 5. However, these studies excluded T4 stage cases and had higher lymph node metastasis rates, potentially causing selection bias. Our results align with Sun et al.'s 6 findings of decreasing D and D* with increasing tumor stages. Extramural venous invasion (EMVI) is a risk factor for poor outcomes in rectal cancer 7. Our study found no significant difference in APT and IVIM parameters in EMVI involvement, contradicting Chen W et al.'s findings 8 of higher APTSI values in EMVI-positive rectal adenocarcinoma. The discrepancy could be due to differing EMVI positive rates and methods of region of interest (ROI) selection and patient sampling. Our study considered tumor heterogeneity by placing ROIs on three different slices for analysis. This study likely underestimates tumor heterogeneity. We found no significant difference in APT and IVIM parameters between groups with and without perineural invasion (PNI), aligning with previous researchy9. This could be because the tumor microenvironment, as reflected by APT or IVIM parameters, doesn't significantly impact perineural infiltration.
Conclusion: D and D* values can be utilized to discriminate T stages, and the incorporation of D with D* values could enhance the diagnostic performance. In summary, IVIM proved to be beneficial in evaluating the prognostic factors associated with rectal adenocarcinoma.
Acknowledgements
NoneReferences
1. Ao, W.; Zhang, X.; Yao, X.; Zhu, X.; Deng, S.; Feng, J., Preoperative prediction of extramural venous invasion in rectal cancer by dynamic contrast-enhanced and diffusion weighted MRI: a preliminary study. BMC Med Imaging 2022, 22 (1), 78.
2. Hou, M.; Sun, J. H., Emerging applications of radiomics in rectal cancer: State of the art and future perspectives. World J Gastroenterol 2021, 27 (25), 3802-3814.
3. Wilkinson, N., Management of Rectal Cancer. Surg Clin North Am 2020, 100 (3), 615-628.
4. Chen, W.; Li, L.; Yan, Z.; Hu, S.; Feng, J.; Liu, G.; Liu, B.; Liu, X., Three-dimension amide proton transfer MRI of rectal adenocarcinoma: correlation with pathologic prognostic factors and comparison with diffusion kurtosis imaging. Eur Radiol 2021, 31 (5), 3286-3296.
5. Li, L.; Chen, W.; Yan, Z.; Feng, J.; Hu, S.; Liu, B.; Liu, X., Comparative Analysis of Amide Proton Transfer MRI and Diffusion-Weighted Imaging in Assessing p53 and Ki-67 Expression of Rectal Adenocarcinoma. J Magn Reson Imaging 2020, 52 (5), 1487-1496.
6. Sun, H.; Xu, Y.; Song, A.; Shi, K.; Wang, W., Intravoxel Incoherent Motion MRI of Rectal Cancer: Correlation of Diffusion and Perfusion Characteristics With Prognostic Tumor Markers. AJR Am J Roentgenol 2018, 210 (4), W139-w147.
7. Zhao, L.; Liang, M.; Yang, Y.; Zhang, H.; Zhao, X., Prediction of false-negative extramural venous invasion in patients with rectal cancer using multiple mathematical models of diffusion-weighted imaging. Eur J Radiol 2021, 139, 109731.
8. Chen, W.; Liu, G.; Chen, J.; Wei, Q.; Ye, Y.; Du, X.; Feng, J.; Yan, Z.; Deng, K.; Liu, X., Whole-tumor amide proton transfer-weighted imaging histogram analysis to predict pathological extramural venous invasion in rectal adenocarcinoma: a preliminary study. Eur Radiol 2023, 33 (7), 5159-5171.
9. Li, J.; Lin, L.; Gao, X.; Li, S.; Cheng, J., Amide Proton Transfer Weighted and Intravoxel Incoherent Motion Imaging in Evaluation of Prognostic Factors for Rectal Adenocarcinoma. Front Oncol 2022, 11, 783544.
Figures