3984
Predictive value of DCE-MR perfusion parameters for microsatellite instability in colorectal cancer1Gansu provincial hospital, lanzhou, China, 2Philips Healthcare, Xi’an, China, 3Gansu University of chinese medicine, Lanzhou, China
Synopsis
Keywords: Cancer, Tumor, colorectal cancer; microsatellite instability,DCE-MR, perfusion parameters,ADC
Motivation: To find an imaging method that can evaluate microsatellite status of colorectal cancer (CRC).
Goal(s): To investigate the value of DCE-MR perfusion parameters and ADC in predicting microsatellite instability of CRC.
Approach: DCE-MR perfusion parameters, including Ktrans, Ve, kep, iAUC and ADC were compared between microsatellite instability (MSI) and microsatellite stability (MSS) CRC groups. Receiver operating characteristics (ROC) curve was drawn to evaluate diagnostic efficacy.
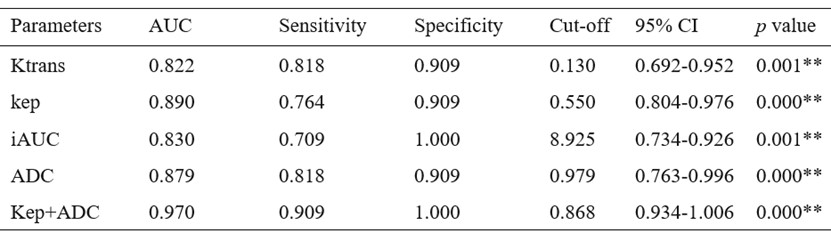
Results: Univariable analysis revealed that kep had highest diagnostic accuracy (AUC, 0.890; sensitivity, 76.4%; specificity, 90.9%). The diagnostic accuracy of kep combined ADC was the greatest in multivariable analysis (AUC, 0.970; sensitivity, 90.0%; specificity, 100%).
Impact: The combination of DCE-MRI based kep value and DWI based ADC value can provide excellent diagnostic accuracy in non-invasively predicting microsatellite status. This study provides insight into potential application of multi-modality MRI in predicting patient with CRC.
Introduction
Microsatellite instability (MSI) is a key element determining the efficacy of immunotherapy in colorectal cancer (CRC)[1,2] . Biopsy pathology is limited in its ability to comprehensively reflect the MSI status and heterogeneity of CRC[3] . Therefore, it is useful to develop a MRI-based approach to preoperatively predict MSI status. However, there has been few studies investigated the feasibility of dynamic contrast-enhanced magnetic resonance imaging (DCE-MR) and diffusion weighted imaging (DWI) to predict microsatellite status. This study aims to investigate the use of DCE-MR perfusion parameters and ADC values in distinguishing microsatellite instability (MSI) from microsatellite stability (MSS).Materials and Methods
In this prospective study, 11 MSI CRC patients and 55 MSS CRC patients (38 males, 28 females; aged 60.62 ± 12.29 years; ranged 22–83 years) were enrolled in our study. The Human Research Ethics Committee of Gansu Provincial Hospital approved the study, and all participants gave informed written consent in accordance with the Helsinki Declaration. Data were collected using two 3.0T MR scanners (Philips Ingenia Elition; Siemens Megnetom Skyra) with phased-array multi-channel coils. T1-weighted DCE-MR sequence parameters were as follows: TR=5.08ms, TE=1.77ms, slice thickness=3.5mm, number of total images=200, acquisition time per slice=0.36 sec, total scan time=284 sec; FOV=260mm. The scan commenced immediately after intravenous administration of a contrast agent at a rate of 3.5 mL/s, with a dose of 0.2 mL/kg of body weight, followed by a 20 mL saline flush using an automatic power injector through the antecubital vein. For DWI sequence, the b-value was set to 0 and 1000s/mm2. All data obtained from the DCE sequences were sent to the Tissue 4D post-processing workstation (Siemens AG) for post-processing, the system automatically generated perfusion images. ADC maps were generated from DWI data. Two abdominal radiologists, each with more than 8 years of experience in interpreting colorectal images draw the regions of interest (ROI) along the high signal intensity border of the tumor on both perfusion images and ADC maps, respectively. The intraclass correlation coefficient (ICC) was used to find the inter-observer reproducibility of the measurements. The calculated DCE parameters were Ktrans (contrast transfer constant, influenced by vascular permeability and leakage space), Ve (fractional volume of the extracellular- extra vascular space (EES)), kep (reflux rate between EES and blood plasma) and iAUC (initial area under the curve, reflecting both perfusion and permeability). The averaged value was used for subsequent analysis. DNA was extracted from 66 CRC patients to detect Microsatellite status. Statistical analysis was performed using SPSS 27.0 and MedCalc software package. The Shapiro-Wilk test was used to check normality. Normally distributed data were analyzed by Student’s t-test, non-normally distributed data were analyzed by Mann-Whitney U test, P<0.05 was regarded as statistically significant. The significant DCE-MR parameters were combined by logistic regression to improve the diagnostic capabilities. The receiver operating characteristic (ROC) analysis was used to compare diagnostic capabilities. Multivariate logistic regression was used to establish a combined model based on DCE-MRI parameter with the greatest diagnostic performance and ADC, and its diagnostic efficacy was evaluated.Results
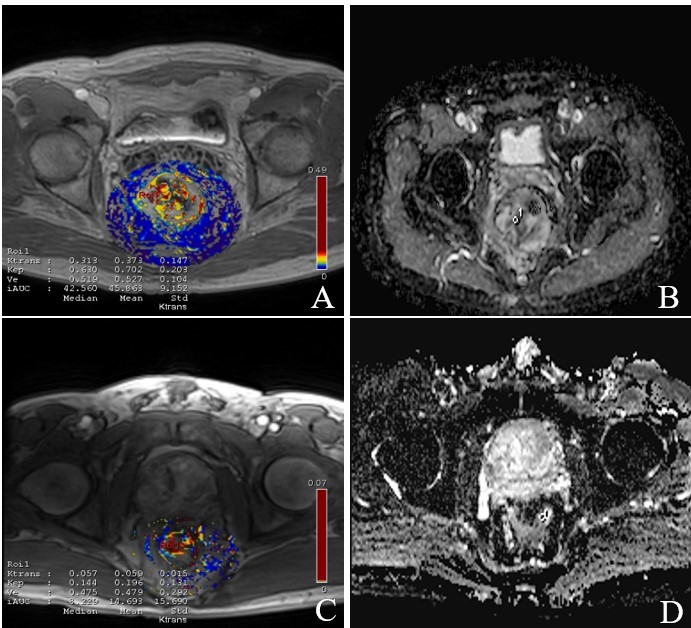
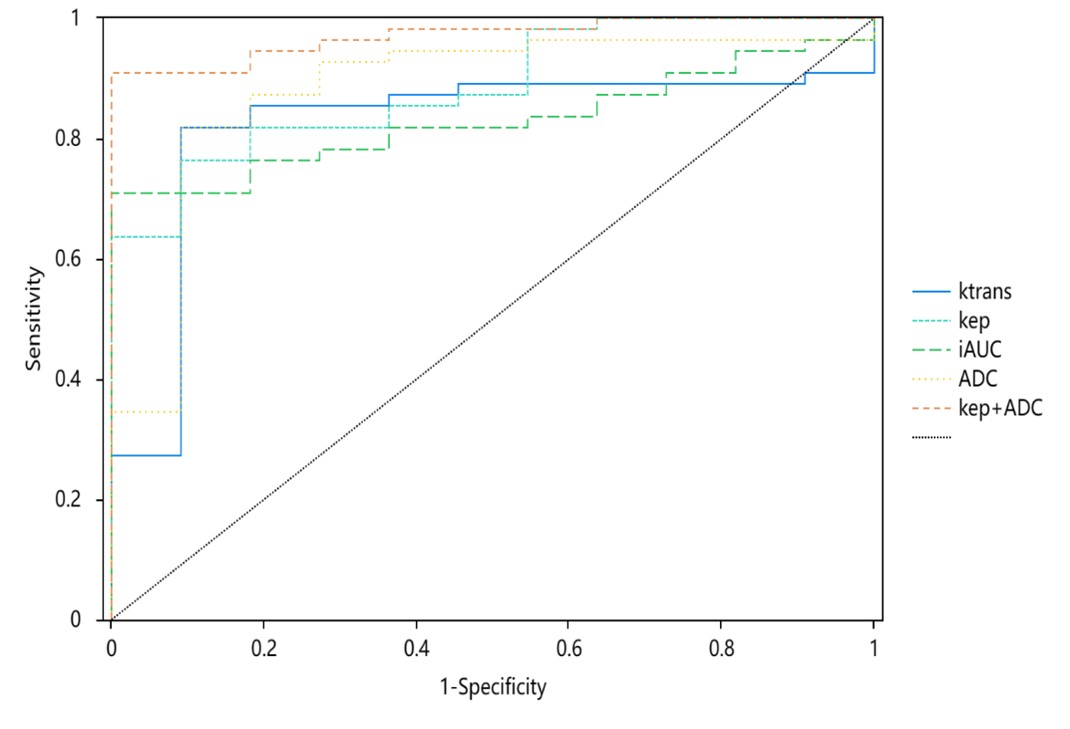
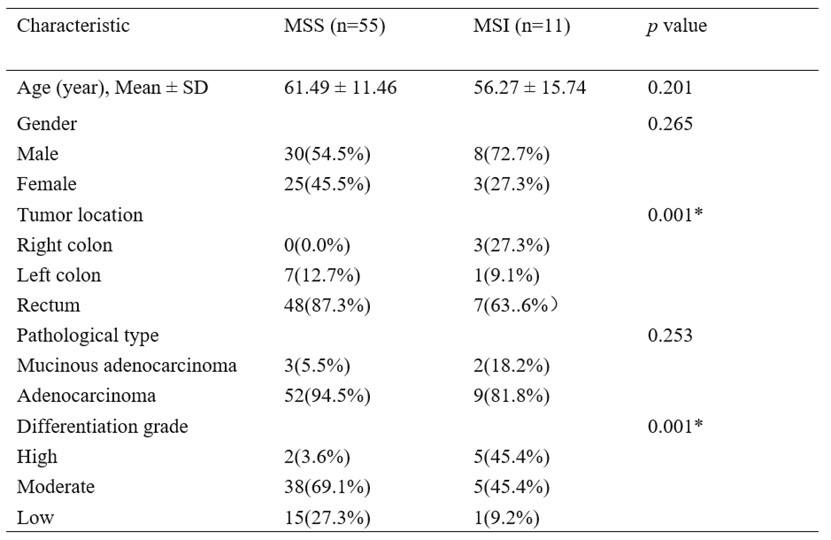
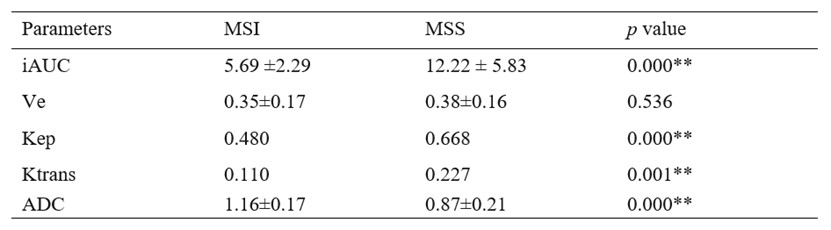
Demographic characteristics were shown in Table 1. Figure 1 showed a representative example of MSS and MSI patients. There was good agreement (ICC = 0.90) between the two radiologists. As can be seen from table 2, Ktrans, kep and iAUC of MSI group were significantly lower than those of MSS group (all P<0.05), ADC was significantly higher than that in MSS group (P<0.001), while Ve of MSI group had no statistical difference with MSS group (P=0.536). The AUC of kep in predicting colorectal cancer MSI was 0.890, which was higher than those of Ktrans, iAUC and ADC (AUC=0.822, 0.830, 0.879, Z=3.456, 3.173, 3.170, all P<0.001). The AUC of Kep+ADC was 0.970, which was higher than those of Kep and ADC alone (Z=6.171, 3.978, both P<0.001). Those results were shown in table 3, figure 2.Discussion
Our study revealed that kep had good diagnostic accuracy for predicting microsatellite status (AUC, 0.890; sensitivity, 76.4%; specificity, 90.9%). The diagnostic accuracy of kep combined ADC was the greatest in multivariable analysis (AUC, 0.934; sensitivity, 90.90%; specificity, 100%). Perfusion parameter kep, the reverse rate constant, reflects the rate at which the contrast agent transfers from the extravascular-extracellular space (EES) back to the blood[4,5,6,7,8] . It reflects the blood supply and actual tumor capillary permeability, and can accurately reflect the tumor microvascular environment.Conclusion
DCE-MRI perfusion parameters especially kep could effectively predict MSI of colorectal cancer. The combination of kep and ADC demonstrates the excellent predictive performance, enabling non-invasive and early evaluation of microsatellite status, thus providing better guidance for immunotherapy in patients with CRC.Acknowledgements
No acknowledgement found.References
[1] WANG Q, XU J, WANG A, et al. Systematic review of machine learning‑based radiomics approach for predicting microsatellite instability status in colorectal cancer[J]. Radiol Med, 2023,128(2):136-148.
[2] CHALABI M, FANCHI L F, DIJKSTRA K K, et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-profcient and MMR-defcient early-stage colon cancers[J]. Nat Med, 2020,26(4):566-576.
[3] ERIKSSON J, AMONKAR M, Al-JASSAR G, et al. Mismatch repair/microsatellite instability testing practices among US physicians treating patients with advanced/metastatic colorectal cancer[J]. J Clin Med, 2019,8(4):558.
[4] KRISHAN S, PATEL A, SUD R, et al. Rectal perfusion parameters normalised to tumour-free rectal wall can predict response to neoadjuvant chemoradiotherapy[J]. Clin Radiol, 2018,73(2):151-157.
[5] Koo HR, Cho N, Song IC, et al., Correlation of perfusion parameters on dynamic contrast-enhanced MRI with prognostic factors and subtypes of breast cancers, J Magn Reson Imaging, 36(2012), 145–151.
[6] Yeo DM, Oh SN, Jung CK, et al., Correlation of dynamic contrast-enhanced MRI perfusion parameters with angiogenesis and biologic aggressiveness of rectal cancer: Preliminary results, J Magn Reson Imaging, 41(2015) ,474-480.
[7] Shen FU, Lu J, Chen L, et al., Diagnostic value of dynamic contrast-enhanced magnetic resonance imaging in rectal cancer and its correlation with tumor differentiation, Mol Clin Oncol, 4(2016) ,500-506.
[8] Krishan S, Patel A, Sud R, et al., Rectal perfusion parameters normalised to tumour-free rectal wall can predict response to neoadjuvant chemoradiotherapy, Clin Radiol, 73(2) (2018), 151-157.
Figures