3983
Correlation of Amide Proton Transfer Magnetic Resonance Imaging with Prognostic Factors in Rectal Adenocarcinoma1Department of Radiology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer Center, Kunming, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Cancer, CEST & MT, Rectal Adenocarcinoma, APT, prognosis
Motivation: Improving the accuracy of imaging to assess prognostic factors in rectal adenocarcinoma.
Goal(s): Recognizing early rectal adenocarcinoma, assisting clinicians to achieve precision treatment.
Approach: Prospective enrollment of rectal adenocarcinoma patients without neoadjuvant therapy undergoing radical surgery for rectal cancer. Using their preoperative imaging data, investigate the correlation between APTw imaging and prognostic factors in rectal adenocarcinoma.
Results: APTw SI value are linked to T-stage and the presence of perineural invasion in rectal adenocarcinoma.
Impact: This study's results hold promise for the non-invasive identification of nerve invasion in rectal adenocarcinoma, offering a foundation for clinicians to pursue precise treatment strategies.
Introduction
While amide proton transfer (APT) imaging has proven valuable in characterizing brain tumors like gliomas [1-4], its potential utility in rectal adenocarcinoma remains underexplored. This study aims to establish the relationship between three-dimensional amide proton transfer magnetic resonance imaging parameters and prognostic factors in rectal adenocarcinoma. The goal is to enhance the precision of preoperative prognostic evaluation and provide an imaging foundation for tailored rectal cancer treatment.Methods
This Prospective study enrolled consecutive patients diagnosed with rectal adenocarcinoma who underwent direct radical rectal cancer surgery without prior neoadjuvant therapy between January 2022 and April 2023. Preoperative MR examination included APT-weighted imaging (APTw) and T1-weighted enhanced images (T1WI-C) (Figure 1). APTw signal intensity (SI) (%) was quantified as the percentage of magnetization transfer ratio asymmetry at a 3.5 ppm offset (MTRasym). Using ITK-SNAP 4.0 software, regions of interest were delineated based on APTw-T1WI-C images, and histogram data were computed. Prognostic factors for rectal adenocarcinoma were stratified by their prognostic characteristics. The APTw SI among different subgroups was compared using one-way ANOVA, Mann-Whitney U-test, or Kruskal-Wallis H-test (Table 1 and Table 2). The diagnostic performance of APTw in assessing prognostic factors was assessed via receiver operating characteristic (ROC) curve analysis.Results
A total of 217 consecutive patients were initially enrolled, with 47 patients (mean age 59 years, range 55 ~ 61 years) meeting the study’s inclusion and exclusion criteria. The area under the curve (AUC) for T-staging in rectal adenocarcinoma using APTw SI mean was 0.683 (95% CI: 0.52 ~ 0.82). The sensitivity and specificity were 86.96% and 50.0%, respectively, with a cutoff value of APTw SI mean ≥ 1.93% for indicating T3-T4 staging (see Figure 2a).The AUC for assessing perineural invasion in rectal adenocarcinoma using both APTw SI mean and APTw SI max was 0.679 (95% CI: 0.52 ~ 0.81), 0.730 (95% CI: 0.57 ~ 0.85), respectively. The sensitivity and specificity for APTw SI mean ≥3.24% (best cut-off value) in indicating perineural invasion were 42.86% and 97.22%, while the corresponding values for APTw SI max ≥3.75% (best cut-off value) were 100.0% and 38.9%. Combining APTw SI mean with APTw SI max to assess perineural invasion increased the AUC value to 0.778 (95% CI: 0,63 to 0.89) (see Figure 2b).
Discussion
While there are limited studies on the application of APTw imaging in rectal cancer, existing research has yielded inconsistent results. Moreover, most studies are retrospective and may suffer from selection bias, a limitation addressed by our prospective study to minimize sample bias. In our study, we found that APTw SI mean was higher in T3-4 stage tumors compared to T-2 stage, aligning with previous findings, such as those by liu[5], Additionally, we observed significant differences in APTw SI max and APTw SI mean between groups with and without perineural invasion (p < 0.05). This contrasts with the results of Cheng's study, which found no correlation between these variables[6].Our approach involved sketching ROIs directly in APTw and T1WI-C matching fusion images, overcoming the challenge of image matching and compensating for APT’s spatial resolution limitations. This difference in methodology might contribute to the discrepancies between our results and those of other studies.
Conclusion
Our study suggests that amide proton transfer imaging holds promise for the assessment of T-staging and perineural invasion in rectal adenocarcinoma. This has the potential to aid clinicians in delivering more precise and tailored treatments for patients.Acknowledgements
No acknowledgements found.References
1. Paech, D., et al., Relaxation-compensated amide proton transfer (APT) MRI signal intensity is associated with survival and progression in high-grade glioma patients. Eur Radiol, 2019. 29(9): p. 4957-4967.
2. Kamimura, K., et al., Amide proton transfer imaging of tumors: theory, clinical applications, pitfalls, and future directions. Jpn J Radiol, 2019. 37(2): p. 109-116.
3. Jiang, S., et al., Identifying Recurrent Malignant Glioma after Treatment Using Amide Proton Transfer-Weighted MR Imaging: A Validation Study with Image-Guided Stereotactic Biopsy. Clin Cancer Res, 2019. 25(2): p. 552-561.
4. da Silva, N.A., et al., Hybrid MR-PET of brain tumours using amino acid PET and chemical exchange saturation transfer MRI. Eur J Nucl Med Mol Imaging, 2018. 45(6): p. 1031-1040.
5. Chen, W., et al., Three-dimension amide proton transfer MRI of rectal adenocarcinoma: correlation with pathologic prognostic factors and comparison with diffusion kurtosis imaging. Eur Radiol, 2021. 31(5): p. 3286-3296.
6. Li, J., et al., Amide Proton Transfer Weighted and Intravoxel Incoherent Motion Imaging in Evaluation of Prognostic Factors for Rectal Adenocarcinoma. Front Oncol, 2021. 11: p. 783544.
Figures
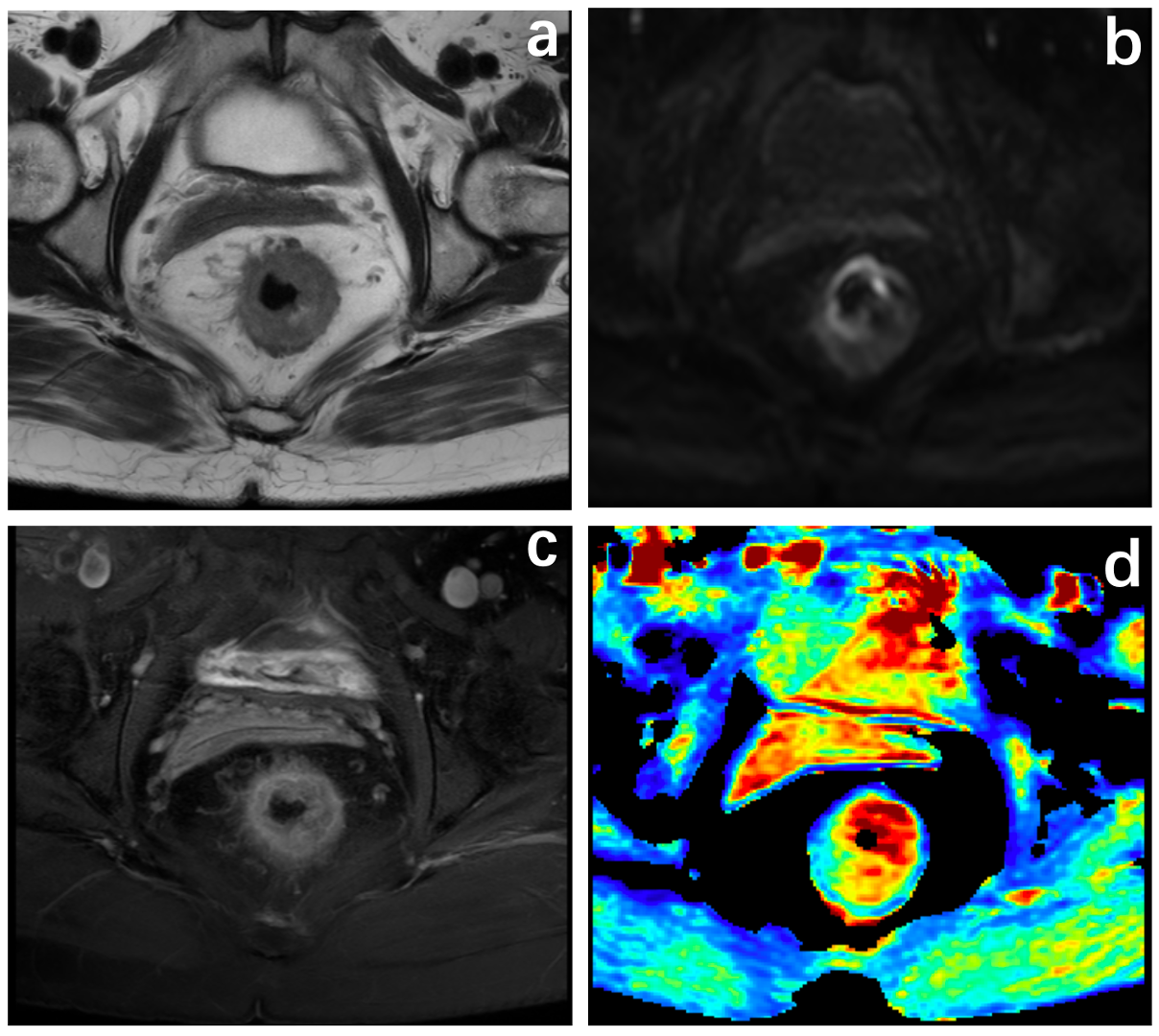
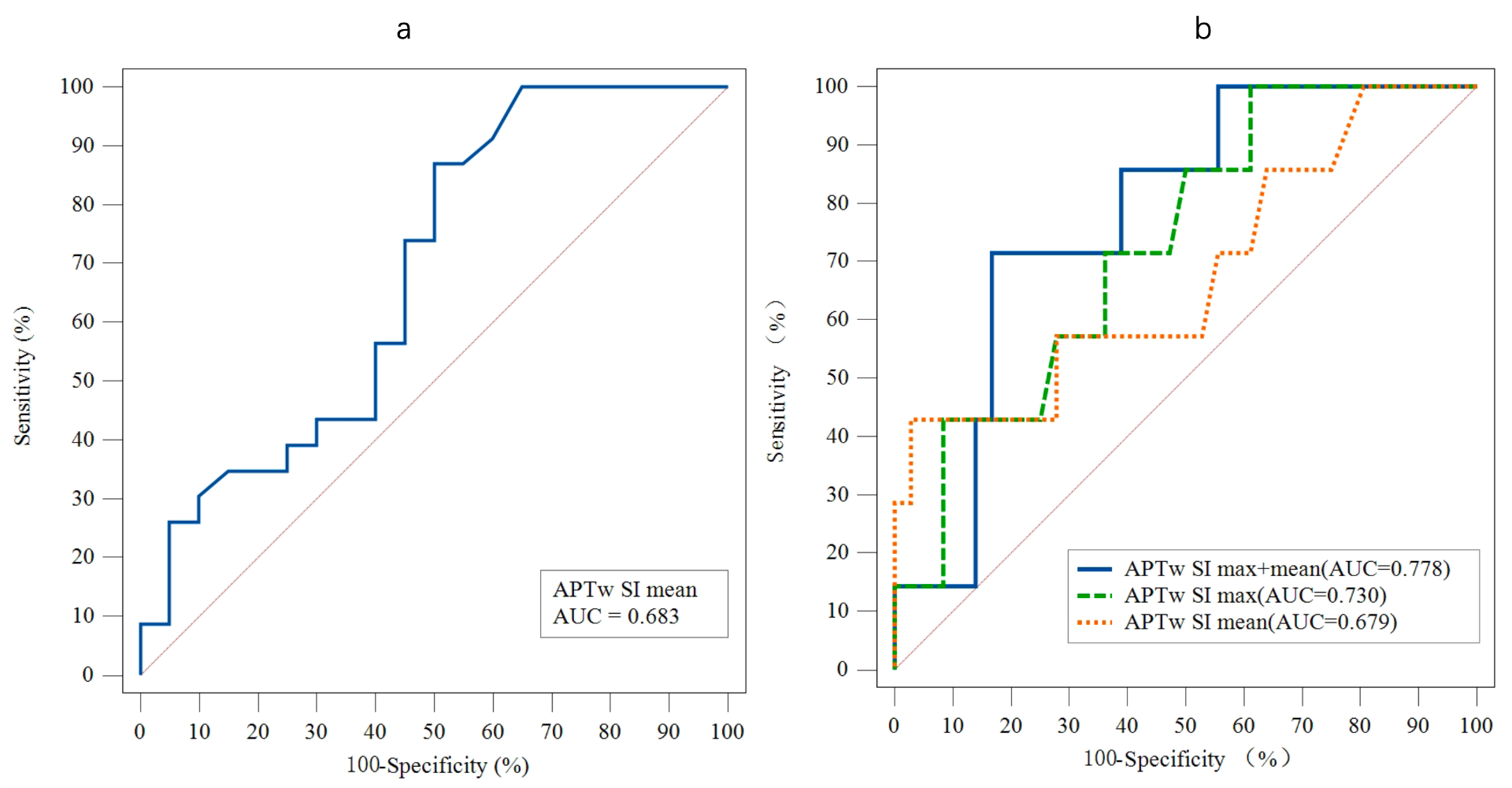
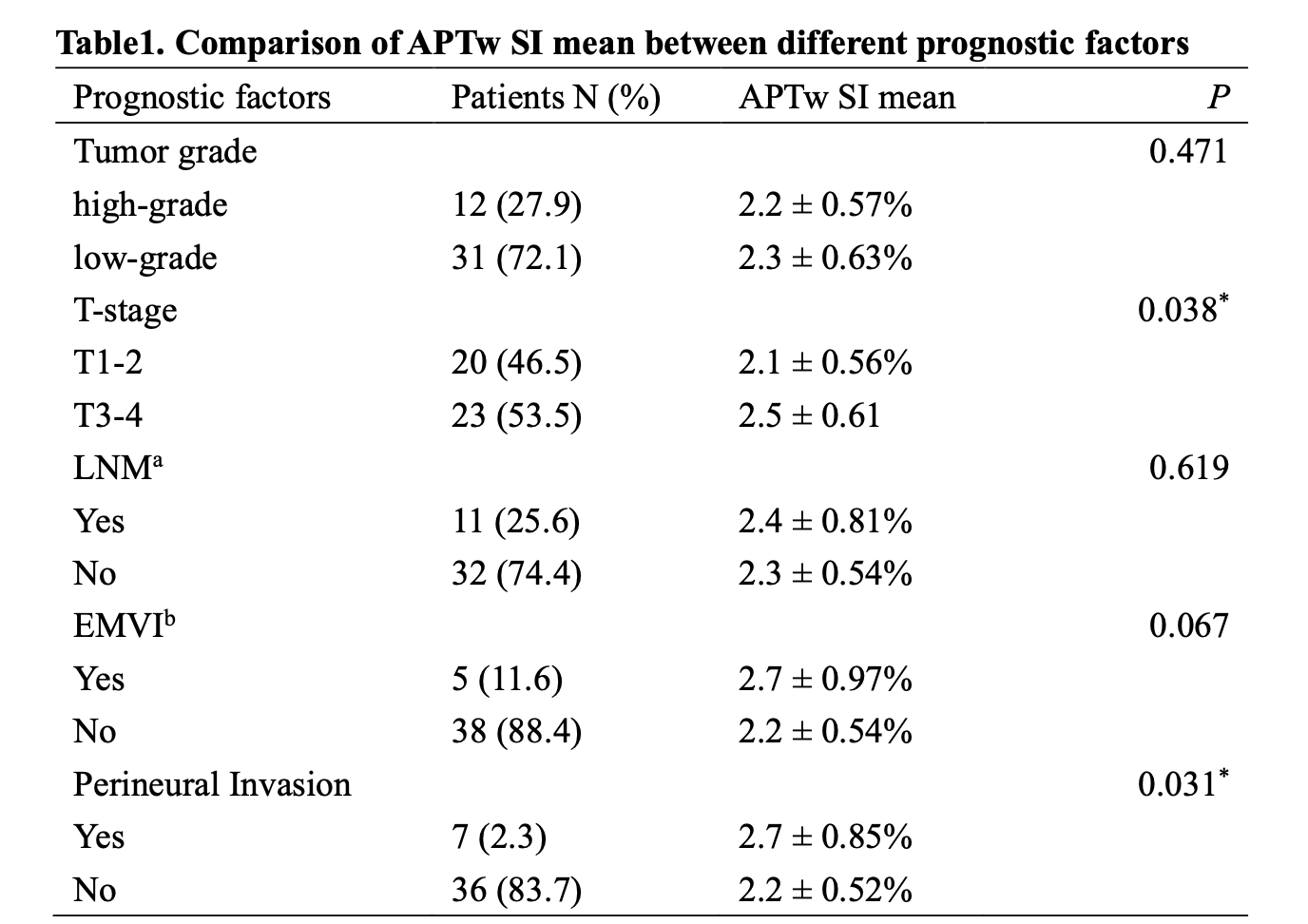
Table 1. Comparison of APTw SI mean between different prognostic factors.
Note: Measurements: normally distributed data are expressed as x ± s; skewed data are expressed as M (interquartile spacing). Count data are expressed as n (%).
*P<0.05 indicates statistically significant difference.
a: LNM:lymph node metastasis.
b: EMVI:Extramural vascular invasion.
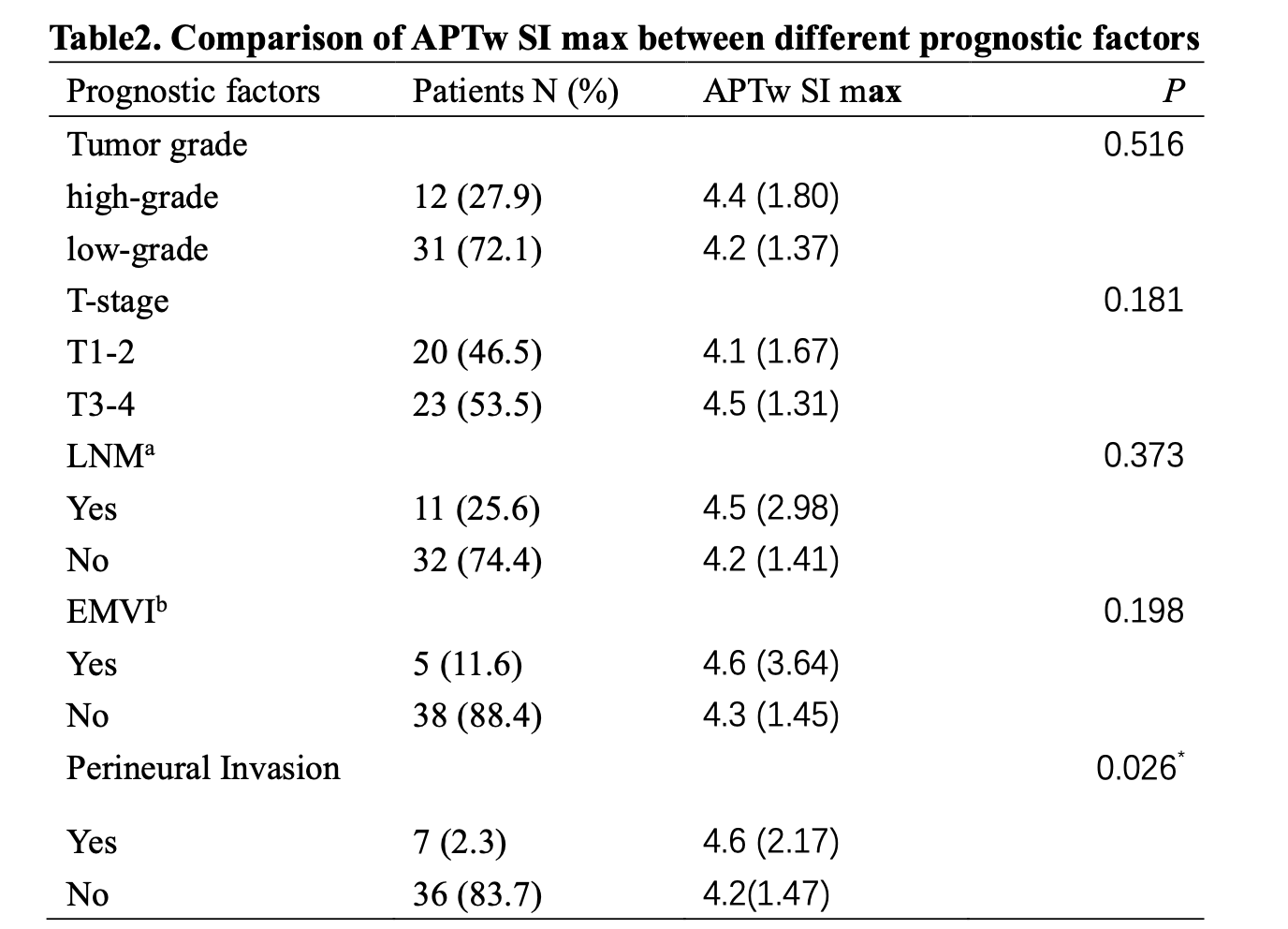
Table 2. Comparison of APTw SI max between different prognostic factors.
Note: Measurements: normally distributed data are expressed as x ± s; skewed data are expressed as M (interquartile spacing). Count data are expressed as n (%).
*P<0.05 indicates statistically significant difference.
a: LNM:lymph node metastasis.
b: EMVI:Extramural vascular invasion.