3978
Biomechanical phase angle as proxy to quantify the presence of microvascular invasion in hepatocellular carcinoma1U1148, INSERM, PARIS, France, 2Assistance Publique - Hôpitaux de Paris, Clichy, France, 3U1149, INSERM, PARIS, France, 4Biomaps, Saclay, France, 5King’s College London, London, United Kingdom
Synopsis
Keywords: Cancer, Elastography, Liver, microvascular invasion, biomechanics
Motivation: In hepatocellular carcinoma (HCC), microvascular invasion (MVI), an indicator for tumor aggressiveness, is identified typically through post-resection pathology examination. Currently, non-invasive methods for assessing tumor aggressiveness are lacking.
Goal(s): Our objective is to discover a non-invasive imaging biomarker for evaluating the presence/absence of MVI.
Approach: The alterations induced by the tumor, such as MVI, can modify the tissue architecture and, consequently, its mechanical properties. Magnetic resonance elastography at 40Hz was performed in 44 HCC patients who had liver resection.
Results: Peritumoral tissue phase angle accurately distinguish patients with/without MVI, indicative for aggressiveness. These results correlate with higher tumor differentiation in patients without MVI.
Impact: This clinical study introduces the phase angle as a new biomarker for gauging HCC aggressiveness whereby enabling patient stratification.
Introduction
Hepatocellular carcinoma (HCC) is a primary cancer whose high prevalence and late detection, despite numerous known risk factors, makes treatment difficult and leaves the patient with an associated unfavorable prognosis. Microvascular invasion (MVI), defined as the presence of tumor emboli in the vessels surrounding the tumor, is one of the main prognostic factors for clinical outcome. Currently, the only reliable way to determine the presence/absence of MVI is via histopathology performed on liver resection specimen. Tumoral cells, notably in MVI, can modify tissue biomechanics by releasing enzymes that degrade the extracellular matrix, provoking cellular rearrangements and inducing inflammatory responses [1]. Magnetic resonance elastography (MRE) is an emerging, non-invasive method for monitoring the biomechanical state of the liver and revealing underlying pathology by determining its shear modulus. The aim here is to use MRE to identify potential new biomarkers for characterizing the severity of HCC, with a view to improving patient management.Methods
44 patients underwent clinical MRI/research MRE prior to resection of their HCC. MRE was performed on a Philips 1.5T MRI using the gravitational liver transducer concept vibrating at 40Hz [2]. Acquisition was performed with a 3D expresso MRE sequence [3] using Hadamar encoding [4]. Three regions of interest were determined manually on the corresponding anatomical images: the tumor region itself, the peritumoral region, and a region characterizing distant non-tumoral liver tissue (Fig1). The corresponding biomechanical parameters obtained within these ROIs were: |G*|=sqrt(Gd2+Gl2), where Gd is the shear stiffness, Gl is the shear viscosity, and Y=2/π*atan(Gl/Gd) is the phase angle. Histopathological analysis was conducted on resected tumors from each patient using hematoxylin-eosin saffron staining on paraffin sections to identify the presence of MVI. Tumoral differentiation (well, moderate and poor, scored from 2 to 0 respectively) was performed according to the World Health Organization [5].Results
The correlation between the phase angle Y in the tumoral region and the peritumoral region is shown in Fig. 2A. Clearly, tumors with or without MVI populate different regions in this phase space. Tumors without MVI (blue dots, MVI-) are localized within a single cluster around Yperi~0.3 and Ytumor~0.35. On the contrary, tumors with MVI (MVI+, red dots) populate two distinct clusters which are mainly characterized by a lower peritumoral phase angle (Yperi~0.25) or a higher peritumoral phase angle (Yperi~0.35) compared to the MVI- cluster. However, this clustering is not found when the phase angle Y within distant non tumoral liver tissue is correlated to the Ytumor (Fig2B). This suggests that the peritumoral tissue is key determinant to distinguish the presence/absence of MVI non-invasively in patients. The phase angle differs between the two MVI+ clusters because the cluster at low Yperi~0.25 exhibits a stiffer peritumoral tissue (Gd) compared to the other cluster (Fig2C).For MVI- patients, tumor and peritumoral phase angle differ significantly (Fig3A), indicating a distinctively different viscoelastic behavior between these two tissues. However, for patients with MVI (MVI+), this difference vanished entirely for the cluster at high Yperi~0.35 (Fig3B,C), and was borderline statistically significant for the cluster at lower Yperi~0.25 (Fig3B,D). This shows that invasion is impacting biomechanical properties of the peritumoral zone, as expected, making it more “similar” to the tumor’s phase angle. Pathological analysis shows that tumor differentiation is increased in MVI- patient compared to MVI+ (Fig4). 82.4% of MVI- patients present moderate-well to well differentiated tumoral cells. This drops for the MVI+ group to 37.5% in the cluster with low Yperi~0.25 and to 33.3% in the cluster with high Yperi~0.35. This match between histopathology (i.e. degree of tumor differentiation) and difference/similarity in biomechanics between tumor and peritumoral region is reassuring.
Finally, when considering the stiffness |G*|, we do not observe any discernible distinction between MVI+ and MVI- patients, regardless of whether peritumoral tissue is correlated to tumoral tissue (Fig. 5A) or distant non tumoral liver tissue (Fig. 5B), contrary to previously published data [6]. These results underscore the superior discriminatory ability of the phase angle Y as a biomarker in identifying tumor aggressiveness.
Conclusions
The phase angle of peritumoral tissue seems to be a promising non-invasive biomarker for HCC patients to identify noninvasively patients with or without MVI. This result could help handling treatment decision for patient and avoid biopsy.Acknowledgements
This study received financial support by funding from the European Union's Horizon 2020 Societal Challenges - Health, Demographic Change and Well-Being Programme under grant agreement No 668039.References
[1] J Winkler et al., Nature Communications 11 (1), 5120 (2020)
[2] Runge et al., Phys Med Biol. 64 (4), 045007 (2019)
[3] P Garteiser et al., NMR in biomedicine 26 (10), 1326 (2013)
[4] C Guenthner et al., NMR in biomedicine 31 (5), e3908 (2018)
[5] Bosman et al., WHO Classification of Tumours of the digestive system (2010)
[6] H Abe et al., Surgery 170 (1), 167 (2021)
Figures
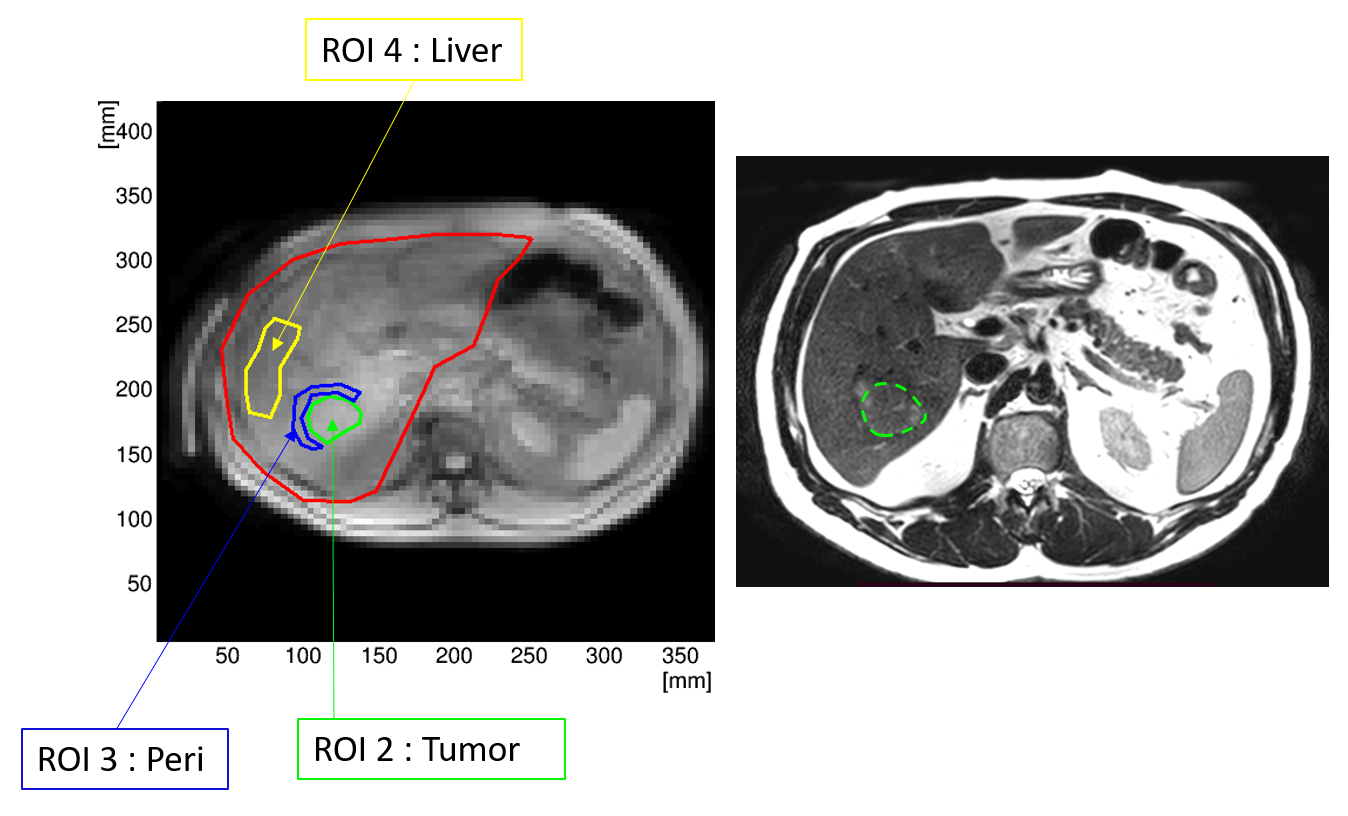
Figure 1: Anatomical image of an HCC patient’s liver. A: magnitude image showing the different regions of interest (ROI): green the ROI for the tumor, blue the ROI for the peritumoral tissue (peri), and yellow ROI for the distant non tumoral part of the liver (liver). B: Corresponding T2 weighted image with tumor located within the green ROI.
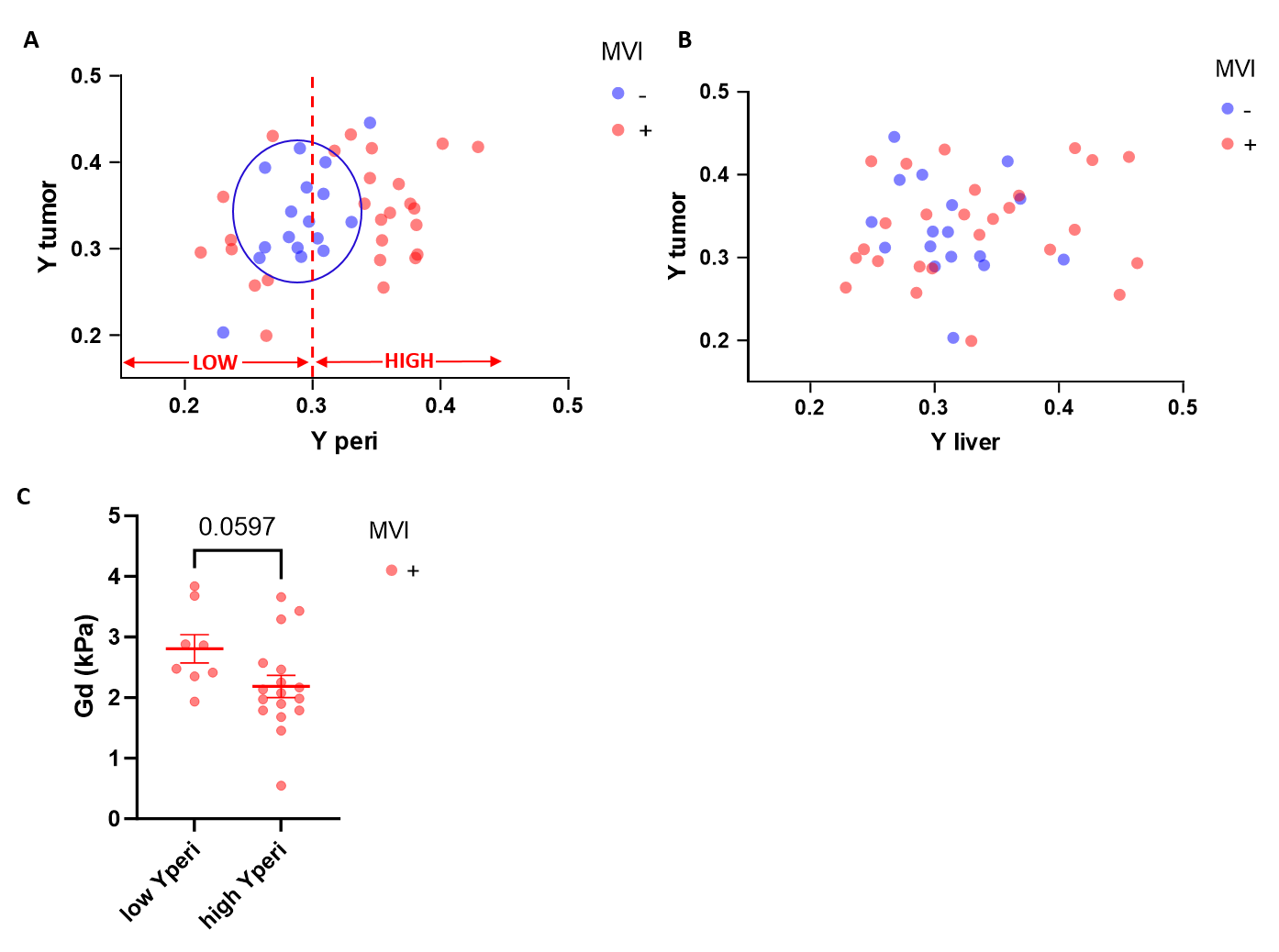
Figure 2: Y phase angle as possible biomarker for identifying patients with or without MVI. A: The correlation of Ytumor with Yperi distinguishes MVI- (blue dots) from MVI+ (red dots) patients. The MVI+ cluster is separated into 2 populations, one with low Yperi and one with high Yperi . B: This clustering of patients is not observed when Y from distant non tumoral liver tissue is considered. C: Variation in Y for the two MVI+ clusters is explained by a stiffer peritumoral tissue for the group with a lower Yperi. Mind that if Gd rises, the phase angle drops if Gl is almost constant.
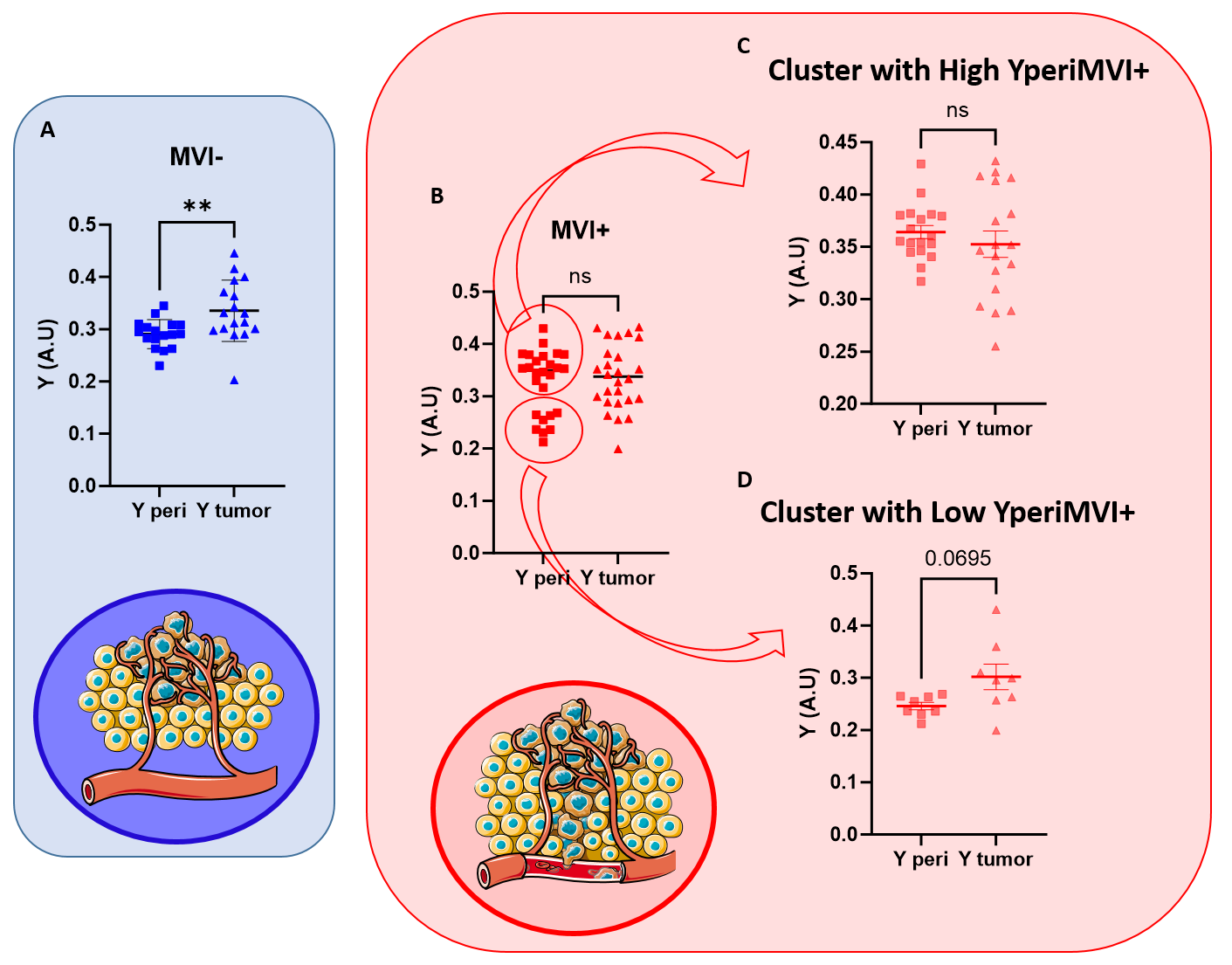
Figure 3: Tissue biomechanics for patients with or without MVI. A: Comparison of the phase angle between Yperi and Ytumor shows a significant difference for MVI- patients indicating a highly distinct biomechanical profile between these two tissues. B: However, MVI+ patients show and opposite behaviour. C: Patients with a high Yperi appear to have similar biomechanical properties in both peritumoral and tumoral tissues, whereas (D) patients with a low Yperi show intermediate variations between these two tissues.
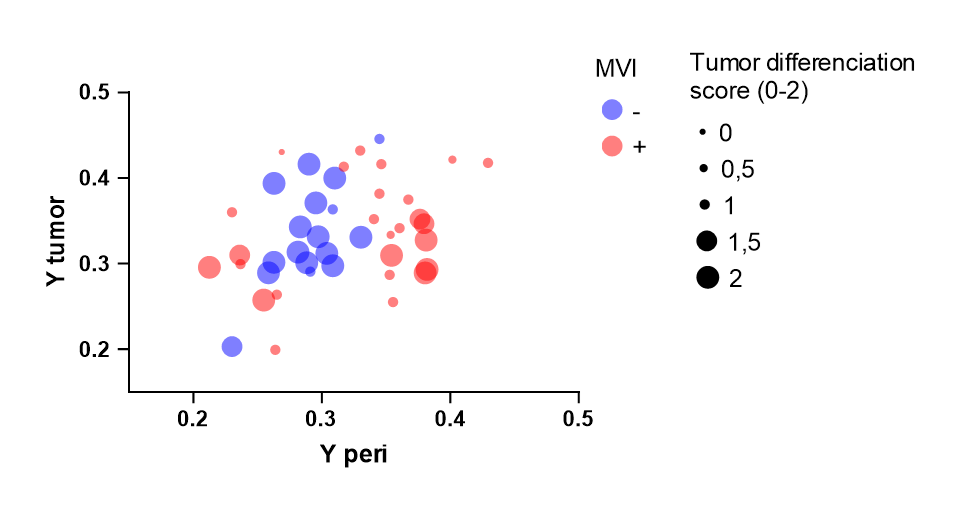
Figure 4: Tumor differentiation evaluation, by hematoxylin-eosin saffron, shows that MVI- patients are exhibiting well and moderate-well differentiation, while MVI+ patients show all poorer differentiation with lower scores (≤1).
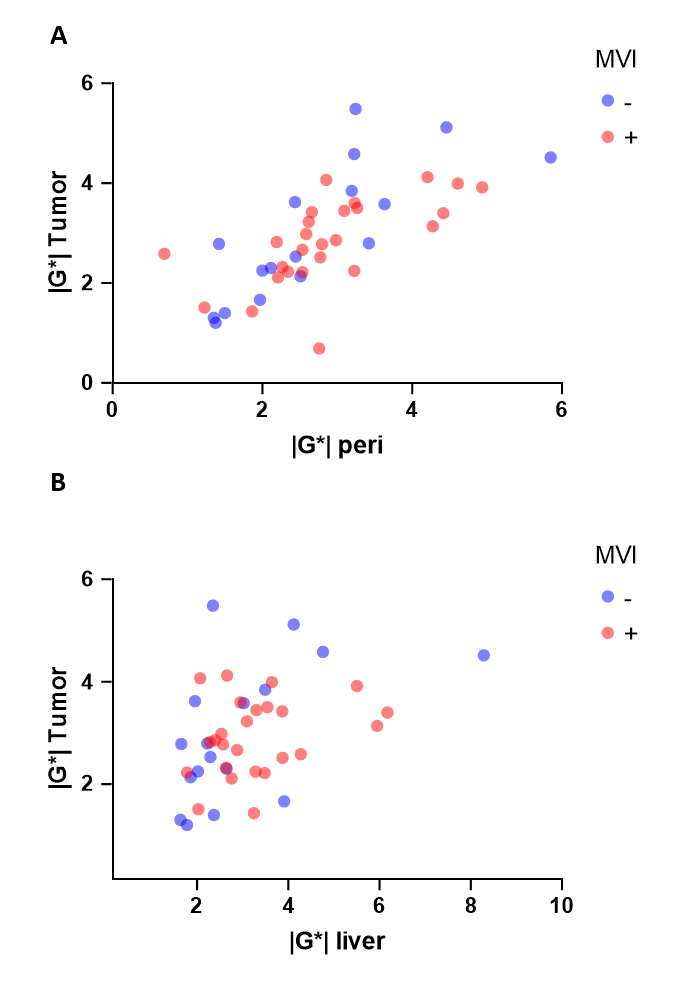
Figure 5: Stiffness |G*| does not seem to be a biomarker for MVI. The correlation between tumor stiffness and (A) peri-tumoral tissue stiffness (or (B) distal non-tumor liver tissue) does not distinguish patients with or without MVI.