3973
IVIM perfusion parameters for non-invasive characterization and radionuclide response assessment in a neuroendocrine tumor model1Department of Medical Radiation Sciences, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, 2Department of medical physics and biomedical engineering, Sahlgrenska University Hospital, Region Västra Götaland, Gothenburg, Sweden
Synopsis
Keywords: Biomarkers, Cancer, Multiparametric, IVIM
Motivation: IVIM MRI potentially offers non-invasive, non-contrast-based quantification of tumor perfusion parameters, which would facilitate tumor tissue characterization and longitudinal assessment of radionuclide therapy.
Goal(s): The goal was to study the feasibility of using IVIM metrics for spatiotemporal tissue characterization in the context of radionuclide therapy in a neuroendocrine tumor model.
Approach: Mice with human neuroendocrine tumors were imaged before and repeatedly after radionuclide treatment and parametric maps of perfusion-related parameters from IVIM and DCE were compared and studied longitudinally.
Results: Interesting spatiotemporal variations that revealed similarities between techniques show promise for further in-depth analysis using spatial image registration techniques and histopathological validation.
Impact: Non-invasive, spatiotemporally resolved tumor perfusion characterization using intravoxel incoherent motion MRI would benefit preclinical optimization and understanding of radionuclide treatment with possible rapid translation into the clinics due to the widespread use of MRI in both research and clinical practice.
Introduction
Radionuclide treatment using 177Lu-octreotate is successful in patients with inoperable neuroendocrine tumors (NETs). However, cure is rare, and there are few biomarkers that can be used to optimize therapeutic response. The opportunity to characterize and follow tumor vascularization, angiogenesis and oxygenation is offered by perfusion imaging, such as dynamic contrast-enhanced (DCE1)- and intravoxel incoherent motion (IVIM2)-MRI. Visualizing perfusion parameters non-invasively and spatiotemporally would be valuable for understanding and optimising intra-tumor radionuclide distribution and therapeutic effects.3DCE-MRI can be used to estimate Ktrans (volume transfer constant of contrast agent (CA) from plasma to extracellular extravascular space (EES)) and ve and vp (fractional EES and plasma volume in tissue). DCE-MRI show promising results for characterizing tumor perfusion metrics, but CAs are problematic for patients with renal impairment, and there is evidence for brain CA deposition.4
IVIM-MRI is a non-CA-based alternative for perfusion imaging. The IVIM perfusion fraction (f) estimates the fraction of diffusion MRI signal attenuation related to perfused capillaries, and the product of f and the pseudo-diffusion (f×D*) has been correlated with blood flow.
The purpose of this study was to evaluate the feasibility of using IVIM perfusion metrics instead of DCE-MRI to characterize NETs and monitor 177Lu-octreotate response in an animal NET model.
Methods
MRI experiments (7T Bruker Biospec) were conducted on 12 nude mice with the subcutaneous human small-intestine neuroendocrine tumour GOT15. Experiments were repeated on days -1, 1, 3 and 8 relative to treatment day 0, when a sub-therapeutic amount (15MBq) 177Lu-octreotate was administered to achieve a range of responses. The study was approved by the Gothenburg Ethical Committee on Animal Research.Included 2D MRI techniques were IVIM-MRI: SE-EPI, 9-11 b-values (0-800s/mm2), gradient directions/separation/duration: 3/9ms/4ms, TR/TE: 1500/21ms, voxel size: 320x320x1000µm3; T1-mapping: RAREVTR, 7 TRs (300-13000ms), TE: 24ms, voxel size: 280x280x1000µm3; DCE-MRI: RARE, 200 dynamics (2.1ms temporal resolution), turbo factor: 4, TR/TE/echo-spacing: 300ms/12ms/12ms and tail vein CA injection during the 6th dynamic (0.3mmol/kg bodyweight, 0.1M gadolinium-DTPA); T2 RARE (for tumor volume measurement).
IVIM parameters were estimated using a Bayesian method with spatial prior distributions (https://github.com/oscarjalnefjord/ivim). T1 for each DCE dynamic was estimated from pre-contrast T1 (from RAREVTR) and the signal equation for a 2D RARE using dictionary-based method. Post-contrast T1 were converted to CA uptake using the expression r1C(τ) = ΔR1 =R1(τ)-R10, where C is the CA concentration, R1=T1-1, R10 pre-contrast longitudinal relaxation rate, τ dynamic number and r1=2.8s-1mM-1 the CA relaxivity 6. The extended Tofts model1 and a literature-based arterial input function7 were used to estimate Ktrans, ve and vp using QbiPy8.
Results
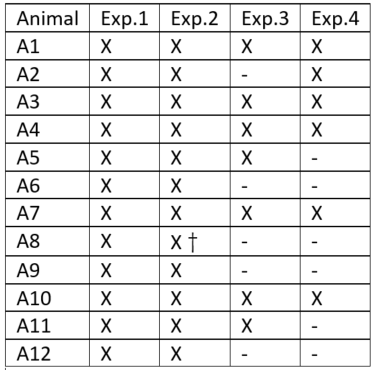
Apart from one animal (A8, died after Exp.2), the therapy was well tolerated, and response varied from good (reduced tumor volume) to poor (only slightly reduced growth rate) on follow-up (Fig.1). CA injections were, in general, successful with significant tumor signal enhancement, but sometimes failed e.g. due to clogging (summarized in Table 1).There was significant intra-tumor heterogeneity with longitudinal variations in most tumors and parameters, and local hot-spots/intra-tumor variations could be recognized both in IVIM and DCE-MRI parametric maps (compare, e.g., Ktrans and f in central tumor on Exp.1, Fig.2). Figures 2/3 show examples from a good/poor responder. An unexplained offset in the DCE-MRI signal on late dynamics obscured parameters for one tumor (A7) on Exp.3 (Fig.2).
On a group level, IVIM parameters tended to increase from Exp.1 to Exp.3 (mean±sd f and f×D* increased from 7.3±2.8 to 10.2±5.6 % and 1.1±0.8 to 1.9±2.3μm2/ms, respectively), but variations were too high to indicate statistical significance (not shown). Group mean DCE-MRI parameters did not reveal any temporal trends (Fig.4).
Discussion
Visual inspection of the parametric maps in this work reveals interesting intra-tumor heterogeneity that can be recognized/followed longitudinally (e.g. the increasing f in the top-left quadrant of A4 (Fig.3, Exp.1-4). The intra-tumor heterogeneity, however, also makes group-level analysis insensitive and challenging to interpret. We currently work with image registration to match DCE-MRI with IVIM images, which will allow us to conduct pixel-wise analysis of correlations between parameters and, thereby, better understand if IVIM could replace CA-based DCE-MRI as a tool to characterize and monitor perfusion-related parameters in our NET model.Conclusion
IVIM-derived perfusion parameters reveal interesting intra-tumor variations that can be non-invasively characterized over time. This shows promise for IVIM-MRI as a non-invasive and non-CA-based technique to characterize neuroendocrine tumor tissue and monitor response after 177Lu-octreotate treatment.Work based on spatial registration between images/parametric maps is currently undertaken, and will allow us to analyze the correlations with CA-based perfusion metrics, and thereby better understand the biological meaning an usefulness of IVIM perfusion data for tumor characterization and therapy response assessment.
Acknowledgements
The study was financed by grants from the Assar Gabrielsson Foundation, the Sahlgrenska University Hospital Research Fund, the Royal Society of Arts and Sciences in Gothenburg (KVVS), grants from the Swedish Cancer Society, the King Gustav V Jubilee Clinic Cancer Research Foundation and Lion's Cancer Research Fund of Western Sweden, and the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement
References
1. Tofts PS, Brix G, Buckley DL, et al. Estimating Kinetic Parameters From Dynamic Contrast-Enhanced T1-Weighted\tMRI of a Diffusable Tracer: Standardized Quantities and Symbols. J Magn Reson Imag 1999;10(July):223–232.
2. Le Bihan D, Breton E, Lallemand D, et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1988;168(2):497–505.
3. Forssell-Aronsson E, Spetz J, Ahlman H. Radionuclide therapy via SSTR: Future aspects from experimental animal studies. Neuroendocrinology 2013;97(1):86–98.
4. Shi C, Liu D, Xiao Z, et al. Monitoring tumor response to antivascular therapy using non-contrast intravoxel incoherent motion diffusion-weighted MRI. Cancer Res. 2017;77(13):3491–3501.
5. Kölby L, Bernhardt P, Ahlman H, et al. A Transplantable Human Carcinoid as Model for Somatostatin Receptor-Mediated and Amine Transporter-Mediated Radionuclide Uptake. Am. J. Pathol. 2001;158(2):745–755.
6. Shen Y, Goerner FL, Snyder C, et al. T1 Relaxivities of Gadolinium-Based Magnetic Resonance. Invest. Radiol. 2015;50(5):330–338.
7. Ahmed Z, Levesque IR. An extended reference region model for DCE-MRI that accounts for plasma volume. NMR Biomed. 2018;31(7):1–13.
8. Berks M, Parker G, Little R, et al. Madym: A C++ toolkit for quantitative DCE-MRI analysis. J. Open Source Softw. 2021;6(66):3523.
Figures
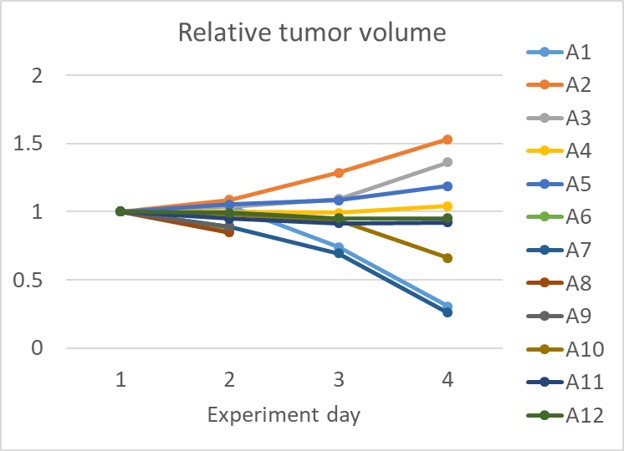
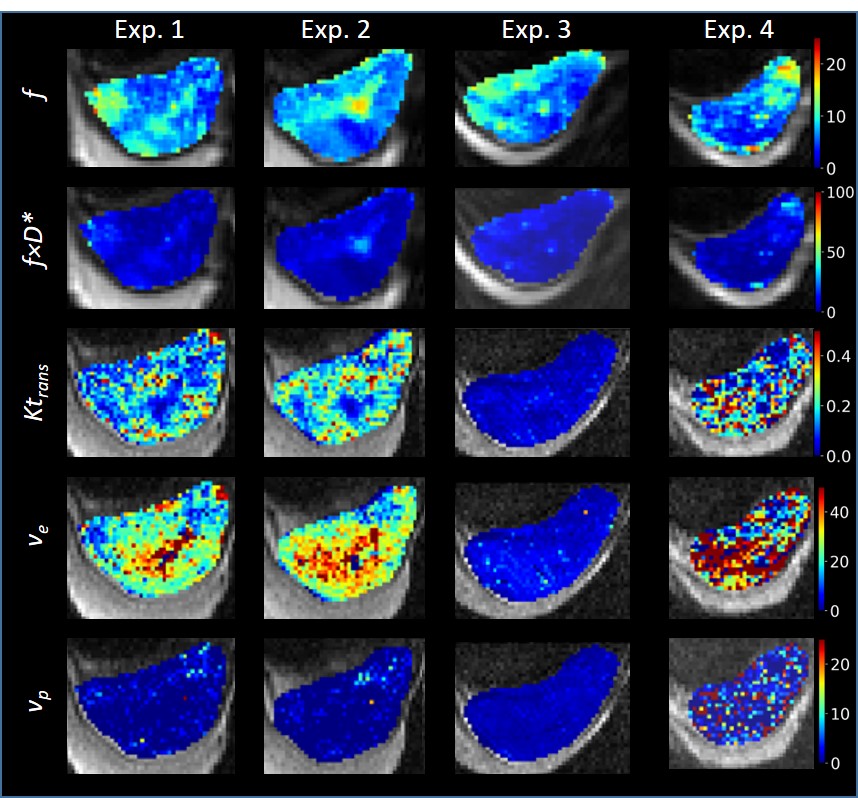
Figure 2. Visualization of parameters over time (Exp.1-Exp.4) in a tumor responding well to therapy (A7, Fig 1). Shown parameters are the perfusion fraction (f [%]),the product of f and the pseudo-diffusion coefficient (fxD*[μm2/ms]), volume transfer constant (Ktrans [min-1]) and fractional volumes of extracellular extravascular and vascular spaces (ve and vp [%], respectively). The high-intensity region below the tumors is a gel used to offset tissue-air susceptibility artefacts
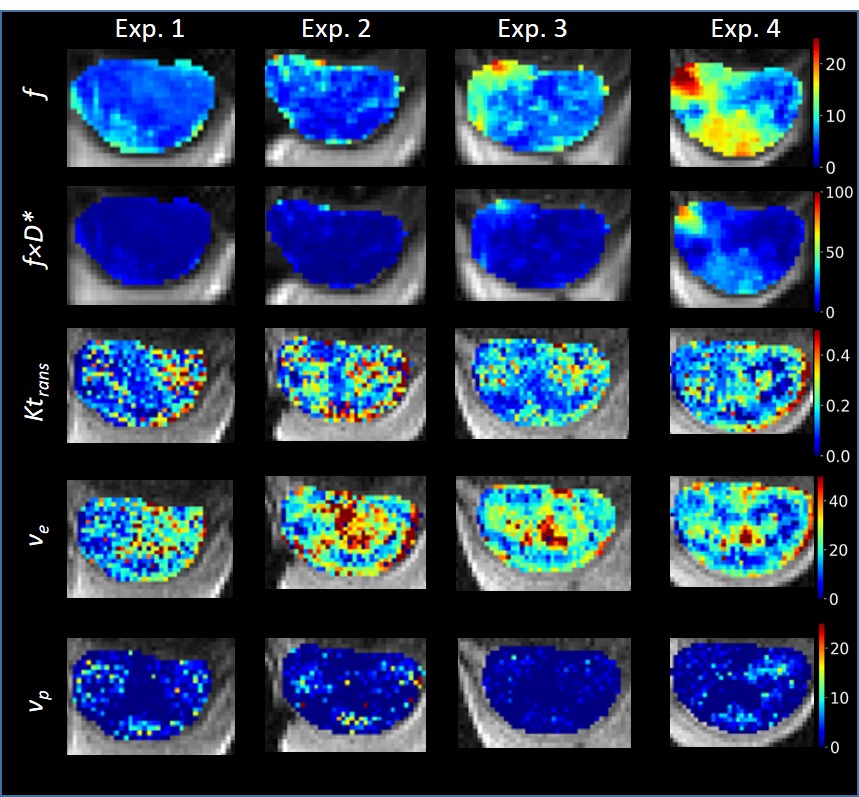
Figure 3. Visualization of parameters over time (Exp.1-Exp.4) in a tumor responding poorly to therapy (A3, Fig 1). Shown parameters are the perfusion fraction (f [%]) and the product of f and the pseudo-diffusion coefficient (fxD*[μm2/ms]), volume transfer constant (Ktrans [min-1]) and fractional volumes of extracellular extravascular and vascular spaces (ve and vp [%], respectively). The high-intensity region below the tumors is a gel used to offset tissue-air susceptibility artefacts
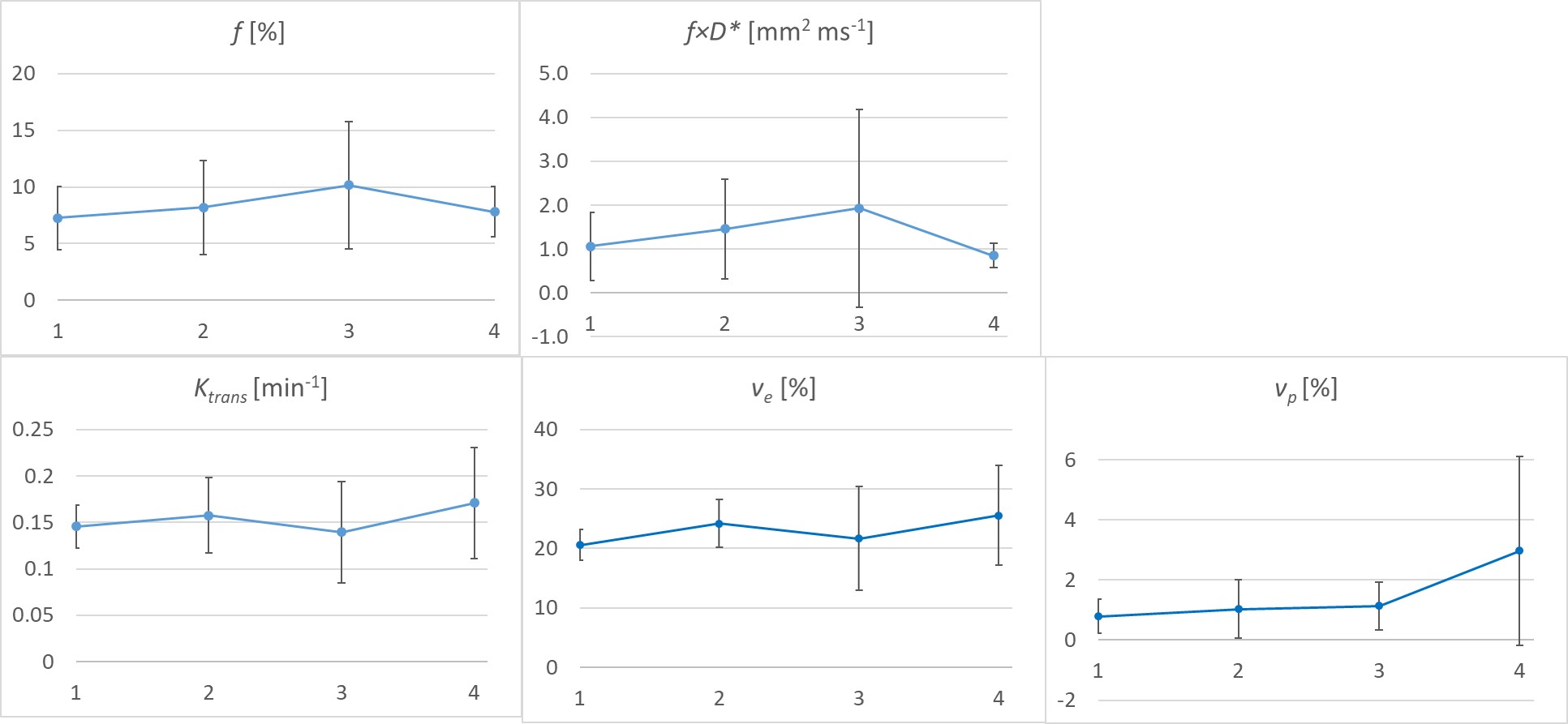
Figure 4. Mean (+/- sd) parameter values of all included tumors over time (Exp.1-Exp.4). Shown parameters are the IVIM-related perfusion fraction (f), product of f and pseudo-diffusion coefficient (fxD*) and the DCE-MRI derived Ktrans and fractional volumes of the extracellular extravascular and vascular spaces ve and vp, respectively