3958
Helix Angle structure appears preserved after myocardial infarction: a preclinical and ex vivo Diffusion Tensor CMR study1Imperial College London, London, United Kingdom, 2Royal Brompton Hospital, London, United Kingdom, 3National Institutes of Health, Bethesda, MD, United States
Synopsis
Keywords: Biology, Models, Methods, Diffusion Tensor Imaging, Cardiovascular
Motivation: Changes in myocardial microstructure that underlie post-myocardial infarction (MI) left ventricular (LV) remodelling may contribute to progressive deterioration in cardiac function and increased risk of adverse clinical events.
Goal(s): To assess post-MI temporal alterations of myocardial microstructure.
Approach: A longitudinal Diffusion Tensor CMR (DT-CMR) pre-clinical study was performed, including healthy, 3 days and 4 months post-MI timepoints, followed by ex-vivo imaging at low and high spatial resolution.
Results: High-resolution ex-vivo DT-CMR suggests preserved helical structure within the infarct core in this swine MI model, with endocardial layers appearing more compressed than mid and epicardial layers.
Impact: Improved understanding of temporal alteration of myocardial microstructure and its dynamics post-MI as seen by in-vivo DT-CMR may facilitate diagnosis and prognostication after MI.
Introduction
Changes in myocardial microstructure that underlie post-myocardial infarction (MI) left ventricular (LV) remodelling may contribute to progressive deterioration in cardiac function and increased risk of adverse clinical events. An apparent decrease in right-handed helices has been observed in Diffusion Tensor CMR (DT-CMR)1,2 derived helix angle (HA) maps in clinical studies3. We performed a longitudinal DT-CMR pre-clinical study, including healthy, 3 days and 4 months post-MI timepoints, followed by ex-vivo imaging at low and high spatial resolution, to assess post-MI temporal alterations of myocardial microstructure.Methods
Animal procedures were approved by the National Heart, Lung, and Blood Institute Animal Care and Use Committee. Yucatan minipigs (N=8, ~40kg) underwent 90-minute percutaneous balloon occlusion of the left anterior descending (LAD, N=4) or left circumflex (LCx, N=4) coronary artery just after the first diagonal/obtuse marginal branch, followed by reperfusion as described previously4. N=1 animals died before completion of the imaging protocol. In vivo CMR was performed in a 3T clinical scanner (Magnetom Skyra, Siemens Healthcare, Erlangen, Germany) before (healthy baseline), at 3 days (acute), and 4 months (chronic) after the reperfused MI procedure. In vivo STEAM EPI DT-CMR was acquired at three mid-ventricular short axis slices at peak systole and end diastole (6 diffusion directions, b-value=500s/mm2, bref=50s/mm2, resolution 2x2x8mm3) as part of a larger protocol that also included late gadolinium enhancement imaging and whole heart coverage cines2. After completion of imaging, animals were euthanised and hearts were prepared for ex vivo imaging, after formalin fixation. Ex vivo DT-CMR was performed in whole hearts in the 3T clinical scanner described above, with low spatial and angular resolution similar to the in vivo DT-CMR data described above (6 diffusion directions, b-value=500s/mm2, bref=50s/mm2, 2x2x2mm3). Subsequently, high spatial and angular resolution ex vivo spin-echo (SE) DT-CMR of transmural blocks of tissue (infarct, adjacent and remote blocks, block size ~1x1x1cm3, b-value=1000s/mm2, 120 diffusion directions, spatial resolution 150x150x150μm3) was performed in a preclinical 9.4T/20cm bore scanner (BioSpec 9.4T, Bruker, Ettlingen, Germany). DT-CMR HA maps and histograms of the distribution of HA were analysed2.Results
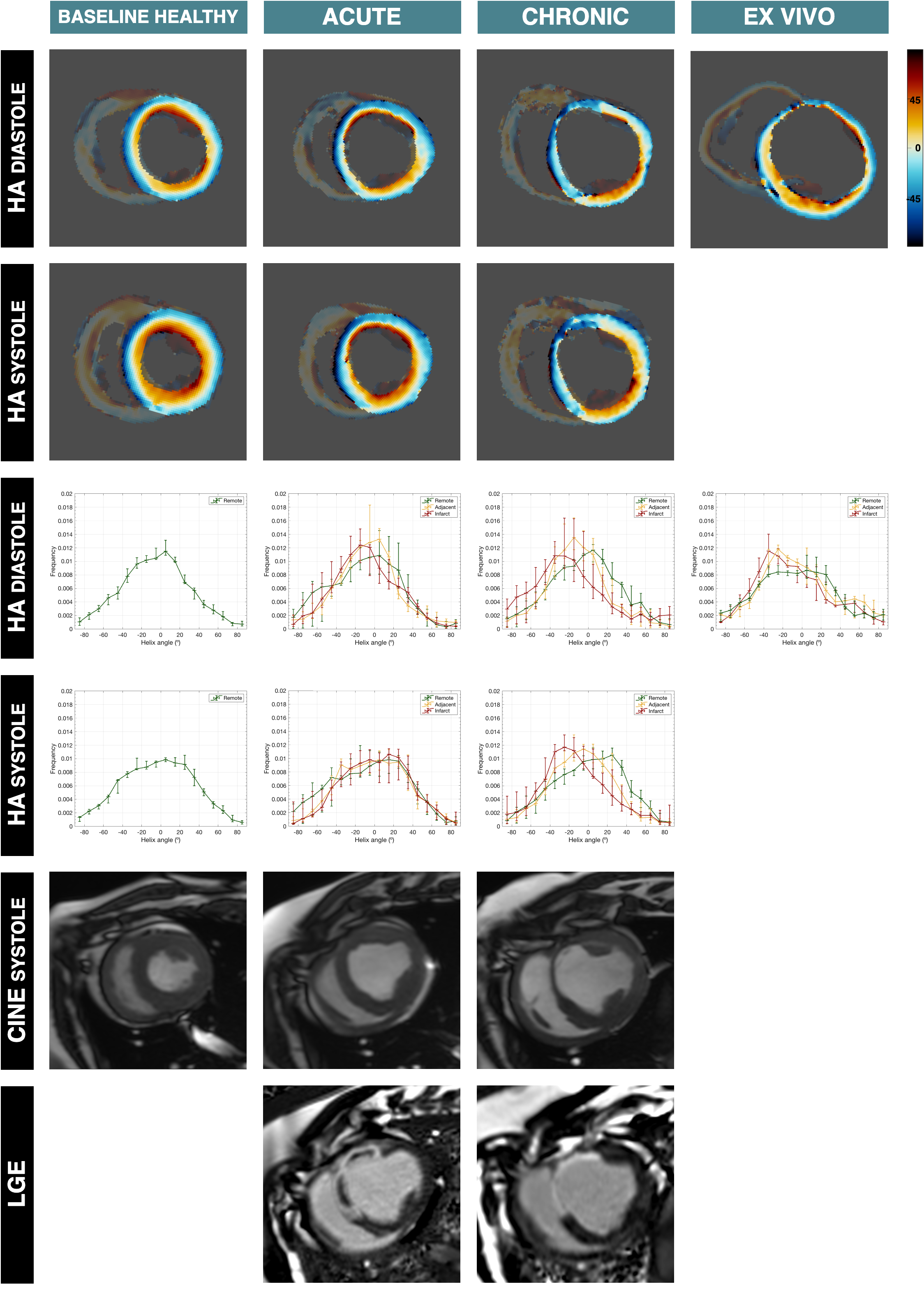
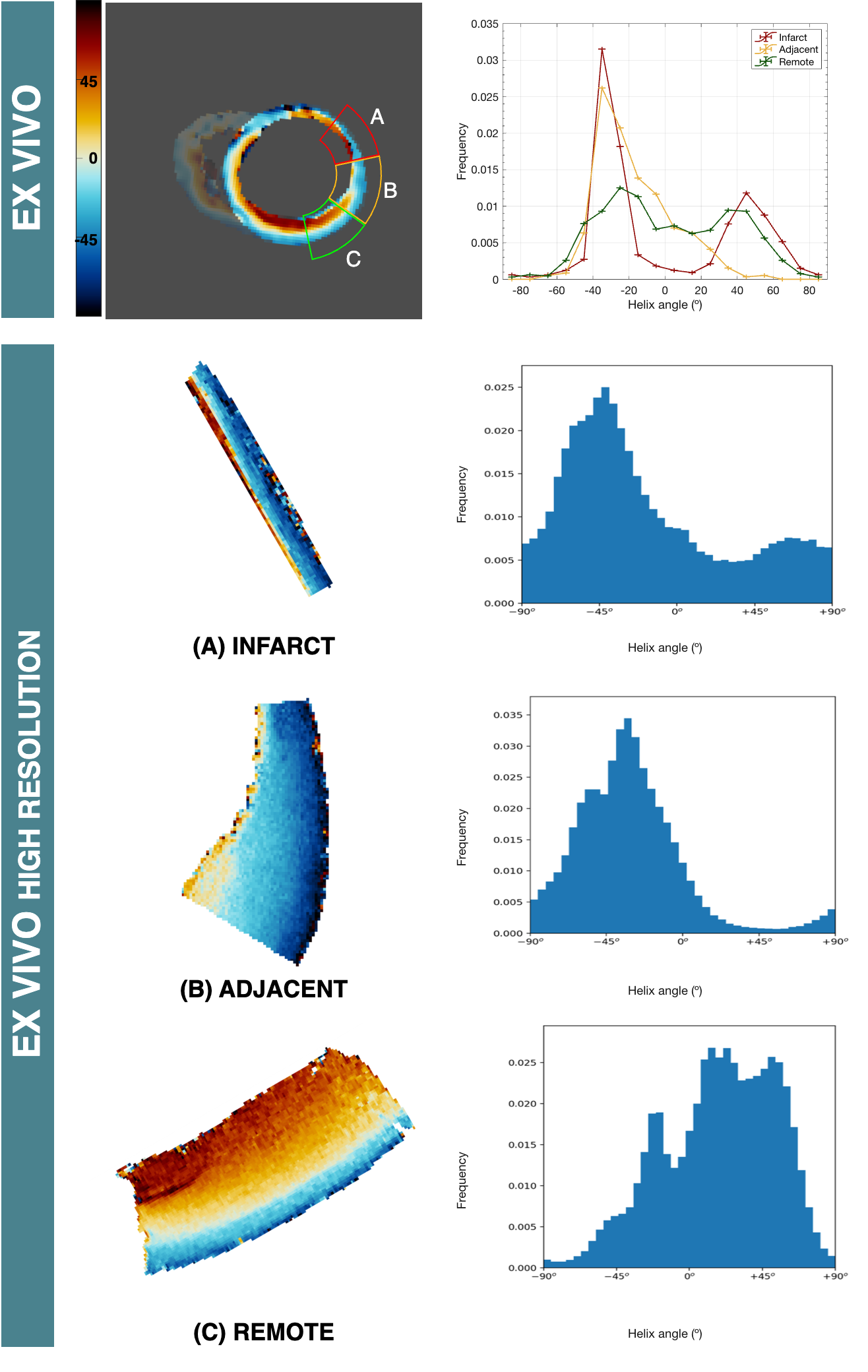
The in vivo chronic HA maps in remodeled hearts depicted reduced right-handed helix angles in the endocardium of the infarct region, also visualized in the histograms, which are shifted towards negative HA values, with associated thinning of the myocardium, consistent with ex vivo low-resolution HA data (Figure 1). However, high resolution imaging (150x150x150μm3) in a block of infarcted myocardium demonstrates preservation of the helical structure range, although compressed in the sub-endocardium (Figure 2). This can also be visualized in the corresponding histograms, which are shifted towards negative HA values in the infarct and adjacent blocks.Conclusions
High-resolution ex vivo SE DT-CMR suggests preserved helical structure range within the infarct core in this swine MI mode, however its distribution becomes skewed with endocardial layers appearing more compressed than the mid and epicardial layers. This is consistent with the known wavefront of necrosis progressing from the sub-endocardium after MI and the fact that collagen fibres, which may be barriers to water diffusion, are laid down in the same orientation as the cardiomyocyte network due to post-MI replacement fibrosis5,6,7. The apparent loss of endocardial right-handed helices in vivo is likely the consequence of partial volume effects due to the larger imaging voxel size (2x2x8mm3) in vivo.Acknowledgements
This work was supported by BHF project grant PG/14/68/30798 and BHF programme grant RG/19/1/34160.References
1. Reese TG, Weisskoff RM, Smith RN, Rosen BR, Dinsmore RE, Wedeen VJ. Imaging myocardial fiber architecture in vivo with magnetic resonance. Magn Reson Med. 1995;34:786–791.
2. Nielles-Vallespin S, Khalique Z, Ferreira PF, de Silva R, Scott AD, Kilner P, McGill LA, Giannakidis A, Gatehouse PD, Ennis D, Aliotta E, Al-Khalil M, Kellman P, Mazilu D, Balaban RS, Firmin DN, Arai AE, Pennell DJ. Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance. J Am Coll Cardiol. 2017 Feb 14;69(6):661-676.
3. Das A, Kelly C, Teh I, et al. Pathophysiology of LV Remodeling Following STEMI. J Am Coll Cardiol Img. 2023 Feb, 16 (2) 159–171.
4. de Silva R, Raval AN, Hadi M, Gildea KM, Bonifacino AC, Yu ZX, Yau YY, Leitman SF, Bacharach SL, Donahue RE, Read EJ, Lederman RJ. Intracoronary infusion of autologous mononuclear cells from bone marrow or granulocyte colony-stimulating factor-mobilized apheresis product may not improve remodelling, contractile function, perfusion, or infarct size in a swine model of large myocardial infarction. Eur Heart J. 2008 Jul;29(14):1772-82.
5. Venugopal H, Hanna A, Humeres C, Frangogiannis NG. Properties and Functions of Fibroblasts and Myofibroblasts in Myocardial Infarction. Cells. 2022 Apr 20;11(9):1386.
6. Frangogiannis NG. Cardiac fibrosis. Cardiovasc Res. 2021 May 25;117(6):1450-1488.
7. Frangogiannis NG. The extracellular matrix in myocardial injury, repair, and remodeling. J Clin Invest. 2017 May 1;127(5):1600-1612.
Figures