3949
Real time monitoring of Ca2+ homeostasis by manganese enhanced cMRI in a remotely induced myocardial ischemia reperfusion injury mouse model1Biomedical MRI, Department of Imaging and Pathology, KU Leuven, Leuven, Belgium, 2Department of Cardiovascular Sciences, KU Leuven, Leuven, Belgium
Synopsis
Keywords: Biology, Models, Methods, Ischemia, Contrast Mechanisms, Molecular Imaging
Motivation: Studies on cardiac ischemia reperfusion injury mainly focus on events following an ischemic event. Our focus were the initial moments during occlusion and reperfusion in a novel murine model.
Goal(s): Our goal was to characterize the dynamic processes occurring during and immediately after ischemia.
Approach: Manganese is a calcium analogue and potent T1-contrast agent for MRI that enters cardiomyocytes through active calcium channels. By exploiting this mechanism, the disruption of calcium homeostasis was monitored during and after ischemia.
Results: Studying the early phase of ischemia is feasible and data suggest a link between the final scar extent and severity of Ca2+ homeostasis disruption.
Impact: Preclinical ischemia-reperfusion injury studies can now be complemented with an early marker for subsequent injury. Revealing the dynamic processes occurring during and immediately after an ischemic event might help to assess the effects of applied therapeutics at an earlier stage.
Introduction
Myocardial ischemia-reperfusion injury (IRI) has long been a subject of scientific investigation, with most research focusing on events that transpire days after the ischemic episode1. Early determination of tissue viability following an infarction is crucial for precise diagnosis and treatment planning. Still, the determination process remains challenging. Previously, it was demonstrated that manganese, a calcium analogue, can measure the alterations in calcium homeostasis which can be used to reveal salvageable tissue. However, in those studies, myocardial viability was not investigated sooner than 1 hour following the start of ischemia in a clinically less relevant model of permanent occlusion2-4. In contrast, we present a unique perspective on this critical period focusing on the ischemic event itself. Employing a novel murine model in which ischemia is initiated during the imaging session, we provide insights into myocardial viability during these overlooked early moments of occlusion and reperfusion by probing calcium homeostasis with manganese.Methods
Animal Model: Mice (C57BL/6, male, 10-12 weeks old, n = 13) underwent microsurgery to place a stitch around the left anterior descending artery (LAD) for possible occlusion. Ischemia was triggered remotely in the IRI group for 30 min (n=8) using a novel setup while sham-operated (determined randomly) received the same surgery without LAD occlusion.MR Imaging: All mice underwent MRI on a 7T Biospec MR scanner (Bruker PCI, Ettlingen, Germany) at four time points (Fig. 1). An 86 mm quadrature transmit coil combined with a surface receive-only coil (T20010V3, Bruker) placed over the chest of the animal was used. Inhalation anesthesia was maintained at 1.5% isoflurane and 1.5 L/ min O2 throughout all experiments. Temperature-respiratory-cardio monitoring was performed using an MR-compatible system (SA Instruments, NY, USA) to maintain the physiological state at 36.5 °C, 70-100 min-1, and 450-600 min-1, respectively. Mice were positioned supine in a purpose-built cradle on day 0 to perform the remote occlusion5. Jointly, manganese chloride (MnCl) (Sigma Aldrich, Saint Louis, USA) was used as a probe (0.1 mmol/kg, i.p. catheter) to monitor the dynamic alterations in calcium homeostasis after the ischemia onset. Dosing was based on a similar study thoroughly reporting events following MnCl administration4. The infarct size was measured 24 hours after surgery via late gadolinium enhancement (LGE). Briefly, gadolinium (Gd-DOTA) (Dotarem, Guerbet, France) was injected (0.5 mmol/kg, i.p.) 20 min prior to scanning. T1 mapping was performed on baseline, day 0, and day 28 with a 3D retrospectively gated T1-weighted FLASH (Intragate, Bruker) and variable flip angle (2/5/8/11/14°) with TE/TR = 2.3/ 11.1 ms. Image matrix 120 x 110 with a FOV of 28 x 25 mm2 was used. Functional analysis was performed at baseline and 28 days post-surgery using an oversampling of 200 at FA 14° reconstructed into 20 cardiac frames. T1 maps were constructed using an oversampling of 25 at FA 2/5/8/11/14° reconstructed into 4 cardiac frames. Postcontrast T1 maps on day 0 were acquired by repeating the 14° FA and extracting the T1 values through pixel-wise signal relation before contrast. LGE-MRI was performed with a multi-slice 2D retrospectively gated T1-weighted FLASH with the same parameters as baseline but with FA = 45°.
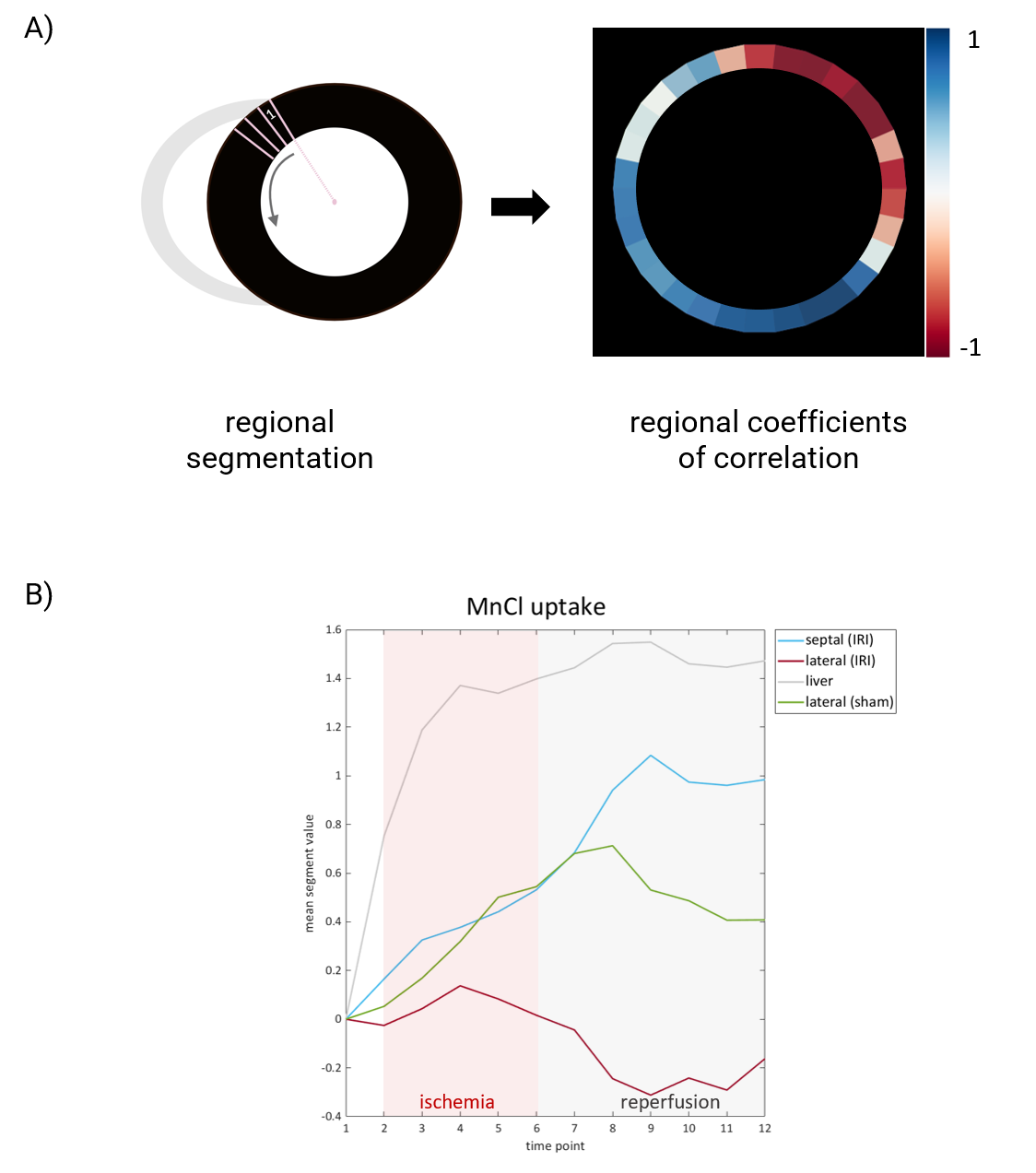
Image Analysis: Analysis was done by a single investigator in random order with custom-written scripts in MATLAB (MathWorks, Natick, USA). T1 mapping and bias field correction available code was employed6,7. For regional analysis, the myocardium was segmented into 30 regions based on the polar angle around the center of the left ventricle oriented counterclockwise (Fig. 3A). Regional alterations in MnCl uptake were characterized as Kendall’s correlation coefficient compared to the liver uptake.
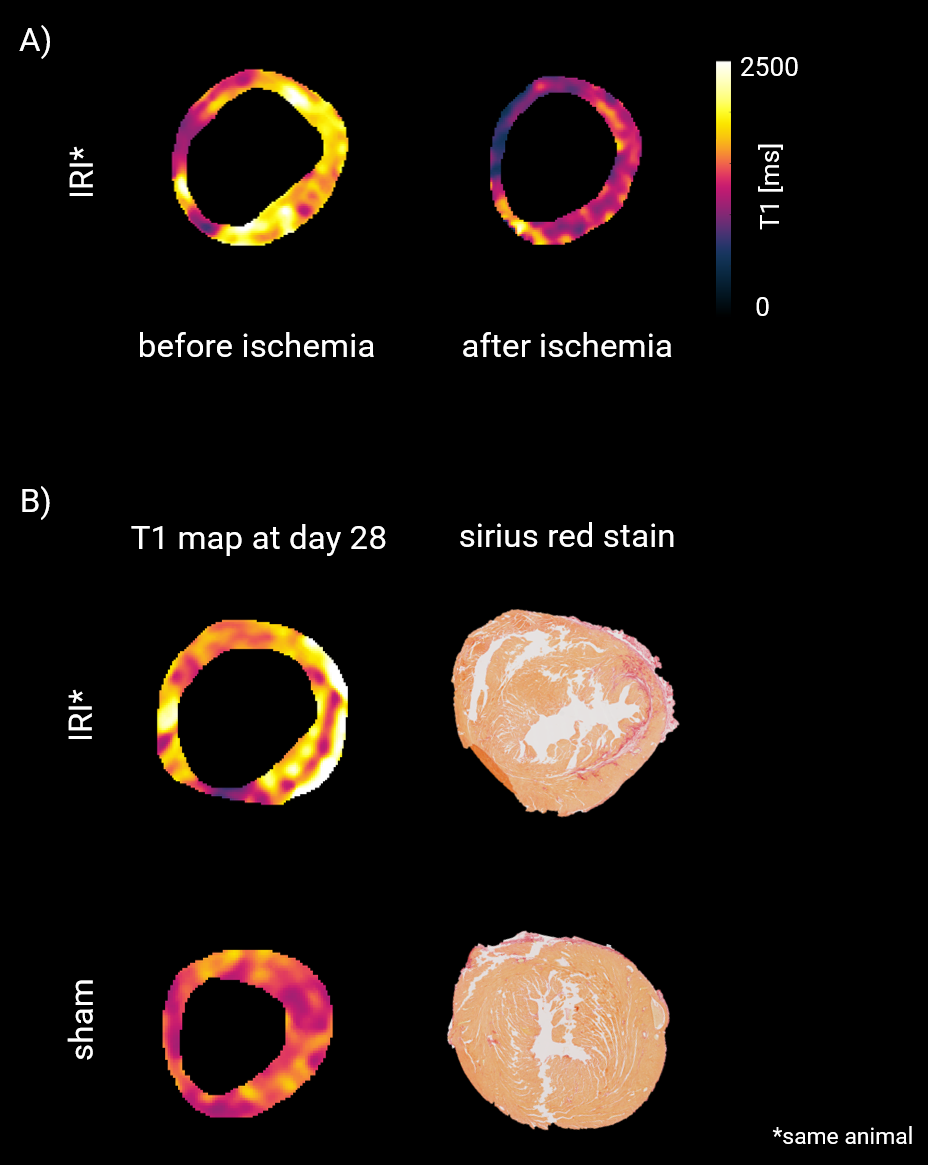
Histology: Sirius red staining was performed 28 days after surgery to depict the extent of scar tissue. The whole heart was longitudinally divided into four sections and cut perpendicularly in short-axis orientation.
Results
An example dataset (Fig. 2) demonstrates the feasibility of monitoring calcium homeostasis during and immediately after an ischemic event. Sections characterized by low correlation to normal liver uptake during ischemia might already characterize unrecoverable regions as the rate of Mn uptake is proportional to tissue viability3 (Fig. 3). This pattern is confirmed by final scar formation corresponding to a region with low Mn uptake quantified by T1 value at the onset of ischemia (Fig. 4).Discussion and Conclusions
We demonstrate the feasibility of investigating myocardial ischemia at the moment of its origin, gathering insights into cellular changes, and the potential for identifying salvageable tissue immediately following myocardial infarction. With an understanding of the relationship to the scar tissue formed, an early insight into the efficacy of the applied treatment can be provided.Acknowledgements
The experiments were performed at the KU Leuven core facility Molecular Small Animal Imaging Center (MoSAIC). The research was supported by research grants from KU Leuven (C14/20/095) and the Research Foundation-Flanders (FWO G0A7722N). M. Algoet was supported by the Research Foundation Flanders Fellowship Grant (11A2423N).References
(1) De Villiers, C. & Riley, P. R. Mouse models of myocardial infarction: comparing permanent ligation and ischaemia-reperfusion. Dis Model Mech 13, (2020). (2) Waghorn, B. et al. Monitoring dynamic alterations in calcium homeostasis by T 1-weighted and T 1-mapping cardiac manganese-enhanced MRI in a murine myocardial infarction model. NMR in Biomedicine 21, 1102–1111 (2008). (3) Waghorn, B. et al. Indirectly probing Ca2+ handling alterations following myocardial infarction in a murine model using T1-mapping manganese-enhanced magnetic resonance imaging. Magnetic Resonance in Medicine 65, 239–249 (2011). (4) Jasmin, N. H. et al. Myocardial Viability Imaging using Manganese-Enhanced MRI in the First Hours after Myocardial Infarction. Advanced Science 8, 2003987 (2021). (5) M. Algoet*, M. Pusovnik* et al., Remote LAD Occlusion in Spontaneously Breathing Mice: A Novel Approach for Studying Myocardial Ischemia-Reperfusion Injury (under review in Journal of Visual Experiments, Oct 2023). (6) Ramos-Llorden G, Vegas-Sanchez-Ferrero G, Bjork M, Vanhevel F, Parizel PM, San Jose Estepar R, den Dekker AJ, Sijbers J. NOVIFAST: A Fast Algorithm for Accurate and Precise VFA MRI Mapping. IEEE Trans Med Imaging.,37(11):2414-2427 (2018). (7) Chunming Li (2023). MRI segmentation and bias field correction (https://www.mathworks.com/matlabcentral/fileexchange/59752-mri-segmentation-and-bias-field-correction), MATLAB Central File Exchange. Retrieved August 24, 2023.Figures
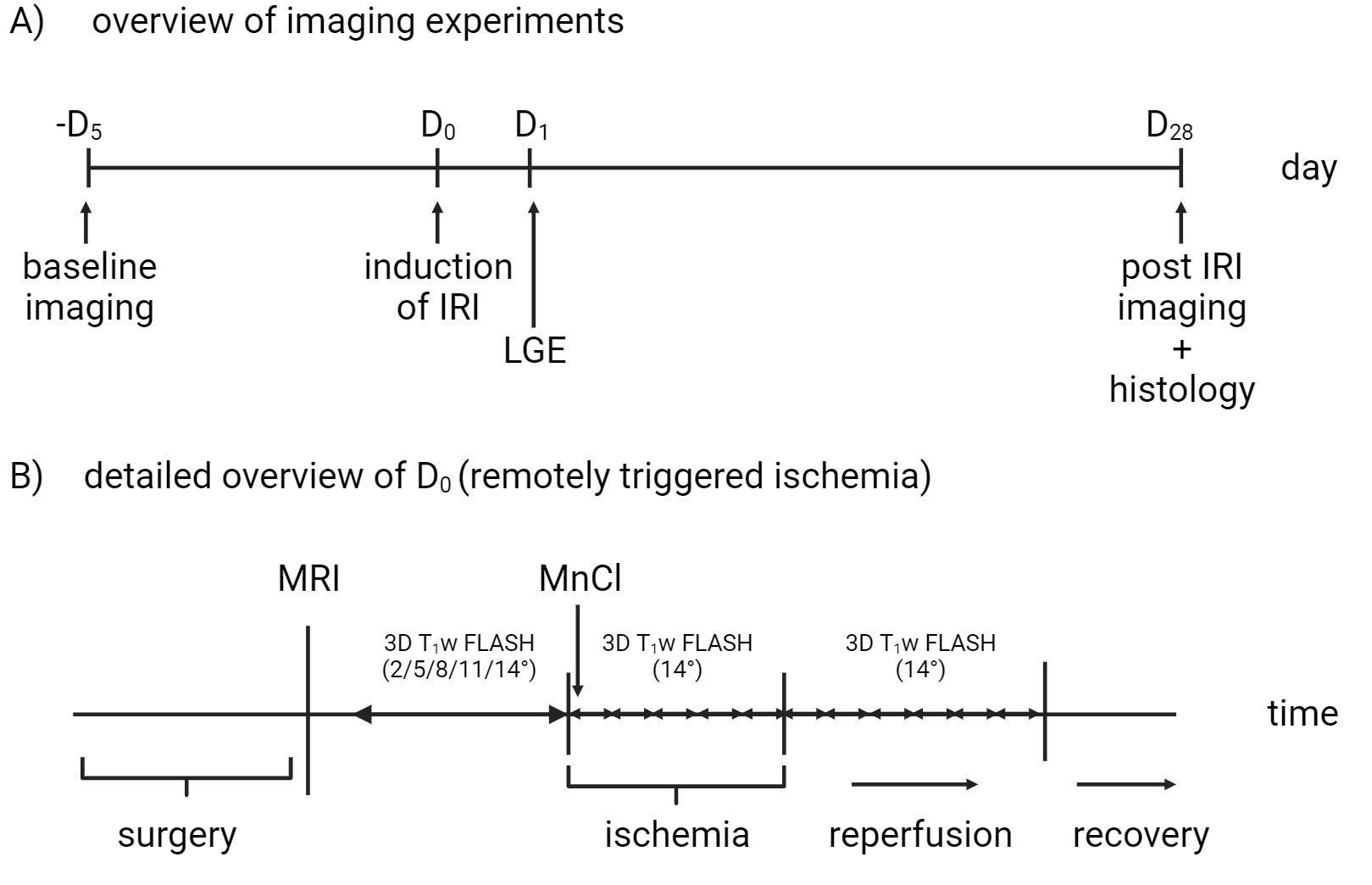
Figure 1: Overview of MRI experiments performed. A) General timeline of imaging experiments. B) Detailed overview of the experimental protocol during remotely triggered ischemia-reperfusion injury
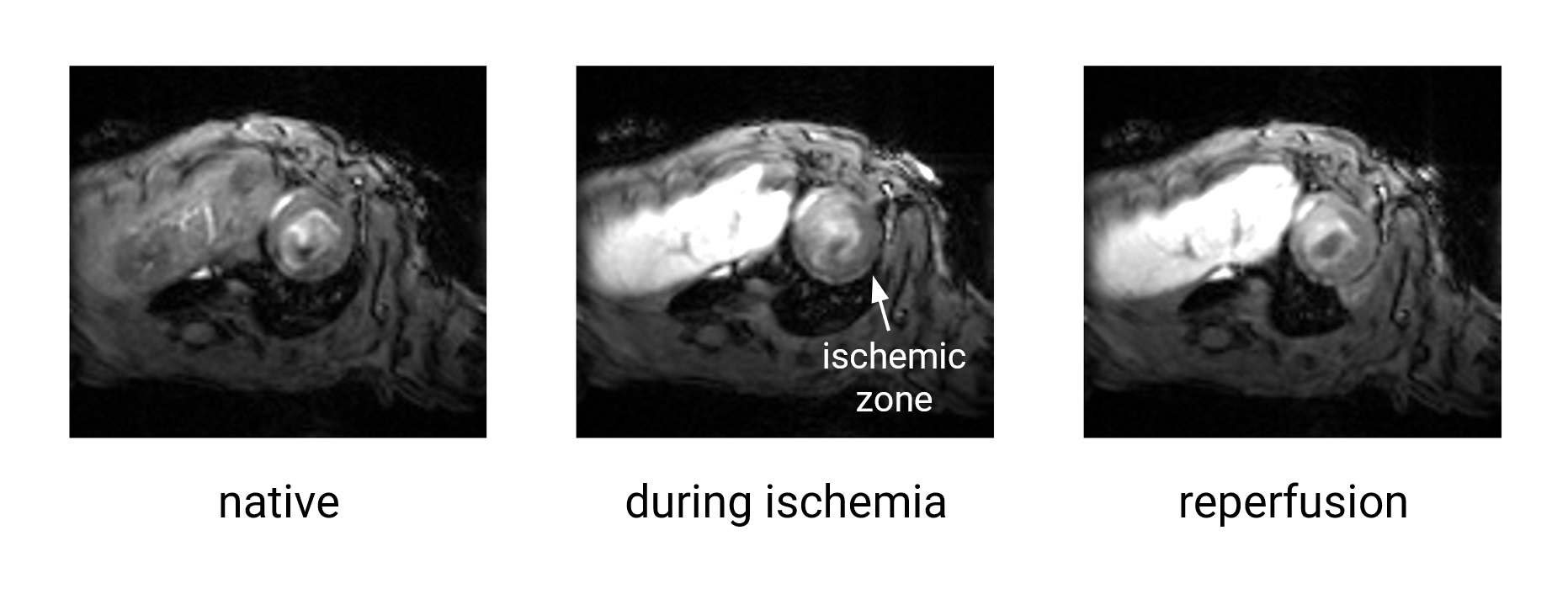
Figure 2: Probing calcium homeostasis during and immediately after ischemia with manganese-enhanced MRI is feasible. Mid-ventricular slice shows the tissue region with low manganese uptake during ischemia (white arrow). Images are shown in raw signal intensities with a common intensity scale.