3919
Motion compensated SE diffusion tensor cardiovascular magnetic resonance at ultra-high gradient strength at Connectom scanner1National Heart and Lung Institute, Imperial College London, London, United Kingdom, 2Cardiovascular Magnetic Resonance Unit, The Royal Brompton Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3Cardiff University Brain Research Imaging Centre (CUBRIC), Cardiff University, Cardiff, United Kingdom, 4Siemens Healthcare Ltd, Camberly, United Kingdom
Synopsis
Keywords: Gradients, Diffusion/other diffusion imaging techniques
Motivation: Second-order motion-compensated spin-echo (MCSE) DT-CMR is limited by long echo-times (TE), resulting in T2-related signal-loss.
Goal(s): Use the ultrahigh gradient-strength of the Connectom scanner to reduce TE of second-order MCSE DT-CMR.
Approach: A second-order MCSE DT-CMR pulse-sequence was developed. Ultra-high (180mT/m) and a high gradient-strength (80mT/m) were compared in acquiring in-vivo DT-CMR data at two cardiac phases.
Results: The substantial reduction in TE enabled by ultra-high gradient-strength resulted in improvements in signal-to-noise ratio (SNR) in both cardiac phases. To our knowledge this is the first report comparing the performance of second-order MCSE DT-CMR at ultra-high gradient-strength (Connectom) to widely available high gradient-strengths.
Impact: Second-order MCSE DT-CMR acquired using ultra-high diffusion gradient strengths increases SNR in both cardiac phases, paving the way for future clinical translation of efficient multiphase DT-CMR.
Introduction
DT-CMR uniquely provides quantitative characterisation of the myocardial microstructure1. Second-order motion compensated spin echo (MCSE) methods were shown to efficiently minimise the sensitivity of DT-CMR to bulk cardiac motion in systole2. However, the TEs are typically long, resulting in T2-related signal-loss, and acquisitions frequently fail in diastolic phases3-5. At ultra-high gradient strengths, a substantial reduction in TE is possible, with potential increases in SNR and improvements in robustness of diastolic imaging.We compare second-order MCSE DT-CMR acquired with the ultra-high gradient strength at Siemens 3T Connectom (300mT/m) to a currently clinically available high gradient strength of 80 mT/m at both peak systolic and diastolic cardiac phases.
Methods
A second order MCSE EPI DT-CMR sequence2,6 (Figure 1) with zonal-excitation was developed to utilize the ultrahigh gradient strength of the 3T Connectom scanner (Siemens Healthcare, Germany) accounting for patient safety (peripheral-nerve and cardiac stimulation). The maximum gradient strength was limited to 180 mT/m due to slew rate limitations, which resulted in zero flat top time in the shorter diffusion encoding gradient lobe. It was deployed with (i) the maximum gradient strength possible (180 mT/m) and (ii) a limited gradient strength (80 mT/m, replicating Siemens Prisma). For effective fat-suppression, a four-pulse binomial water excitation was used (1:3:3:1).ECG triggered short-axis DT-CMR acquisitions with six encoding directions at b = 0,150 (2 averages), 500 s/mm2 (8 averages) were acquired at 2.8×2.8×8 mm3 (1.4×1.4x8 mm3 reconstructed) for both cardiac phases (systole and diastole) with field of view 360×135 mm2, TE= 58/48 ms (for Gmax= 80/180 mT/m), repetition-time = 2RR intervals and SENSEx2.
11 healthy human subjects (5 female, 19-42 years) were recruited in accordance with ethical approval. Two subjects’ data were used in optimising protocols and two subjects’ data were discarded for scanner malfunction and excessive heart-rate variability. All DT-CMR data was processed using an in-house MATLAB (Mathworks, MA) software tool.
Results
From the 7 subjects that the protocol was successfully completed in, data was discarded from 1 subject in systole and 2 in diastole due to poor DT-CMR data quality. Example MCSE DT-CMR images at both gradient strengths are demonstrated in Figure 2. The single image SNR (repeated measurement technique) is compared between gradient strengths in Figure 3. An increase in SNR in the diffusion-weighted images for higher gradient strength of 180mT/m compared to 80 mT/m is observed and the median SNR is higher for every direction at b=500 s/mm2 and for b=0 s/mm2 in both cardiac phases.Figure 4 shows example DT-CMR parameter maps for both diffusion gradient strengths and cardiac phases. The average fractional-anisotropy (FA), mean-diffusivity (MD), helix-angle (HA) slope and second eigenvector (E2A) in the left ventricle (LV) myocardium for both cardiac phases are compared between diffusion gradient strengths in Figure 5. The observed significant difference in the standard-deviation (SD) of MD, E1, E2, E3 and HA-slope across the myocardium at diastole suggest improvement of the data quality for ultra-high gradient strength.
Discussion and Conclusion
To the best of our knowledge this is the first report comparing second-order MCSE DT-CMR at ultra-high gradient strength of 180 mT/m utilizing the Siemens Connectom to the high gradient strength available in other 3T scanners (i.e., 80 mT/m, Siemens Prisma). While others have demonstrated the use of Connectom gradients in providing high b-values and 3rd order motion-compensated DT-CMR with more complex encoding waveforms7, this report demonstrates the utility of Connectom gradients in providing multi-phase MCSE DT-CMR.The substantial reductions in TE enabled by ultra-high gradient strengths resulted in an improvement in SNR. With a larger cohort in future studies, the improved robustness of MCSE DT-CMR acquired in diastolic cardiac phases with ultra-high diffusion encoding strengths is expected to be evident, paving the way for future clinical translation of efficient multiphase DT-CMR.
Acknowledgements
This work was funded by British Heart Foundation grant RG/19/1/34160.
References
1. Nielles-Vallespin et al., Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance, JACC 2017, 69(6).
2. Stoeck et al., Second-Order Motion-Compensated Spin Echo DiffusionTensor Imaging of the Human Heart, MRM 2016, 75:1669–1676.
3. Khaliqueet al. Diffusion tensor cardiovascular magnetic resonance in hypertrophic cardiomyopathy: a comparison of motion-compensated spin echo and stimulated echo techniques. MAGMA 2020, 33(3):331-342.
4. Scott et al. An in-vivo comparison of stimulated-echo and motion compensated spin-echo sequences for 3 T diffusion tensor cardiovascular magnetic resonance at multiple cardiac phases, JCMR 2018, 20:1.
5. Moulin et al., Probing cardiomyocyte mobility with multiphase cardiac diffusion tensor MRI, PLOS ONE 2020, 15(11): e0241996.
6. Welsh et al., Higher-Order Motion-Compensation for In Vivo Cardiac Diffusion Tensor Imaging in Rats, IEEE Trans Med Imaging 2015, 34(9):1843-53.
7. Afzali et al., Cardiac diffusion MRI using Connectom scanner, Proc. Intl. Soc. Mag. Reson. Med. 2023, 31:4284.
Figures
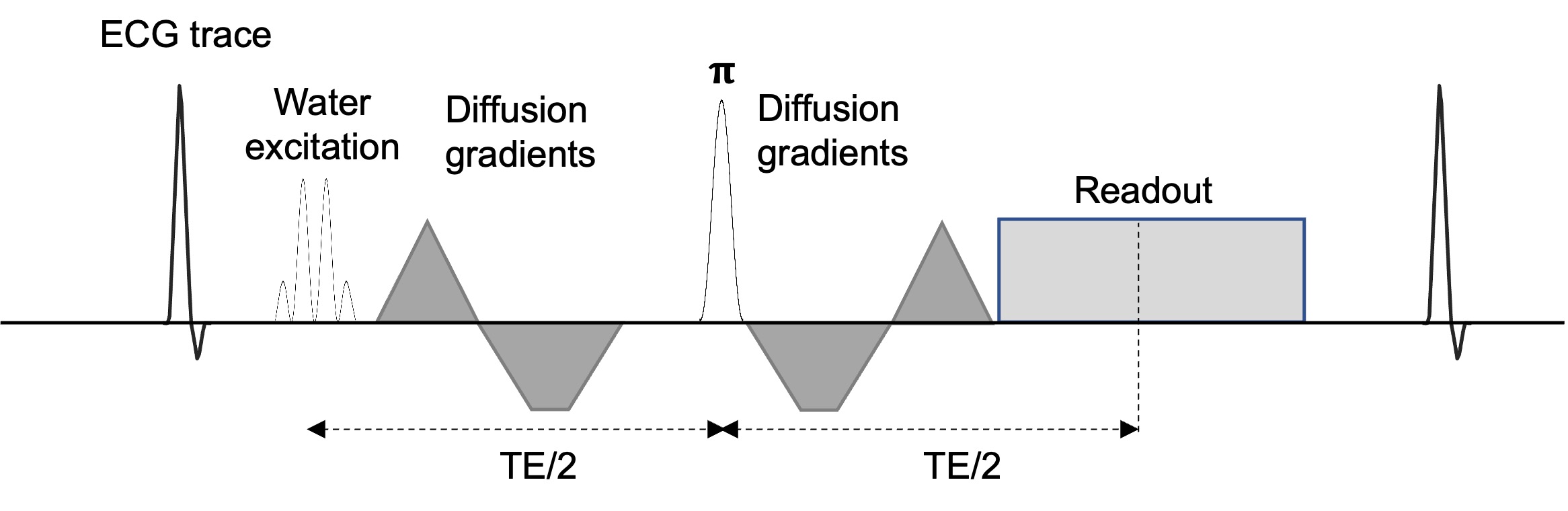
Figure1: Second order MCSE EPI DT-CMR pulse-sequence for the Connectom scanner utilizing binomial water selective (1:3:3:1). While the Connectom scanner can achieve 300mT/m, slew-rate limitations resulted in triangular gradient waveforms in the shorter diffusion encoding lobe at 180mT/m, prohibiting any further increases in gradient amplitude for this waveform design.
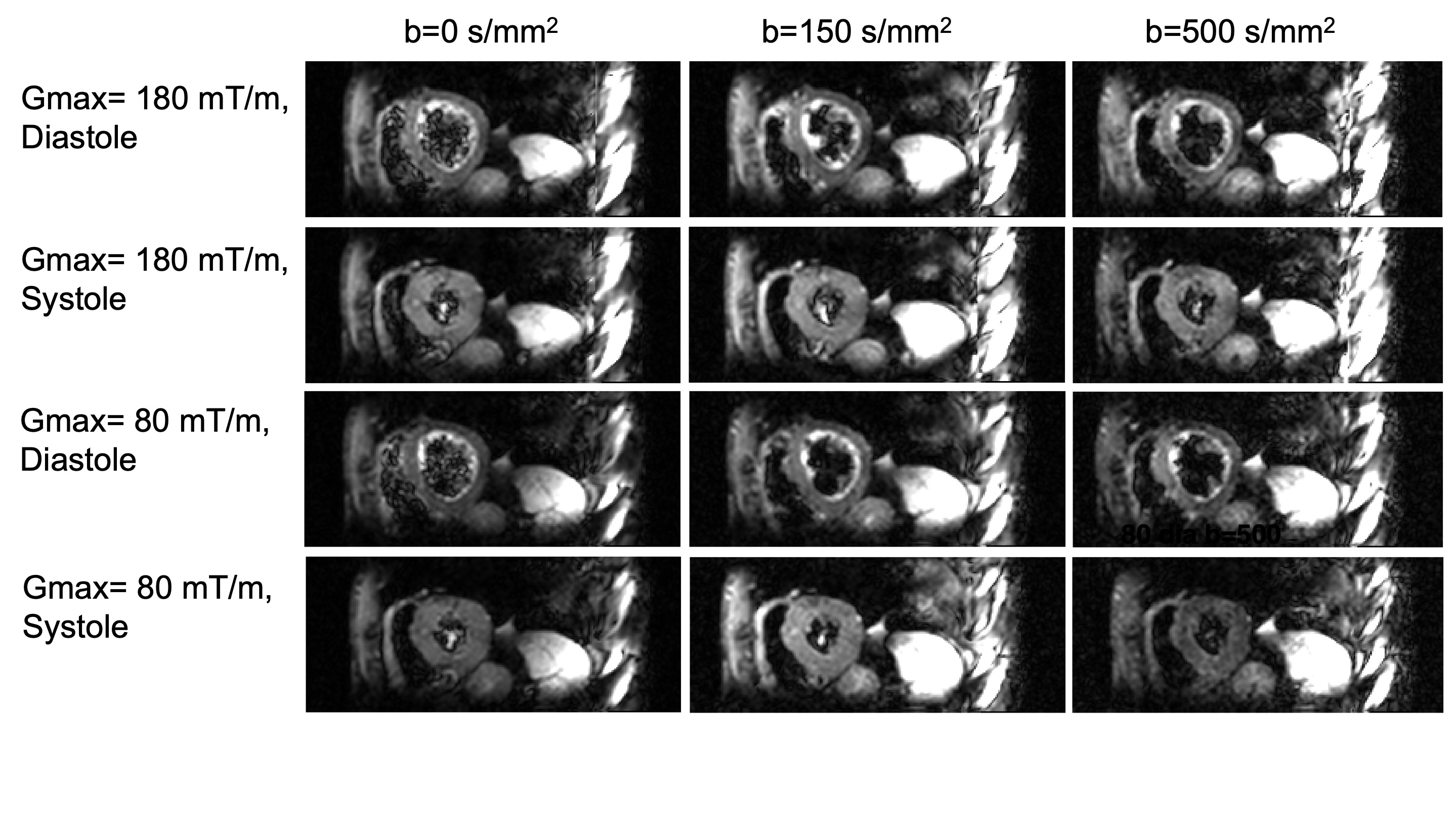
Figure 2: Second order MCSE DT-CMR images for b=0, 150 and 500 s/mm2 for two diffusion gradient strengths (80 and 180 mT/m) for a healthy subject during both cardiac phases. One encoding direction is shown for b=150 and 500 s/mm2. The images are windowed separately to highlight the image quality at all b-values. The improvement in SNR at the higher maximum gradient strength is visually apparent.
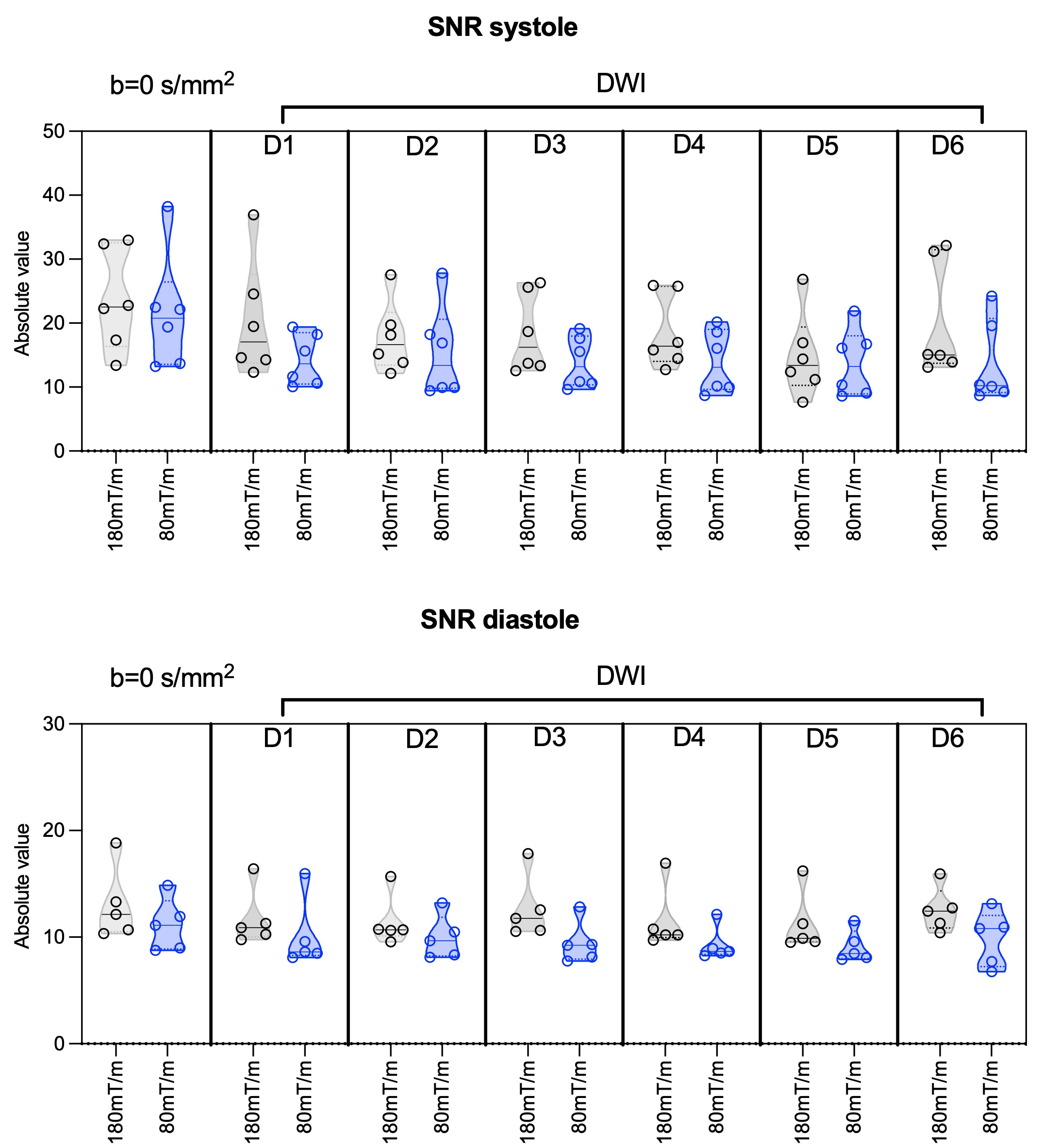
Figure 3: Mean single image SNR in the LV myocardium for each subject (individual data point), both diffusion gradient strengths and cardiac phases for b=0s/mm2 and diffusion weighted data for six diffusion directions (D1-6) with b=500s/mm2 (calculated using the multiple repetitions method). An improvement in SNR is evident for both cardiac phases. In diastole, median SNR is higher for every direction at b=500s/mm2 and for b=0s/mm2.
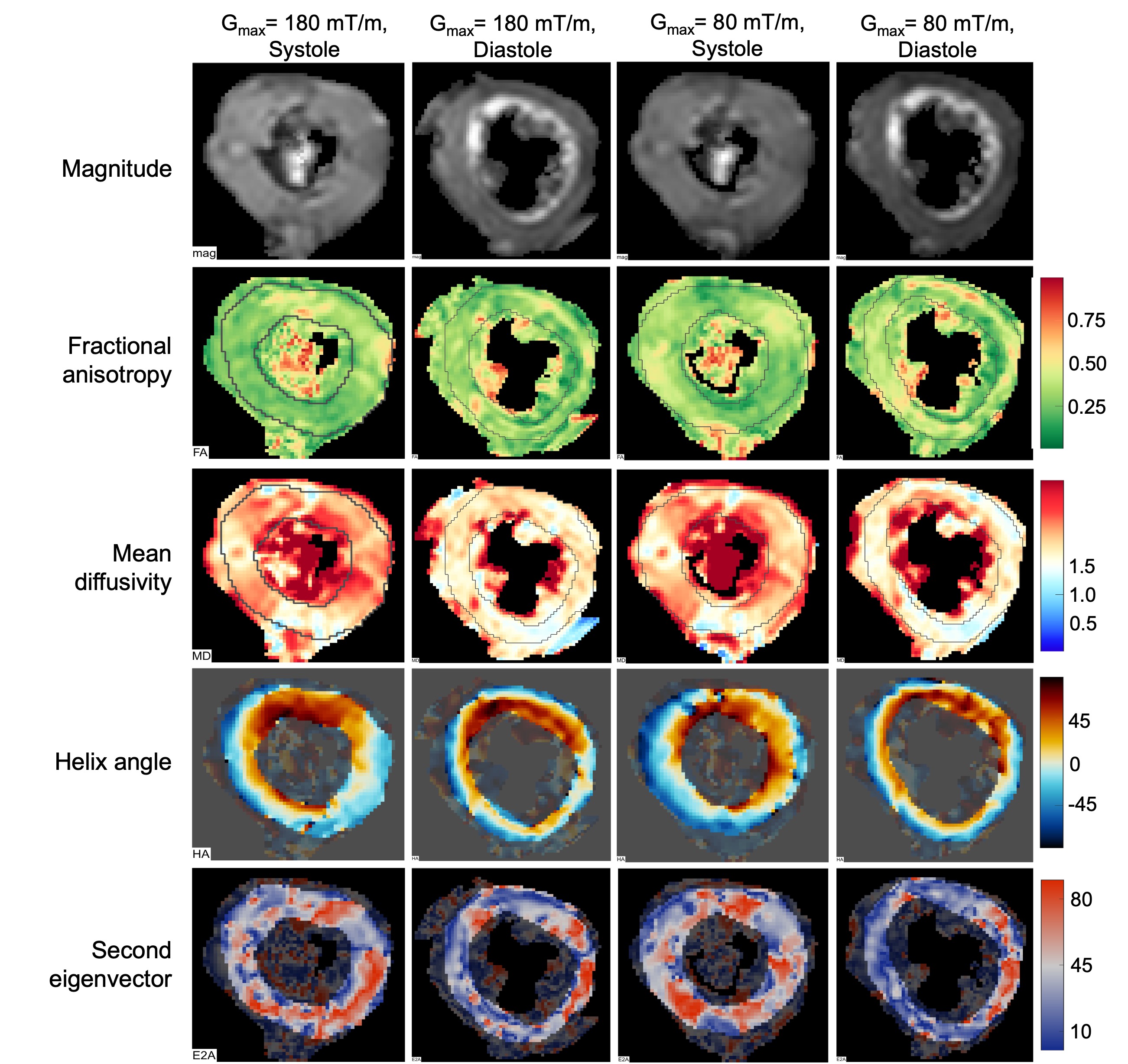
Figure 4: DT-CMR parameter maps calculated for a healthy subject data, obtained for both diffusion gradient strengths and cardiac phases.
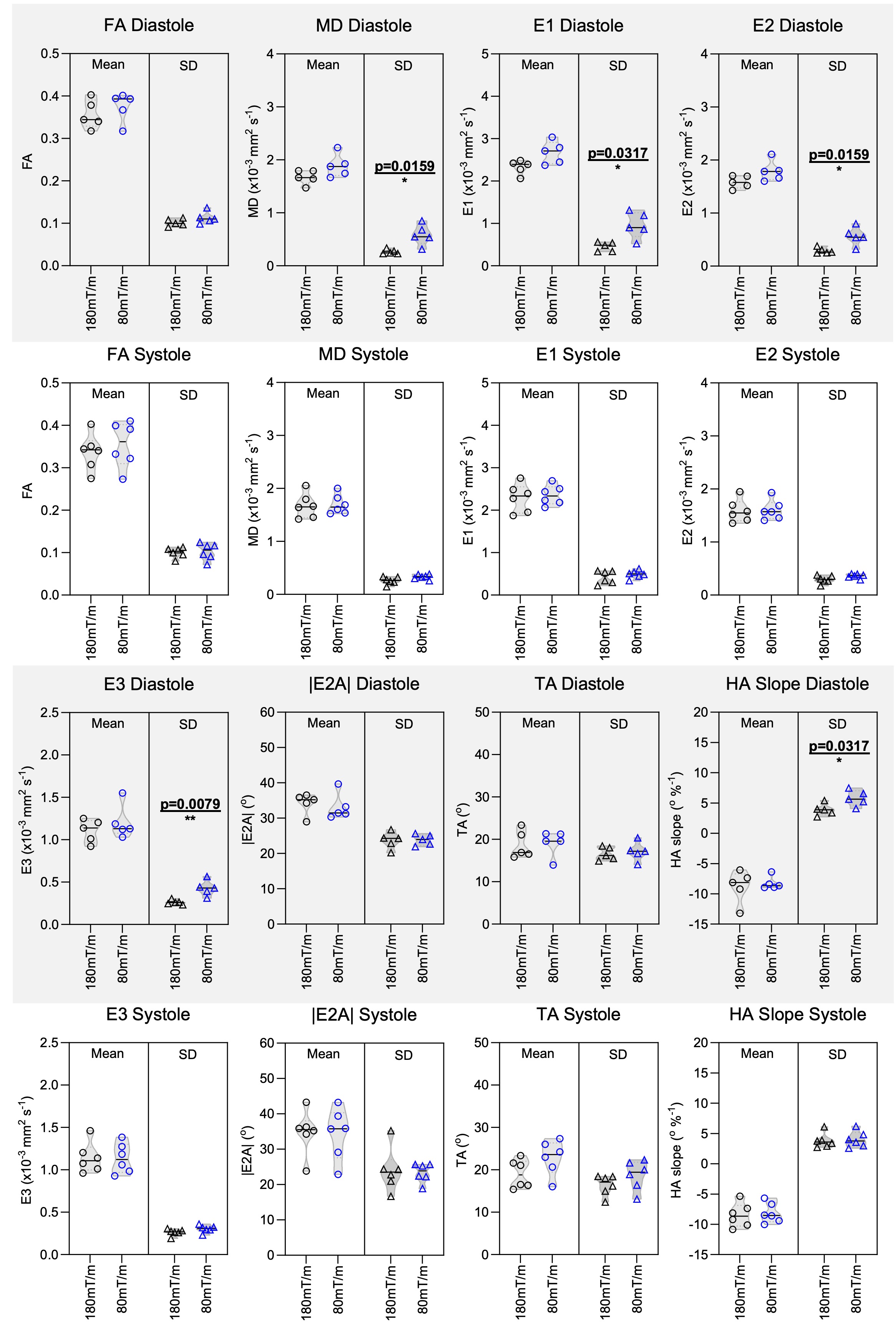
Figure 5: Mean and standard deviation (SD) of DT-CMR parameters over the LV for each subject (individual data point) are presented here for fractional anisotropy (FA), mean diffusivity (MD), helix angle (HA) slope, transverse angle (TA), second eigenvector (E2A) and eigenvalues (E1, E2, E3) for both diffusion gradient strengths and cardiac phases. For statistical analysis Mann-Whitney test was used and p<0.05 considered to be significant.