3917
Addressing Gradient Imperfection Related Bias in Stack-of-Stars MRI for Free-Breathing, Confounder-Corrected T1 Mapping1Department of Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 2Department of Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Department of Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 4GE Healthcare, Waukesha, WI, United States, 5Department of Electrical and Computer Engineering, University of Wisconsin-Madison, Madison, WI, United States, 6Department of Medicine, University of Wisconsin-Madison, Madison, WI, United States, 7Department of Emergency Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: System Imperfections, Relaxometry
Motivation: Non-Cartesian sampling strategies enable free-breathing imaging due to their robustness against motion but are susceptible to artifacts related to gradient imperfections. Such artifacts may manifest as bias or structured noise in quantitative imaging applications.
Goal(s): In this study, we explore the effects of gradient imperfections and evaluate the performance of gradient correction methods in non-Cartesian, confounder-corrected T1 mapping using both phantom and in vivo imaging experiments.
Approach: For this purpose, we compare confounder-corrected T1 maps reconstructed with data-driven and calibration-based gradient correction approaches.
Results: Our initial results indicate that gradient correction methods are essential for mitigating the bias due to gradient imperfections.
Impact: This study confirms that gradient imperfections result in bias in non-Cartesian quantitative imaging applications. Our findings indicate that T1 relaxometry is less susceptible to gradient imperfections than PDFF and R2* quantification. The application of gradient correction methods mitigates this bias.
Introduction
Conventional T1 mapping typically relies on Cartesian sampling, favored for its robustness to gradient imperfections and straightforward image reconstruction1-3. However, Cartesian sampling is prone to motion artifacts, which are addressed through respiratory-triggered and breath-hold imaging. These methods reduce imaging efficiency and put constraints on imaging times.Non-Cartesian methods such as stack-of-stars (SoS) are well-suited for free-breathing imaging due to their motion insensitivity4. However, non-Cartesian techniques are affected by gradient imperfections, such as gradient delays and eddy currents5-7. These imperfections cause differences between the intended and actual k-space trajectory, and lead to unwanted phase accumulation due to B0 eddy currents8,9.
Several different techniques have been proposed to address gradient imperfections, including data-driven and calibration-based approaches like RING7 and gradient impulse response function (GIRF)3,10, respectively. This study aims to compare these approaches for addressing gradient imperfections in free-breathing, confounder-corrected T1 mapping11 for abdominal imaging.
Methods
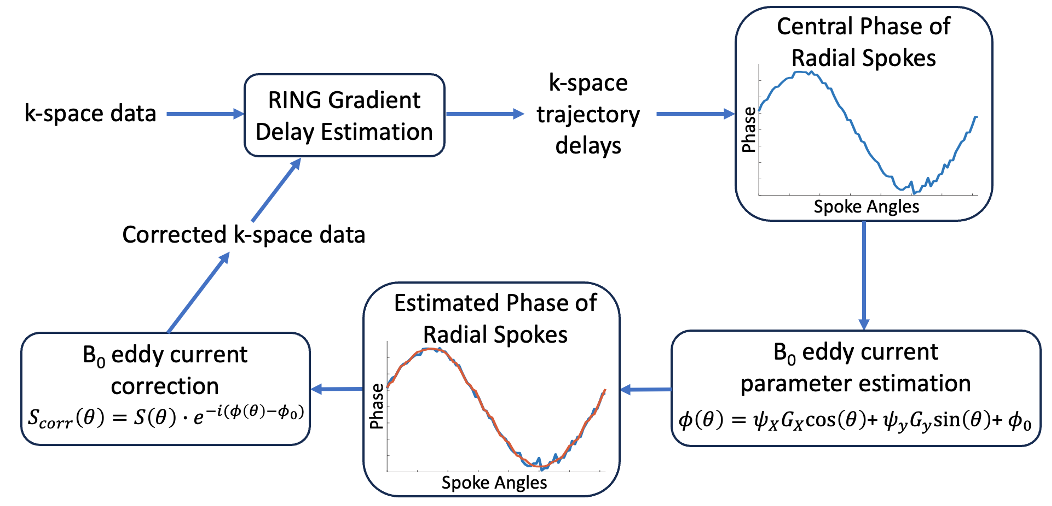
Data-Driven Correction: RING is a data-driven method used for estimating gradient delays directly from the k-space data7. However, B0 eddy currents introduce additional phase errors in k-space, leading to unreliable delay estimations with RING. Errors in gradient delay estimations may also hamper the correction of B0 eddy current effects, since determining the central point of radial spokes is crucial for this process9. To accurately estimate gradient delays and correct for B0 eddy current effects, we developed a novel iterative approach, summarized in Figure 1.Calibration-Based Correction: Unlike RING, GIRF can avoid the effects of B0 eddy currents by measuring gradient responses independently in orthogonal directions10,12. The k-space trajectory can be corrected according to GIRF calibration, and the corrected trajectory can, subsequently, be used to address B0 eddy current effects9.
Phantom Experiments: Phantom experiments were performed on a 3.0T clinical PET/MR system (GE Signa PET/MR, GE HealthCare, Waukesha WI). Two different phantoms were used for imaging: i) a vendor provided doped water phantom, ii) an in-house agar-gel phantom with varying T1 (200-1000 msec) and proton density fat fractions (PDFF) (0-20%).
In Vivo Experiments: Experiments were performed on a healthy volunteer on the same MRI system using a 48-channel phased-array coil.
Chemical shift encoded (CSE)-MRI (IDEAL-IQ, GE HealthCare, Waukesha, WI) was used as a reference for PDFF and R2* maps, while a saturation recovery T1 mapping method (SMART1Map, GE Healthcare, Waukesha, WI) was used as a reference for T1 map13,14.
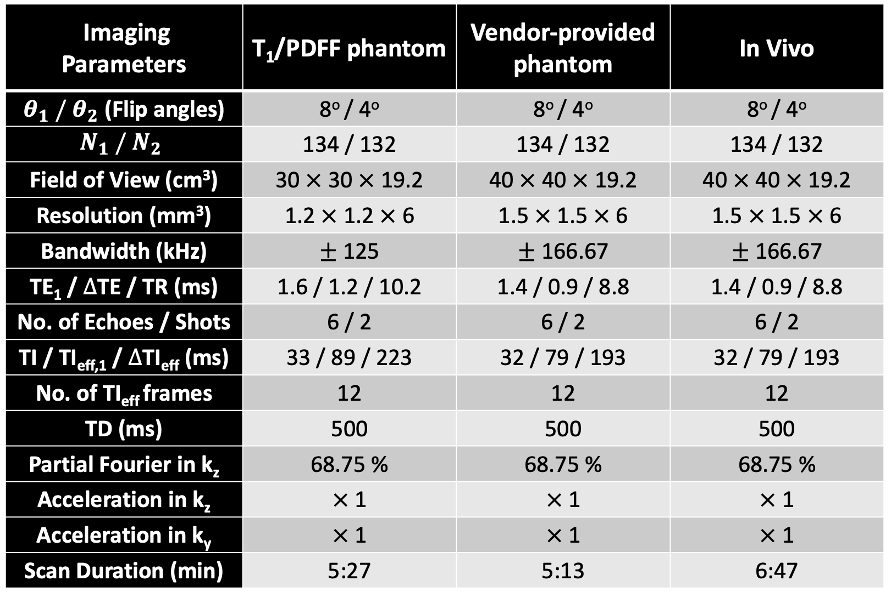
Confounder-corrected T1 maps were obtained using a SoS, inversion-recovery, CSE-MRI method11, with the imaging parameters detailed in Figure 2. The non-Cartesian k-space data were reconstructed under the following conditions: i) without any gradient correction, ii) with a single iteration of the data-driven correction, iii) with three iterations of the data-driven correction, and iv) with the calibration-based correction. Based on empirical evidence, three iterations of the data-driven method were sufficient for a good image quality.
Results
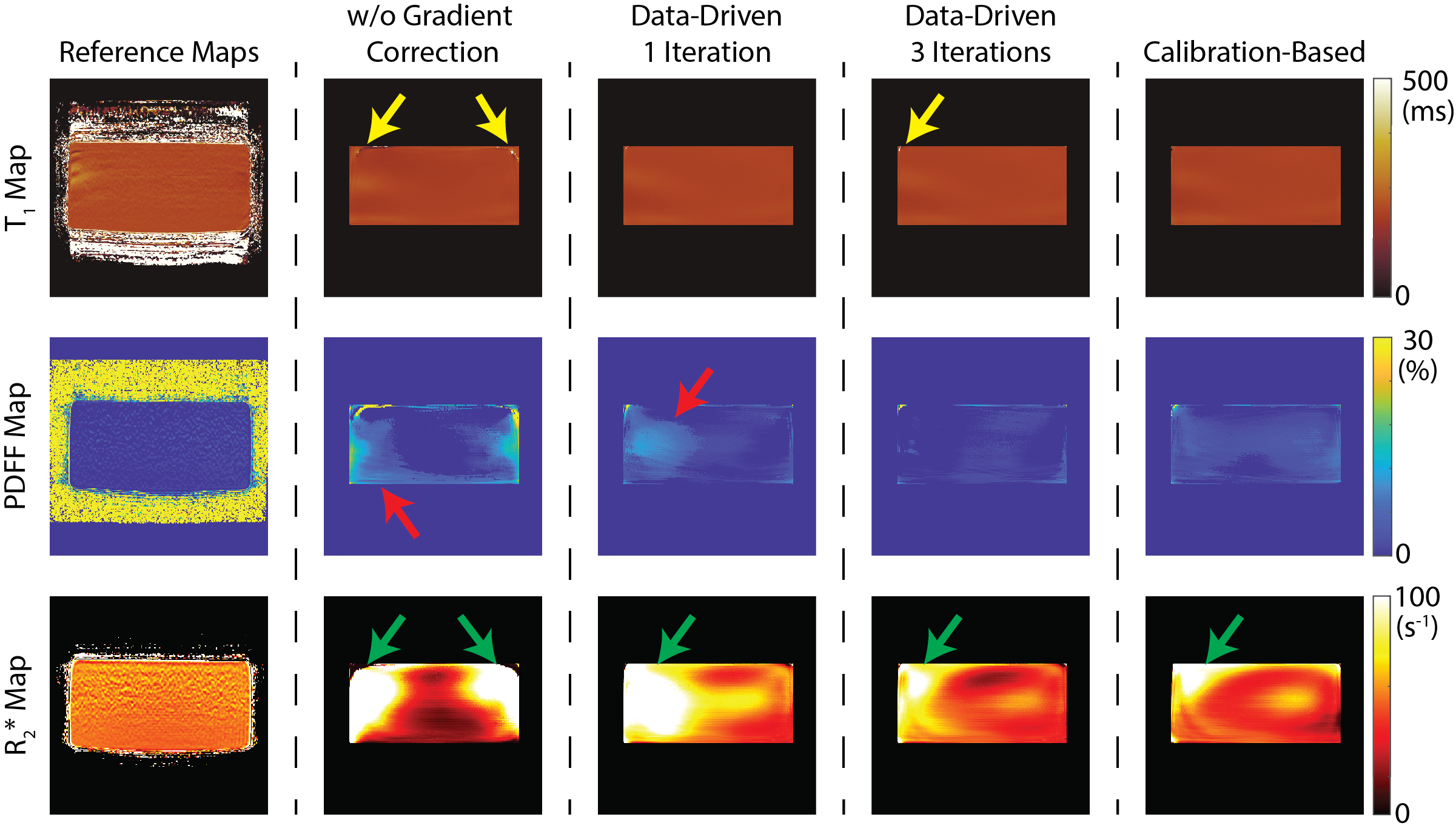
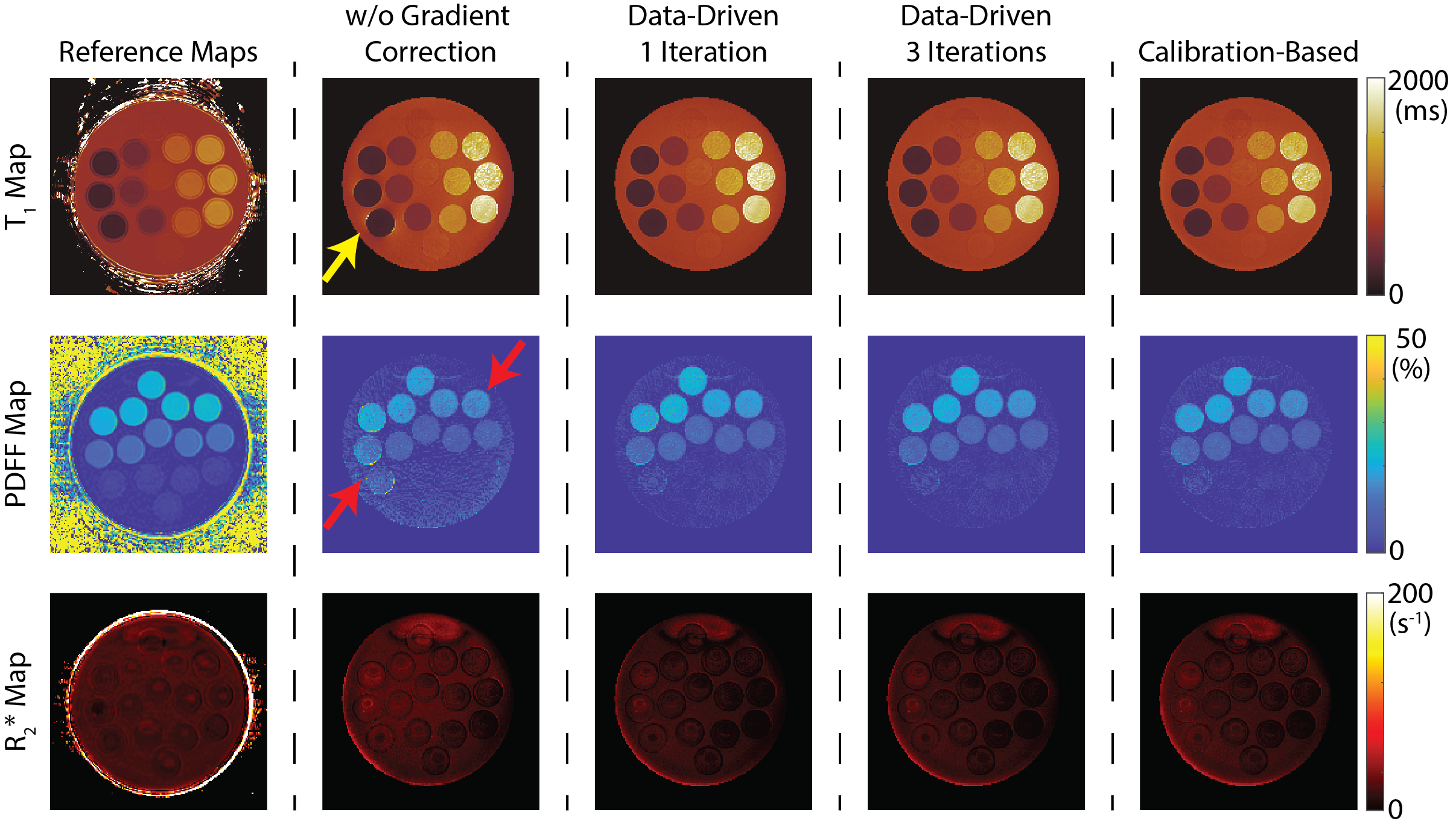
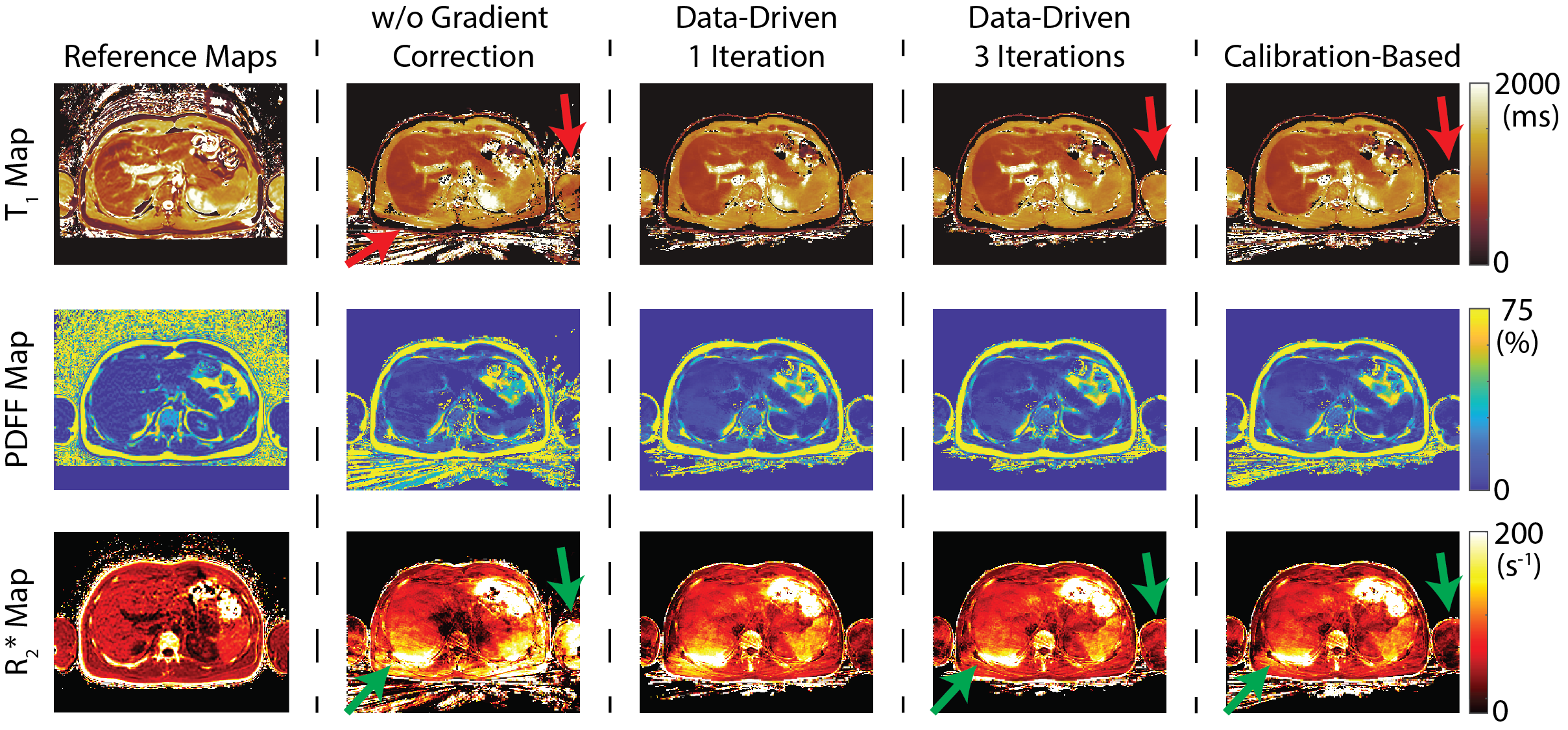
Phantom Experiments: Figures 3 and 4 illustrate the impact of gradient imperfections and the effectiveness of various correction methods in SoS, confounder-corrected T1 mapping. In Figure 3, confounder-corrected T1 maps from a vendor-provided phantom are presented. Without gradient correction, PDFF and R2* measurements exhibit noticeable bias. A single iteration of the data-driven correction method reduced bias in the PDFF map but does not eliminate it entirely. However, the data-driven approach significantly improves results with just three iterations, producing comparable outcomes to the calibration-based correction method.Figure 4 presents quantitative maps obtained from the agar-gel phantom. Maps reconstructed without gradient correction exhibit poor signal-to-noise ratio (SNR) performance in the PDFF map and display bias in the T1 map. Conversely, the bias is eliminated with the other gradient correction approaches.In Vivo Experiments: Figure 5 illustrates the performance of gradient correction methods in a healthy subject. Without gradient correction, substantial bias was evident in quantitative parameter maps, particularly around the arms and the right lobe of the liver. The correction algorithms helped mitigate this bias, although some residual R2* bias was still observed in the right-posterior lobe of the liver.
Discussion and Conclusion
This work investigated the impact of gradient imperfections and the efficacy of different correction methods in non-Cartesian, confounder-corrected T1 mapping using phantom and in vivo imaging experiments. Preliminary findings indicate that gradient imperfections introduce significant bias in PDFF and R2* maps, although T1 maps appear to be less sensitive to such errors. Gradient correction approaches (RING and GIRF) help mitigate these errors. We continue to observe bias in in vivo R2* maps, even after the application of gradient correction algorithms, although this may be due to ineffective motion correction. Future research will focus on further characterizing the bias related to gradient imperfections and developing a robust correction method.Acknowledgements
We wish to acknowledge investigator-initiated research support from Bayer, UW Institute for Clinical and Translational Research, and the Clinical and Translational Science Award of the NCATS/NIH (UL1TR002373). Further, we wish to acknowledge GE Healthcare who provides research support to the University of Wisconsin. Finally, Dr. Reeder is the John. H Juhl Endowed Chair of Radiology.References
[1] Block KT, Chandarana H, Milla S, et al. Toward routine clinical use of radial stack-of-stars 3D gradient-echo sequences for reducing motion sensitivity. J Korean Soc Magn Reson Med 2014; 18:87-106.
[2] Chandarana H, Block TK, Rosenkrantz AB, et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol. 2011;46:648–653.
[3] Stich M, Wech T, Slawig A, Ringler R, Dewdney A, Greiser A, Ruyters G, Bley TA, Köstler H. Gradient waveform pre-emphasis based on the gradient system transfer function. Magn Reson Med. 2018 Oct;80(4):1521-1532.
[4] Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014; 72:707-717.
[5] Reeder SB, Atalar E, Faranesh AZ, McVeigh ER. Referenceless interleaved echo-planar imaging. Magn Reson Med. 1999 Jan;41(1):87-94.
[6] Peters, D.C., Derbyshire, J.A. and McVeigh, E.R. (2003), Centering the projection reconstruction trajectory: Reducing gradient delay errors. Magn. Reson. Med., 50: 1-6.
[7] Rosenzweig, S, Holme, HCM, Uecker, M. Simple auto-calibrated gradient delay estimation from few spokes using Radial Intersections (RING). Magn Reson Med. 2019; 81: 1898–1906.
[8] Brodsky EK, Klaers JL, Samsonov AA, Kijowski R, Block WF. Rapid measurement and correction of phase errors from B0 eddy currents: impact on image quality for non-Cartesian imaging. Magn Reson Med. 2013 Feb;69(2):509-15.
[9] Moussavi, A., Untenberger, M., Uecker, M. and Frahm, J. (2014), Correction of gradient-induced phase errors in radial MRI. Magn. Reson. Med, 71: 308-312.
[10] Vannesjo, S.J., Haeberlin, M., Kasper, L., Pavan, M., Wilm, B.J., Barmet, C. and Pruessmann, K.P. (2013), Gradient system characterization by impulse response measurements with a dynamic field camera. Magn Reson Med, 69: 583-593.
[11] Muslu Y, Cashen TA, Mandava S, Hernando D, Reeder SB. Free-Breathing, Confounder-Corrected, 3D T1 Mapping of the Liver through Simultaneous Estimation of T1, PDFF, R2* and B1+. In Proceedings of 32nd Annual Meeting of ISMRM, Toronto, ON, Canada, 2023.
[12] Jang H, McMillan AB. A rapid and robust gradient measurement technique using dynamic single-point imaging. Magn Reson Med. 2017 Sep;78(3):950-962.
[13] Hernando, D., Kramer, J.H. and Reeder, S.B. (2013), Multipeak fat-corrected complex R2* relaxometry: Theory, optimization, and clinical validation. Magn. Reson. Med., 70: 1319-1331.
[14] Slavin GS, Stainsby JA. True T1 mapping with SMART1Map (saturation method using adaptive recovery times for cardiac T1 mapping): a comparison with MOLLI. Journal of Cardiovascular Magnetic Resonance. 2013;15(1):P3. doi:10.1186/1532-429X-15-S1-P3
Figures