3906
Quantification of Tau in the Piriform Cortex in AD using MR-PET1Department of Radiology, Stanford University School of Medicine, Stanford, CA, United States, 2Department of Neurology, Stanford University School of Medicine, Stanford, CA, United States, 3Wu Tsai Neuroscience Institute, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Alzheimer's Disease, Alzheimer's Disease, MR-PET
Motivation: Olfactory dysfunction can be an early sign of Alzheimer’s disease (AD), but involvement of primary olfactory piriform cortex in AD pathology is unknown.
Goal(s): We use Tau MR-PET to compare piriform cortex uptake to the adjacent medial temporal lobe across the progression of AD pathology.
Approach: Using PI-2620 Tau MR-PET, we manually segmented and computed piriform tau compared to automatically segmented medial temporal uptake in amyloid negative/positive healthy controls, mild cognitive impairment, and AD subjects.
Results: Piriform tau uptake increases ordinally with disease severity and is significantly different higher in amyloid positive compared to negative controls.
Impact: We show early increases in piriform cortex tau uptake that closely track adjacent medial temporal regions. This not only explains deficits in olfaction early in AD but opens the door to more sensitive testing and comprehensive detection of neurodegeneration.
Introduction:
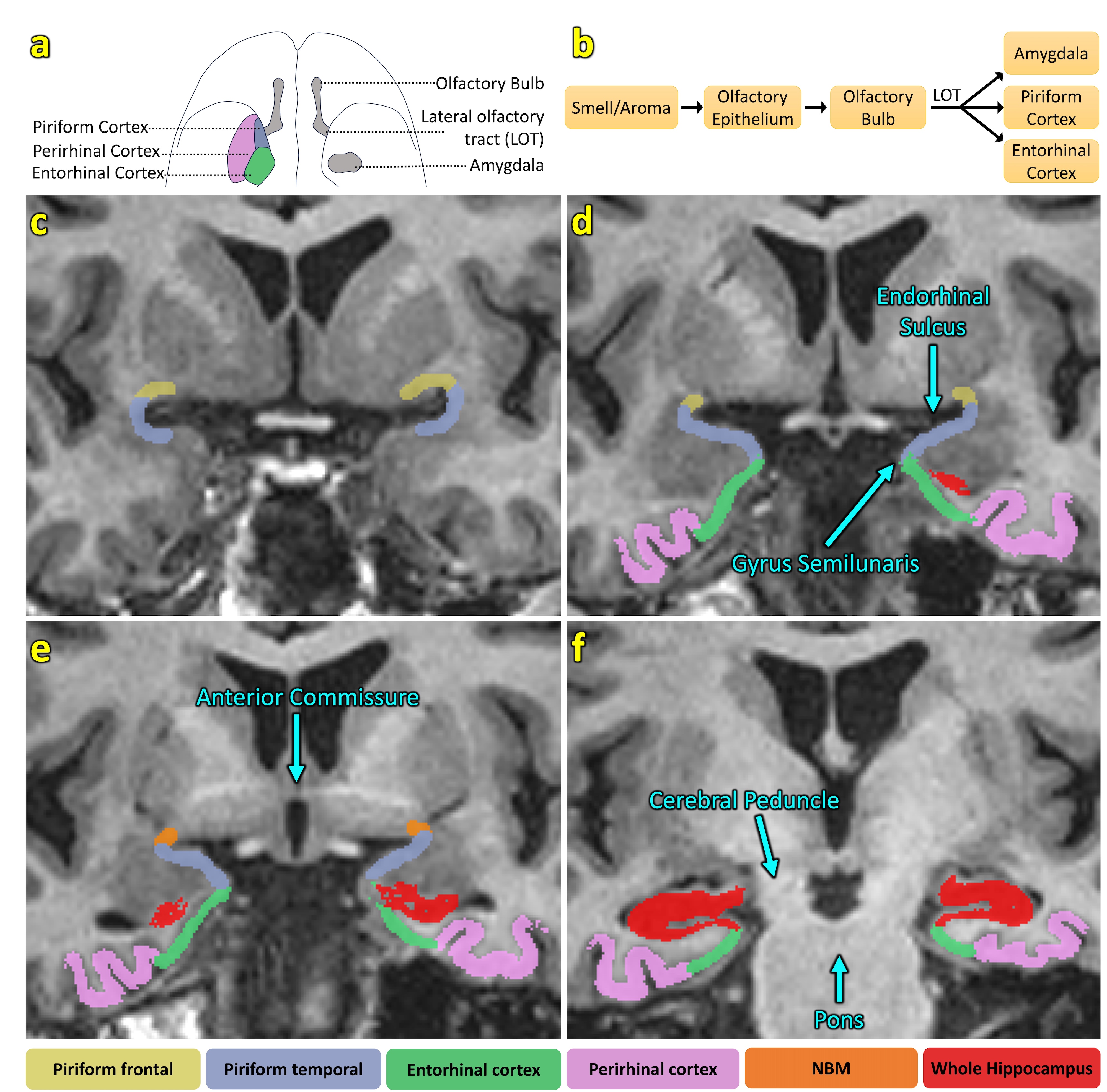
Alzheimer's disease (AD) is widespread across the globe and is the primary cause of dementia among the elderly population1. Accompanying AD is an impaired sense of smell2–4. Olfactory deficiency, or hyposmia, can be present in preclinical AD and predict the subsequent manifestation of mild cognitive impairment (MCI) and AD in the absence of other observable symptoms5–7. Analyzing key regions within the olfactory circuit could reveal important insights into the neuropathological progression. Dysfunction in the olfactory circuit has been shown in the olfactory nerve in limited postmortem studies8, including involvement of the piriform cortex9. FDG-positron emission tomography (PET) and fMRI have shown differential and reduced piriform cortex metabolism and activation in AD, respectively10,11. Thus, the piriform cortex is a promising candidate in the early identification of neurodegenerative pathology underlying olfaction.Tau-PET radiotracers such as 18F-AV-1451 have proven effective for assessing tau pathology in vivo in AD12, though affinity is lower in the earlier stages of AD13. New tau-PET tracer candidates such as 18F-PI-2620 tracer display higher affinity for hyperphosphorylated tau14,15. The piriform cortex has not been examined with any form of tau-PET imaging, and links between noninvasive tau imaging and early olfaction deficiency are lacking9.
Our goal in this study is to measure and compare tau uptake in the piriform cortex across the stages of AD in comparison to regions of the medial temporal lobe. We used 18F-PI-2620 MR-PET to measure tau uptake in the piriform cortex, entorhinal and perirhinal cortices, amygdala, and hippocampus, cross-sectionally examining AD, mild cognitive impairment (MCI), and amyloid positive and negative healthy controls (HC).
Methods:
We analyzed data from 102 subjects: 22 were excluded due to incomplete data, leaving 31 amyloid negative and 25 amyloid positive healthy controls (Amyloid–HC and Amyloid+HC, respectively), 8 mild cognitive impairment (MCI), and 16 Alzheimer’s disease (AD). All subjects underwent MR-PET in a GE 3.0T scanner using tau tracer PI-2620 with a simultaneous coregistered sagittal T1-weighted 3D IR-FSPGR and either a simultaneous or recently acquired coronal T2-weighted FSE. We coregistered all MR sequences and PET using NiftyReg. Automatic Segmentation of Hippocampal Subfields was performed to segment hippocampal subfields, including the entorhinal/perirhinal cortices (Fig. 1D-F). Using ITK-SNAP16 on the coregistered MR images and referencing published piriform segmentation guidelines17, we manually segmented blind to subject diagnosis the frontal and temporal portions of the piriform cortex (Fig. 1C). All segmentations underwent multiple independent quality control checks. Because the tau distributions appeared non-normal among the four ordinal patient categories (Amyloid–HC, Amyloid+HC, MCI, AD), we used a nonparametric Jonckheere-Terpstra test in Stata to test for ordinal increase in tau uptake across three regions bilaterally (whole hippocampus=CA1-4 + DG + subiculum, entorhinal/perirhinal, and piriform).Results:
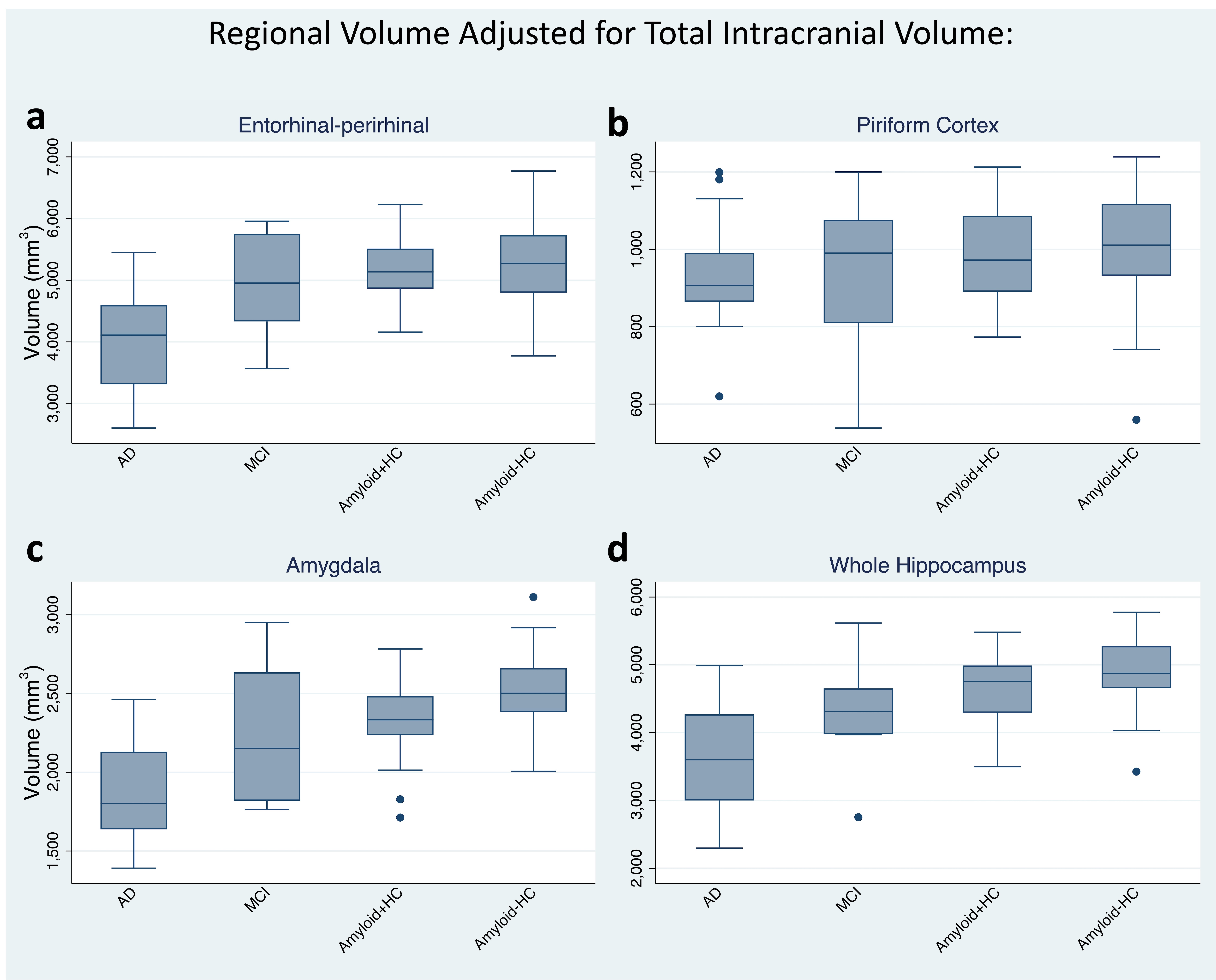
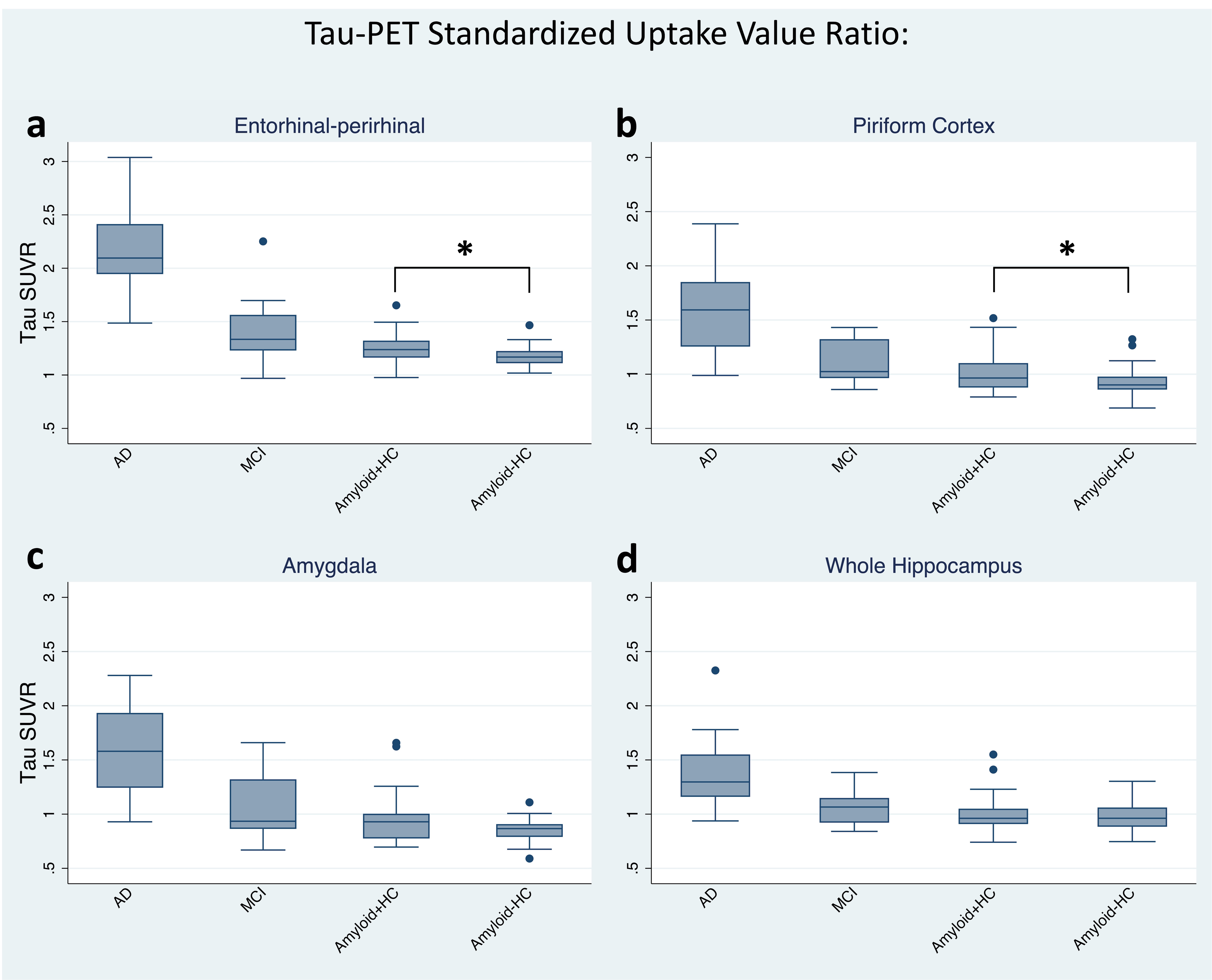
Volume: The volume was inversely associated with disease severity such that AD had the lowest volume followed by MCI, and HC (amyloid+ and -) in all four regions: Entorhinal-perirhinal (J*=3.825, p<0.001), piriform (J*=2.046, p=0.020), amygdala (J*=5.149, p<0.001), and whole hippocampus (J*=4.851, p<0.001) (Fig. 2).Tau SUVr: Tau uptake was positively associated with disease severity in all four regions: Entorhinal-perirhinal (J*=-6.262, p<0.001) piriform, (J*=-5.753, p<0.001), amygdala (J*=-5.166, p<0.001), and whole hippocampus (J*=-4.316, p<0.001). Ranksum tests showed that amyloid+HC had more tau than amyloid-HC in piriform (p=0.049) and entorhinal/perirhinal (p=0.047) but not in amygdala (p=0.207) or whole hippocampus (p=0.786) (Fig. 3).
Discussion:
This work suggests by noninvasive MR-PET that early tau deposition in the piriform cortex may explain early smell loss in AD. Supporting the known but only minimally studied pathological appearance of piriform tau in AD, we found increasing tau uptake cross-sectionally in our study. The uptake was stronger in the temporal compared to the frontal piriform, which could relate to its closer proximity to the transentorhinal region. We further found that only piriform and entorhinal/perirhinal tau were statistically different between amyloid positive and negative healthy controls, suggesting that piriform tau uptake is an early event in AD. Future work will correlate this uptake with quantification of olfactory function.Conclusion:
We show significant changes in the olfactory circuit noninvasively with tau MR-PET, with early increases in piriform cortex tau uptake closely tracking adjacent medial temporal regions. This may explain deficits in olfaction early in AD and could open the door to more sensitive testing and detection of neurodegeneration.Acknowledgements
This study was funded by the NIH (P30AG066515, R21AG058859, R01AG048076, R01AG74339, R01AG061120, K99AG071837), the Alzheimer’s Association (AARFD-21-849349), the Good Planet Foundation, the Stanford Wu Tsai Neuroscience Institute, and the Stanford Precision Health and Integrated Diagnostics (PHIND) Center.References
1. Tahami Monfared AA, Byrnes MJ, White LA, Zhang Q. Alzheimer’s Disease: Epidemiology and Clinical Progression. Neurol Ther. 2022;11(2):553-569. doi:10.1007/S40120-022-00338-8/TABLES/4
2. Tian Q, Bilgel M, Moghekar AR, Ferrucci L, Resnick SM. Olfaction, Cognitive Impairment, and PET Biomarkers in Community-Dwelling Older Adults. J Alzheimers Dis. 2022;86(3):1275-1285. doi:10.3233/JAD-210636
3. Misiak MM, Hipolito MS, Ressom HW, Obisesan TO, Manaye KF, Nwulia EA. Apo E4 Alleles and Impaired Olfaction as Predictors of Alzheimer’s Disease. Clin Exp Psychol. 2017;3(4). doi:10.4172/2471-2701.1000169
4. Goodsmith MS, Wroblewski KE, Schumm LP, Ma MK, Mcclintock JM, Pinto N®. Association of APOE ε4 Status With Long-term Declines in Odor Sensitivity, Odor Identification, and Cognition in Older US Adults. Neurology. 2023;101(13):e1341-e1350. doi:10.1212/WNL.0000000000207659
5. Wilson RS, Schneider JA, Arnold SE, Tang Y, Boyle PA, Bennett DA. Olfactory Identification and Incidence of Mild Cognitive Impairment in Older Age. Arch Gen Psychiatry. 2007;64(7):802-808. doi:10.1001/ARCHPSYC.64.7.802
6. Wilson RS, Arnold SE, Schneider JA, Boyle PA, Buchman AS, Bennett DA. Olfactory Impairment in Presymptomatic Alzheimer’s Disease. Ann N Y Acad Sci. 2009;1170(1):730-735. doi:10.1111/J.1749-6632.2009.04013.X
7. Rajani V, Yuan Q. Noradrenergic Modulation of the Piriform Cortex: A Possible Avenue for Understanding Pre-Clinical Alzheimer’s Disease Pathogenesis. Front Cell Neurosci. 2022;16. doi:10.3389/fncel.2022.908758
8. Bathini P, Mottas A, Jaquet M, Brai E, Alberi L. Progressive signaling changes in the olfactory nerve of patients with Alzheimer’s disease. Neurobiol Aging. 2019;76:80-95. doi:10.1016/J.NEUROBIOLAGING.2018.12.006
9. Saiz-Sanchez D, De la Rosa-Prieto C, Ubeda-Banon I, Martinez-Marcos A. Interneurons, tau and amyloid-β in the piriform cortex in Alzheimer’s disease. Brain Struct Funct. 2015;220(4):2011-2025. doi:10.1007/S00429-014-0771-3/FIGURES/9
10. Kareken DA, Doty RL, Moberg PJ, et al. Olfactory-evoked regional cerebral blood flow in Alzheimer’s disease. Neuropsychology. 2001;15(1):18-29. doi:10.1037/0894-4105.15.1.18
11. Li W, Howard JD, Gottfried JA. Disruption of odour quality coding in piriform cortex mediates olfactory deficits in Alzheimer’s disease. Brain. 2010;133(9):2714-2726. doi:10.1093/BRAIN/AWQ209
12. Young CB, Winer JR, Younes K, et al. Divergent Cortical Tau Positron Emission Tomography Patterns Among Patients With Preclinical Alzheimer Disease. Published online 2022. doi:10.1001/jamaneurol.2022.0676
13. Lowe VJ, Curran G, Fang P, et al. An autoradiographic evaluation of AV-1451 Tau PET in dementia. Acta Neuropathol Commun. 2016;4(1). doi:10.1186/S40478-016-0315-6
14. Kroth H, Oden F, Molette J, et al. Discovery and preclinical characterization of [18F]PI-2620, a next-generation tau PET tracer for the assessment of tau pathology in Alzheimer’s disease and other tauopathies. Eur J Nucl Med Mol Imaging. 2019;46(10):2178-2189. doi:10.1007/S00259-019-04397-2/FIGURES/5
15. Mormino EC, Toueg TN, Azevedo C, et al. Tau PET imaging with 18F-PI-2620 in aging and neurodegenerative diseases. Eur J Nucl Med Mol Imaging. 2021;48(7):2233. doi:10.1007/S00259-020-04923-7
16. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116-1128. doi:10.1016/J.NEUROIMAGE.2006.01.015
17. Iqbal S, Leon-Rojas JE, Galovic M, et al. Volumetric analysis of the piriform cortex in temporal lobe epilepsy. Epilepsy Res. 2022;185:106971. doi:10.1016/J.EPLEPSYRES.2022.106971Figures