3893
Gas-free cerebrovascular reactivity predicts cognition in older individuals1Diagnostic Radiology, University of Maryland School of Medicine, Baltimore, MD, United States, 2Radiology, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Keywords: Dementia, Neurodegeneration, Biomarkers, Diagnosis/Prediction
Motivation: Small-vessel-disease (SVD), a contributing risk factor in vascular cognitive impairment and dementia (VCID), needs sensitive biomarkers to assess the brain.
Goal(s): Our goal is to evaluate whether gas-free cerebrovascular reactivity (CVR) can predict cognitive function in older individuals.
Approach: We performed gas-free CVR mapping with intermittent breath modulation in two studies of elderly individuals and evaluated the relationship between gas-free CVR and global cognition.
Results: Higher whole-brain gas-free CVR was correlated with better MoCA scores.
Impact: Gas-free cerebrovascular reactivity (CVR) using intermittent breath modulation can be used as a practical tool to evaluate cerebrovascular function and probe vascular pathology in small-vessel-disease (SVD) and vascular cognitive impairment and dementia (VCID).
INTRODUCTION
Small-vessel-disease (SVD) related vascular contributions to cognitive impairment (VCI) represent a major cause of cognitive dysfunction in older individuals, as up to 80% of patients with Alzheimer’s Disease (AD) have vascular pathology1. Furthermore, vascular pathology increases the patient’s risk to develop Amyloid Related Imaging Abnormalities (ARIA), a new imaging syndrome after receiving anti-amyloid immunotherapy2. Therefore, characterizing vascular pathology using noninvasive biomarkers is urgently needed. Cerebrovascular reactivity (CVR), an index of cerebral vessel’s capacity to dilate in response to vasostimulation, is a highly promising biomarker to assess VCI. Previous studies demonstrated a positive correlation between CVR measured with CO2 inhalation and global cognition measured with Montreal-Cognitive-Assessment (MoCA)3, which was reproduced by different sites and cohorts4. However, CVR measurement using CO2 inhalation requires considerable subject cooperation and special gas delivery systems, which limits its utilization in clinical applications. Recently, we developed a new CVR mapping technique using intermittent breath modulation which does not require gas inhalation5. Here we apply this gas-free CVR technique, bm-CVR, in a group of older individuals with mild-cognitive-impairment (MCI), mild dementia, and normal cognition, and study the relationship between whole-brain CVR and global cognition. We also aim to validate the findings in a second group of elderly in an ongoing study. Our hypothesis is that gas-free CVR using intermittent breath modulation can predict global cognition in older individuals.METHODS
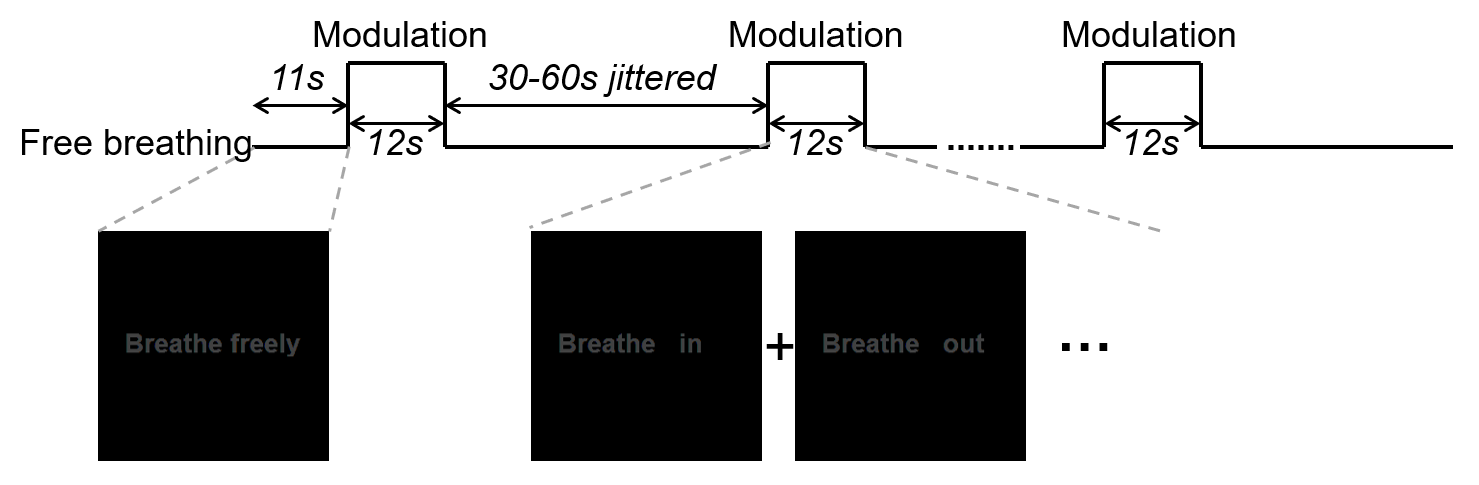
Participants: Study 1 was conducted in 59 older subjects (28M/31F), aged 70.5 ± 7.4 years (18 cognitively normal, 34 MCI, and 7 mild dementia). Participants were enriched for vascular risks. Study 2 is an ongoing study aiming to enroll 90 older subjects (55-90 years) in total with the same enrollment criteria as Study 1, in which 20 subjects (6M/14F), aged 68.4 ± 6.7 years (7 cognitively normal, and 13 MCI) were enrolled. For each participant, the global cognition was assessed via MoCA.MRI: The participants underwent bm-CVR scans on 3T MRI systems. During the intermittent breath modulation task, the subjects were asked to breathe at their own pace except for the periods when pacing instructions, “breathe in” or “breathe out”, appear on the screen. The pacing instructions appear for 12 seconds after every 30-60s free breathing period (Figure 1). The pacing frequency was 6s/breath (3s in/3s out) for Study 1 and 4s/breath (2s in/2s out) for Study 2, respectively. BOLD data was collected during the bm-CVR scans (TR/TE=1500/21ms, 3.4x3.4x3.8mm3 resolution, 9.3min scan duration in Study 1; TR/TE=720/37ms, 2x2x2mm3 resolution, 7min scan duration in Study 2). End-tidal carbon dioxide (EtCO2) was recorded with a nasal cannula during the scan using a capnograph device. Analysis of the gas-free CVR data followed the method described previously5. Briefly, after standard pre-processing, whole-brain CVR was obtained using GLM analysis where the whole-brain BOLD time course (low-pass filtered at 0.08Hz) was the dependent variable, EtCO2 time course was the independent variable, and motion vectors and a linear trend were included as covariates.
Statistical Analysis: For each study, a multi-linear regression model was used to test the associations between gas-free CVR and MoCA, with age, gender, and years of education as co-variates.
RESULTS
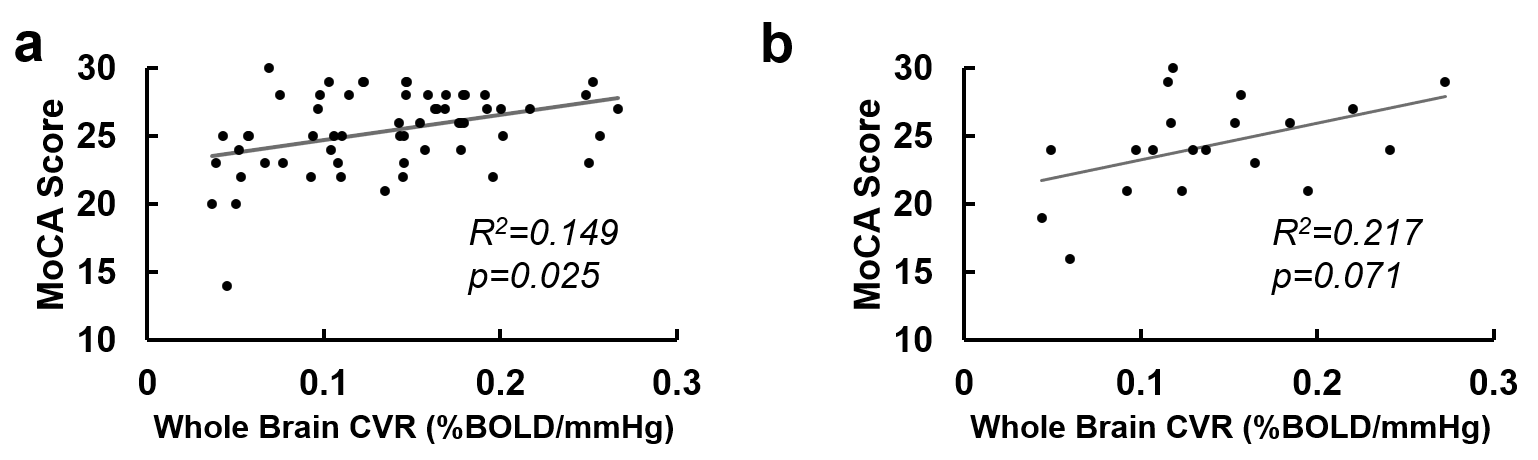
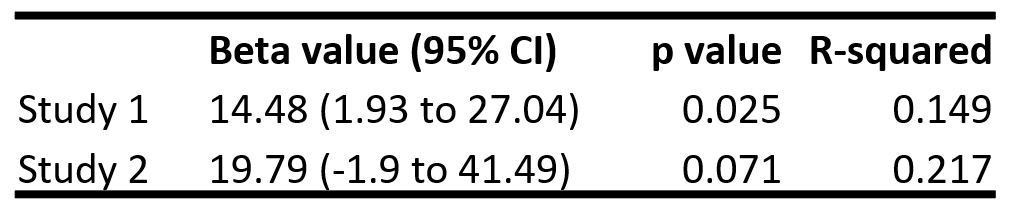
Table 1 summarizes the participant demographics of the two studies. Whole-brain CVR values were 0.137±0.060 %mmHg and 0.139±0.061 %mmHg for Study 1 and Study 2, respectively, with no significant difference between the two studies (p=0.44). Figure 2 shows the scatter plots between gas-free CVR and MoCA in both studies, and the statistical analysis results are summarized in Table 2. In Study 1 with 59 subjects, higher gas-free CVR was significantly associated with better MoCA score (p=0.025, Figure 2a), after accounting for age, gender and education differences. In Study 2, with only 20 subjects enrolled so far, gas-free CVR showed a trend for positive correlation with MoCA (p=0.071, Figure 2b).DISCUSSION AND CONCLUSION
In the present work we quantified whole-brain CVR using intermittent breath modulation in two different cohorts of older individuals, and evaluated its predictive value for global cognition measured by MoCA. In both cohorts, higher CVR was correlated with better MoCA score. This finding is consistent with that observed with conventional CVR mapping using CO2 inhalation3, 4. Compared to conventional CVR mapping methods, the gas-free CVR with intermittent breath modulation eliminates the need for gas delivery systems, and is also more comfortable to the participants than CO2 inhalation or breathing-holding5. Therefore, this gas-free CVR technique can be used as a more practical tool to evaluate cerebrovascular function and probe vascular pathology in patients with SVD and VCID.Acknowledgements
No acknowledgement found.References
1. Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007; 69: 2197-2204.
2. van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, Kanekiyo M, Li D, Reyderman L, Cohen S, Froelich L, Katayama S et al. Lecanemab in Early Alzheimer's Disease. N Engl J Med 2023; 388: 9-21.
3. Sur S, Lin Z, Li Y, Sevil Y, Rosenberg P, Abhay M, Hou X, Rita K, Hazel K, Pottanat G, Xu C, van Zijl P et al. Cerebrovascular reactivity predicts cognitive performance independent of Alzheimer pathology. Neurology 2020; In press.
4. Liu P, Lin Z, Hazel K, Pottanat G, Xu C, Jiang D, Lucke E, Bauer CE, Gold BT, Greenberg SM, Helmer KG, Jann K et al. Cerebrovascular reactivity (CVR) MRI as a biomarker for small vessel disease related cognitive decline: validation in the MarkVCID Consortium. Proc Intl Soc Mag Reson Med; Toronto, CA2023. p. 408.
5. Liu P, Xu C, Lin Z, Sur S, Li Y, Yasar S, Rosenberg P, Albert M, Lu H. Cerebrovascular reactivity mapping using intermittent breath modulation. Neuroimage 2020; 215: 116787.
Figures