3887
Cognitive impairment is associated with elevated oxygen extraction and metabolism in the medial temporal lobe1Department of Biomedical Engineering, Johns Hopkins University School of Engineering, Baltimore, MD, United States, 2Department of Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Neuroscience, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Division of Geriatric Psychiatry and Neuropsychiatry, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 5Division of Geriatric Medicine and Gerontology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 6Division of Endocrinology, Diabetes, and Metabolism, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 7Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: Aging, Neurodegeneration
Motivation: Currently, the primary MRI-based biomarker for cognitive dysfunction is the atrophy of medial-temporal-lobe (MTL). However, MTL atrophy represents a late stage of tissue damage. Functional biomarkers such as the MTL oxygen metabolism may be more sensitive in early stages.
Goal(s): To evaluate the association of MTL oxygen metabolism with cognitive function in non-demented elderly individuals.
Approach: We used a novel MRI technique to evaluate the MTL oxygen metabolism in 48 elderly subjects. Cognitive function of the participants was assessed.
Results: Worse cognitive scores were associated with elevated oxygen extraction and metabolic rate in the MTL, but not with the volume of MTL.
Impact: Our findings indicated that measuring the oxygen extraction and metabolic rate in the medial temporal lobe may be more sensitive than structural atrophy in detecting tissue damage in early stages of cognitive impairment.
INTRODUCTION
The medial-temporal-lobe (MTL) is critical in human cognitive function, particularly in memory formation. Currently, MTL atrophy is the primary MRI-based biomarker for cognitive dysfunction1,2. Unfortunately, brain atrophy typically signifies a late stage of tissue damage and is generally considered irreversible. Since oxygen metabolism is the predominant energy source for the human brain, functional biomarkers such as oxygen-extraction-fraction (OEF) and cerebral-metabolic-rate-of-oxygen (CMRO2) in the MTL may offer greater sensitivity to tissue injury in the early stages of cognitive dysfunction.Recently, a novel MRI technique, arterial-suppressed-accelerated-T2-relaxation-under-phase-contrast (AS-aTRUPC)3, has been developed for non-invasive assessment of MTL-OEF. In this study, we utilized AS-aTRUPC in combination with pseudo-continuous-arterial-spin-labeling (pCASL) to evaluate oxygen metabolism in the MTL of non-demented elderly individuals and investigated the relationship between cognitive function and MTL oxygen metabolism.
METHODS
Participants: Forty-eight elderly subjects (31 females, 72.3±5.6 years old) were included in this IRB-approved study. Cognitive function of the participants was assessed using Montreal Cognitive Assessment (MoCA)4 (N=46) or Clinical Dementia Rating Sum of Boxes score (CDR-SoB)5 (N=43). Table 1 summarizes the characteristics of the participants.MRI Experiments: All MRI experiments were performed on a 3T Siemens Prisma scanner. MTL-OEF was evaluated by AS-aTRUPC using the following parameters3: field-of-view (FoV)=200×200mm2, reconstructed in-plane resolution=0.78×0.78mm2, 3 effective-TEs of 0, 40 and 80ms, and scan duration=4.8min.
Cerebral-blood-flow (CBF) was measured using pCASL with labeling-duration=1.8s and post-labeling-delay=2.2s6. 3D T1-MPRAGE with voxel-size=1.0×1.0×1.0mm3 was acquired for brain parcellation.
Data Processing: The AS-aTRUPC data were analyzed to provide the venous-oxygenation (Yv) in bilateral basal-veins (BVs), which are the major draining veins of the MTL3. OEF was calculated by OEF=(Ya−Yv)/Ya×100%, assuming arterial-oxygenation Ya=98%. The averaged OEF of bilateral BVs was used to represent MTL-OEF.
The T1-MPRAGE images were automatically segmented7 to obtain the volume of MTL (including bilateral amygdalas, hippocampi, and parahippocampal gyri). The MTL-volume was represented as a percentage of the total intracranial volume.
The pCASL data were processed to obtain voxel-wise CBF maps8. Averaged CBF in the MTL was extracted from the CBF maps based on the T1-MPRAGE segmentation.
Finally, MTL-CMRO2 was computed as CMRO2=CBF×OEF×Ya×Ch, where Ch=8.97μmol O2/ml for a hematocrit of 0.449.
Statistical Analysis: We first examined the effects of aging on OEF, CBF and CMRO2 in the MTL using linear regression analyses, with sex as a covariate. Next, to investigate how MTL oxygen metabolism affects cognitive functions, we conducted linear regression analyses in which MoCA or CDR-SoB was the dependent variable and MTL-OEF, MTL-CBF or MTL-CMRO2 was the independent variable, with age, sex, and education (in years) as covariates. These analyses were also repeated for MTL-volume to examine the relationship of MTL atrophy with aging and cognitive decline.
RESULTS
Figure 1 illustrates representative AS-aTRUPC data. As shown, complex subtraction between the reference and flow-encoded images effectively isolates blood signals in the BVs, which show expected T2-decay with increasing effective-TEs. Fitting of the decay function results in the OEF of BVs.We observed a significant age-related increase in MTL-OEF (P=0.02, Figure 2A), consistent with a recent report3. In addition, there was a negative correlation between MTL-OEF and MTL-CBF across the patients (P=0.03, r=−0.34, Figure 2B). No significant aging effect on MTL-CBF or MTL-CMRO2 was found (P>0.5). We also observed a trend towards a negative association of MTL-volume with age (P=0.06).
As shown in Figure 3A, we discovered that higher MTL-OEF was associated with a lower MoCA score (P=0.01). MoCA was not associated with MTL-CBF, MTL-CMRO2, or MTL-volume (P>0.1).
Furthermore, we observed that higher MTL-CMRO2 was associated with a higher CDR-SoB score, indicating worse cognitive function (P=0.03, Figure 4B). No significant association was found between the CDR-SoB score and MTL-OEF, MTL-CBF, or MTL-volume (P>0.1).
DISCUSSION AND CONCLUSION
In this study, we observed that higher MTL-OEF was associated with a lower MoCA score, and elevated CMRO2 was associated with a worse CDR-SoB score, suggesting that hypermetabolism in the MTL may be related to cognitive decline. Our findings were consistent with a few FDG-PET studies that reported elevated MTL glucose metabolism in Alzheimer’s disease10,11. This MTL hypermetabolism may be explained by the hippocampal hyperactivity observed in patients with mild-cognitive-impairment12, which, in turn, may be caused by disinhibition resulting from reduced functional connectivity between the hippocampus and other brain regions13.It is worth noting that MTL-volume showed no significant association with MoCA or CDR-SoB. This indicates that functional biomarkers like MTL-OEF or MTL-CMRO2 may be more sensitive than structural atrophy in the early stages of cognitive dysfunction, given that none of the patients in our cohort had dementia.
In summary, our findings suggest that the quantification of MTL oxygen metabolism may provide sensitive biomarkers for cognitive dysfunction.
Acknowledgements
No acknowledgement found.References
1. Jack CR, Jr., Petersen RC, Xu YC, Waring SC, O'Brien PC, Tangalos EG, Smith GE, Ivnik RJ, Kokmen E. Medial temporal atrophy on MRI in normal aging and very mild Alzheimer's disease. Neurology 1997;49:786-794.
2. Jack CR, Jr., Bennett DA, Blennow K et al. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 2016;87:539-547.
3. Jiang D, Liu P, Lin Z, Hazel K, Pottanat G, Lucke E, Moghekar A, Pillai JJ, Lu H. MRI assessment of cerebral oxygen extraction fraction in the medial temporal lobe. Neuroimage 2023;266:119829.
4. Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-699.
5. O'Bryant SE, Waring SC, Cullum CM, Hall J, Lacritz L, Massman PJ, Lupo PJ, Reisch JS, Doody R, Texas Alzheimer's Research C. Staging dementia using Clinical Dementia Rating Scale Sum of Boxes scores: a Texas Alzheimer's research consortium study. Arch Neurol 2008;65:1091-1095.
6. Alsop DC, Detre JA, Golay X et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015;73:102-116.
7. Mori S, Wu D, Ceritoglu C, Li Y, Kolasny A, Vaillant MA, Faria AV, Oishi K, Miller MI. MRICloud: Delivering High-Throughput MRI Neuroinformatics as Cloud-Based Software as a Service. Computing in Science & Engineering 2016;18:21-35.
8. Li YA-O, Liu P, Li Y et al. ASL-MRICloud: An online tool for the processing of ASL MRI data. NMR Biomed 2019;32:e4051.
9. Peng SL, Dumas JA, Park DC, Liu P, Filbey FM, McAdams CJ, Pinkham AE, Adinoff B, Zhang R, Lu H. Age-related increase of resting metabolic rate in the human brain. Neuroimage 2014;98:176-183.
10. Apostolova I, Lange C, Maurer A et al. Hypermetabolism in the hippocampal formation of cognitively impaired patients indicates detrimental maladaptation. Neurobiol Aging 2018;65:41-50.
11. Chetelat G, Desgranges B, Landeau B, Mezenge F, Poline JB, de la Sayette V, Viader F, Eustache F, Baron JC. Direct voxel-based comparison between grey matter hypometabolism and atrophy in Alzheimer's disease. Brain 2008;131:60-71.
12. Bakker A, Krauss GL, Albert MS, Speck CL, Jones LR, Stark CE, Yassa MA, Bassett SS, Shelton AL, Gallagher M. Reduction of hippocampal hyperactivity improves cognition in amnestic mild cognitive impairment. Neuron 2012;74:467-474.
13. Tahmasian M, Pasquini L, Scherr M et al. The lower hippocampus global connectivity, the higher its local metabolism in Alzheimer disease. Neurology 2015;84:1956-1963.
Figures
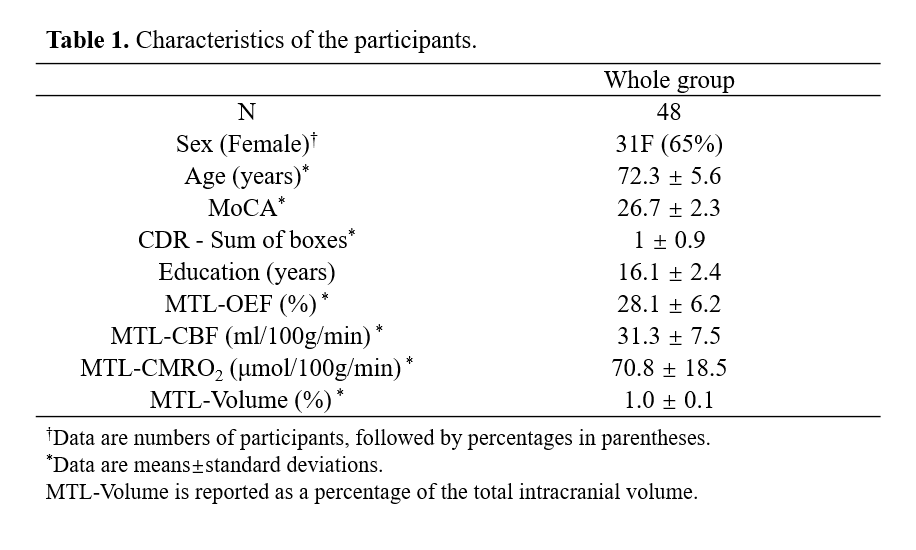
Table 1. Characteristics of the participants.
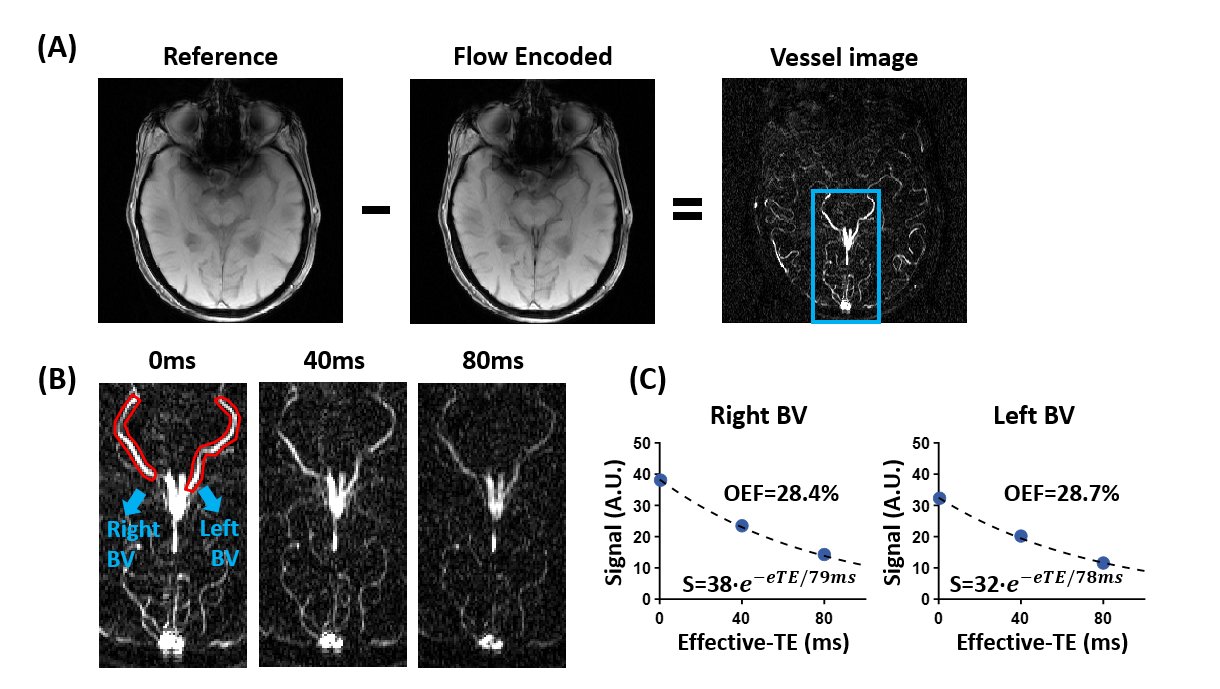
Figure 1. Representative AS-aTRUPC data. (A) AS-aTRUPC uses phase-contrast subtraction between phase-reference and flow-encoded images to yield a vessel image, which contains pure blood signal in the BVs. (B) T2-preparation is utilized to modulate the T2-weighting of the vessel image. Zoom-in views of the vessel image (blue box in A) are shown for all effective-TEs. The bilateral basal-veins (BVs) are highlighted by the red contours. (C) Fitting of the BV signal as a function of effective-TEs gives the OEF.
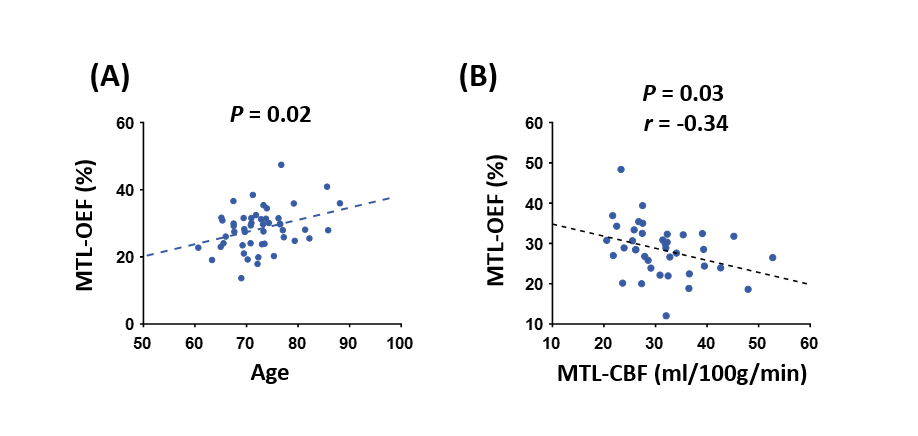
Figure 2. The association of MTL-OEF with aging and MTL-CBF. (A) MTL-OEF increased with age. The plot has been adjusted for sex. (B) MTL-OEF negatively correlated with MTL-CBF.
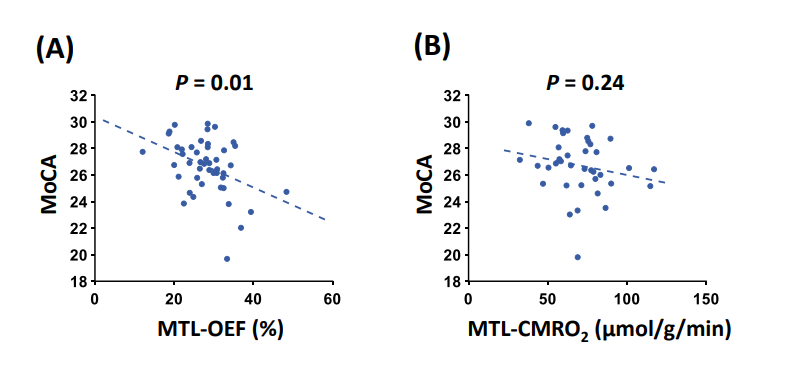
Figure 3. Associations between MoCA scores and MTL-OEF and MTL-CMRO2. All plots have been adjusted for age, sex, and education.
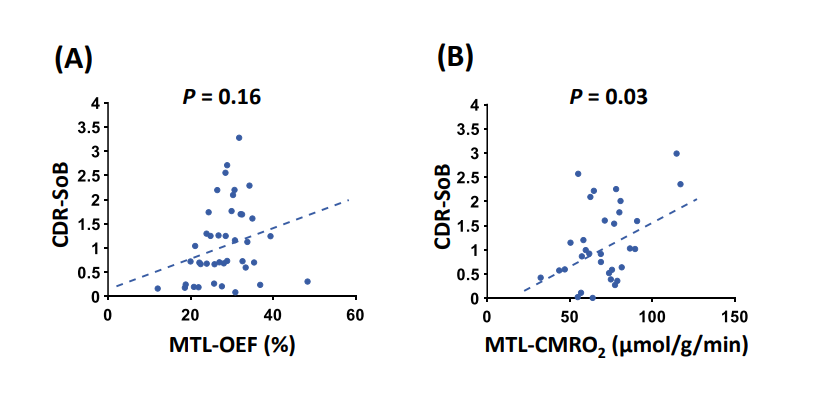
Figure 4. Relationships between CDR-SoB scores and MTL-OEF and MTL-CMRO2. All plots have been adjusted for age, sex, and education.