3883
Microvascular physiology differs in older adults with varying vascular risk and white matter lesion burden1Faculty of Medicine, Kiel University, Kiel, Germany, 2Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 3Department of Radiology, Harvard Medical School, Boston, MA, United States
Synopsis
Keywords: Aging, Oxygenation
Motivation: While links between microvascular physiology and white matter lesion burden have largely been studied in older adults with high vascular risk, some individuals exhibit high lesion burden despite presenting with low vascular risk.
Goal(s): To determine whether associations between hemo-metabolic physiology and lesion burden vary in older adults according to vascular risk.
Approach: We compared MRI-based measures of oxygen supply and oxygen extraction fraction (OEF) between older adults categorized by vascular risk and white matter lesion burden.
Results: In low-risk individuals, OEF was uniquely lower in the subgroup with higher lesion burden, while oxygen supply did not differ between the subgroups.
Impact: Impaired oxygen extraction may represent an important and independent contributor to white matter lesion burden in older adults in whom lesion burden is high despite the absence of conventional vascular risk factors.
Introduction
White matter lesions (WMLs) are common with aging, and a higher WML burden has been observed in older adults with vascular risk factors, including diabetes and hypertension.1 Oxygen availability is essential for brain tissue health, and hypoxia due to reduced oxygen supply (i.e. hypoperfusion) has been hypothesized to contribute to the formation of age-related WMLs.2 Meanwhile reduced oxygen availability to the brain may also result from a decrease in oxygen extraction fraction (OEF).3 Recent studies have indicated that lower OEF may correlate with increased impairment in clinical conditions4 as well as in the context of WMLs.5 However, OEF has not been as extensively studied in this context. In addition, the presence or absence of vascular risk factors might disturb these processes6 and lead to variability in associations between hemodynamic physiology and WML burden. In this study, we investigated the relationship between vascular risk factors and microvascular physiology (i.e., oxygen supply and oxygen extraction fraction), and their association with WML burden in older adults.Methods
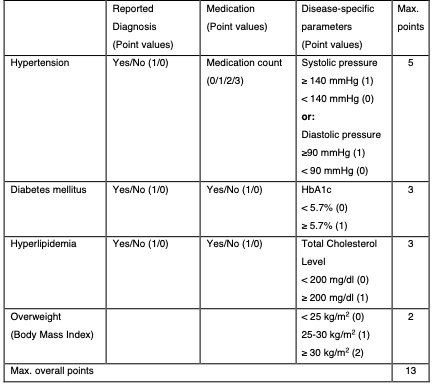
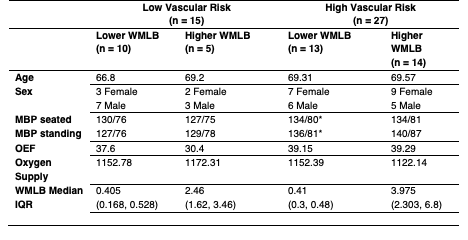
Study participants. A cohort of typically-aging older adults between 60–80 years (n=42) was enrolled in this prospective study. Participants were categorized exhibiting either ‘high’ vascular risk (VRF+; n=27) or ‘low’ vascular risk (VRF−; n=15) based on information regarding medication use, clinical diagnosis, and disease-specific markers of four major modifiable conditions: hypertension, diabetes, hyperlipidemia, and overweight (Figure 1). Participants were further subdivided within the vascular risk groups into ‘high’ or ‘low’ WML burden based on positive or negative residuals, respectively, from a regression of WML burden against age.Data acquisition. MR imaging data was acquired in all participants at 3 Tesla (Prisma; Siemens Healthcare; Erlangen, Germany) using a 32-channel head coil. T1-weighed MRI was acquired using a multi-echo MPRAGE (TR=2500 ms; TI=1000 ms; TE=1.8/3.6/5.4/7.2 ms; spatial resolution=0.8×0.8×0.8 mm3; number of echoes=4). A multi-timepoint pseudocontinuous arterial spin labeling sequence (labeling duration=1500 ms and five post-labeling delays equally spaced between 200-2200 ms) and a multi-band 2D gradient-echo EPI readout (multi-band factor=6; TR=3580 ms; TE=19 ms; spatial resolution=2.5×2.5×2.5 mm3) was acquired.7 T2-relaxation-under-spin-tagging (TRUST) MR data8 were acquired with a post-labeling delay time=1022 ms, four effective echo times (eTEs) = 0, 40, 80, and 160 ms, and a single-slice gradient-echo EPI readout (TR/TE = 1978/3.6 ms; spatial resolution = 3.4 × 3.4 mm2) at approximately 20 mm above the confluence of the sinuses.
Processing and analysis. Cerebral blood blow (CBF) was computed using a two-compartment model and with accounting for arterial transit time as previously described.9 Cerebral oxygen supply was computed as the product of CBF, arterial oxygen saturation (measured with pulse oximetry), and the oxygen transport capacity of blood. Venous oxygenation was derived from TRUST,10 and OEF was computed as the relative ratio between arterial oxygen saturation (from pulse oximetry) and venous saturation. Cerebral oxygen supply and cerebral OEF were compared between risk/lesion burden groups using t-tests with a 0.05 level of significance.
Results
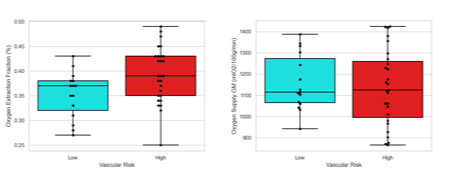
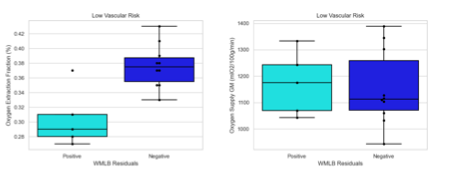
Participant demographics are shown in Figure 2. Participants did not differ in oxygen supply, but OEF was significantly higher in VRF+ (39.22%) versus VRF− (35.2%) individuals (p = 0.02; Figure 1). Within the VRF+ group, no differences were observed in oxygen supply or OEF were found when comparing high versus low lesion burden individuals. Within the VRF− group, no differences in oxygen supply were observed, but OEF was significantly lower in the high lesion burden (30.4%) compared to the low lesion burden (37.6%) subgroup (p = 0.01; Figure 2).Discussion
OEF was significantly higher in VRF+ individuals, indicating a potential compensatory mechanism in the presence of elevated risk for vascular impairment. However, within the VRF− group, the high lesion burden subgroup had a lower OEF than the low lesion burden subgroup, indicating a potentially different physiological mechanism that contributes to WML burden in this group. While it is possible that lower OEF in the high lesion burden group could be related to reduced overall metabolism, analogous differences in OEF were not observed in VRF+ individuals with high and low lesion burden. Therefore, it is not likely that OEF was reduced solely because of lower overall metabolic demand. However, further investigation in larger samples is needed to address the origin of impaired OEF in older adults with healthy vasculature to gain additional insights into the pathophysiological mechanisms of WML pathophysiology.Conclusion
Our findings suggest that lower OEF may represent a marker of impaired physiology associated with WML burden in the absence of conventional vascular risk factors. Such impairment could arise from disturbed capillary transit patterns, and future work will investigate these mechanisms.Acknowledgements
This work was performed with support from the National Institutes of Health (R21AG072068 and K01AG070318), the American Heart Association (19CDA34790002), and the Athinoula A. Martinos Center for Biomedical Imaging.References
1. Breteler MM, van Swieten JC, Bots ML, Grobbee DE, Claus JJ, van den Hout JH, van Harskamp F, Tanghe HL, de Jong PT, van Gijn J. Cerebral white matter lesions, vascular risk factors, and cognitive function in a population-based study: the Rotterdam Study. Neurology. 1994;44:1246-1252. doi: 10.1212/wnl.44.7.1246
2. Martinez Sosa S, Smith KJ. Understanding a role for hypoxia in lesion formation and location in the deep and periventricular white matter in small vessel disease and multiple sclerosis. Clin Sci (Lond). 2017;131:2503-2524. doi: 10.1042/CS20170981
3. Østergaard L, Jespersen SN, Engedahl T, Gutiérrez Jiménez E, Ashkanian M, Hansen MB, Eskildsen S, Mouridsen K. Capillary dysfunction: its detection and causative role in dementias and stroke. Curr Neurol Neurosci Rep. 2015;15:37. doi: 10.1007/s11910-015-0557-x
4. Juttukonda MR, Donahue MJ, Waddle SL, Davis LT, Lee CA, Patel NJ, Pruthi S, Kassim AA, Jordan LC. Reduced oxygen extraction efficiency in sickle cell anemia patients with evidence of cerebral capillary shunting. J Cereb Blood Flow Metab. 2020:271678X20913123. doi: 10.1177/0271678X20913123
5. Juttukonda MR, Stephens KA, Yen YF, Howard CM, Polimeni JR, Rosen BR, Salat DH. Oxygen extraction efficiency and white matter lesion burden in older adults exhibiting radiological evidence of capillary shunting. J Cereb Blood Flow Metab. 2022:271678X221105986. doi: 10.1177/0271678X221105986
6. Dickinson CJ. Cerebral oxidative metabolism in hypertension. Clin Sci (Lond). 1996;91:539-550. doi: 10.1042/cs0910539
7. Harms MP, Somerville LH, Ances BM, Andersson J, Barch DM, Bastiani M, Bookheimer SY, Brown TB, Buckner RL, Burgess GC, et al. Extending the Human Connectome Project across ages: Imaging protocols for the Lifespan Development and Aging projects. Neuroimage. 2018;183:972-984. doi: 10.1016/j.neuroimage.2018.09.060
8. Lu H, Ge Y. Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI. Magn Reson Med. 2008;60:357-363. doi: 10.1002/mrm.21627
9. Juttukonda MR, Li B, Almaktoum R, Stephens KA, Yochim KM, Yacoub E, Buckner RL, Salat DH. Characterizing cerebral hemodynamics across the adult lifespan with arterial spin labeling MRI data from the Human Connectome Project-Aging. Neuroimage. 2021;230:117807. doi: 10.1016/j.neuroimage.2021.117807
10. Lu H, Xu F, Grgac K, Liu P, Qin Q, van Zijl P. Calibration and validation of TRUST MRI for the estimation of cerebral blood oxygenation. Magn Reson Med. 2012;67:42-49. doi: 10.1002/mrm.22970
Figures