3874
Forecasted Brain Structure Alteration Facilitates Cognitive Impairment Prediction: a 7-Year Community Elderly Follow-up Study1College of Computer and Information Sciences, Fujian Agriculture and Forestry University, Fuzhou, China, 2Department of Biomedical Engineering, National University of Singapore, Singapore, Singapore, 3Department of Geriatric Psychiatry, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 4Alzheimer’s Disease and Related Disorders Center, Shanghai Jiao Tong University, Shanghai, China, 5School of Biomedical Engineering, ShanghaiTech University, Shanghai, China
Synopsis
Keywords: Preclinical Image Analysis, Alzheimer's Disease, Asymptomatic Stage; Cognitive Decline; Progression Prediction;
Motivation: Predicting the conversion from cognitive normal to mild cognitive impairment (MCI) at the asymptomatic stage is challenging.
Goal(s): To investigate whether longitudinal alteration in brain structure can provide valuable information for normal-to-MCI conversion prediction.
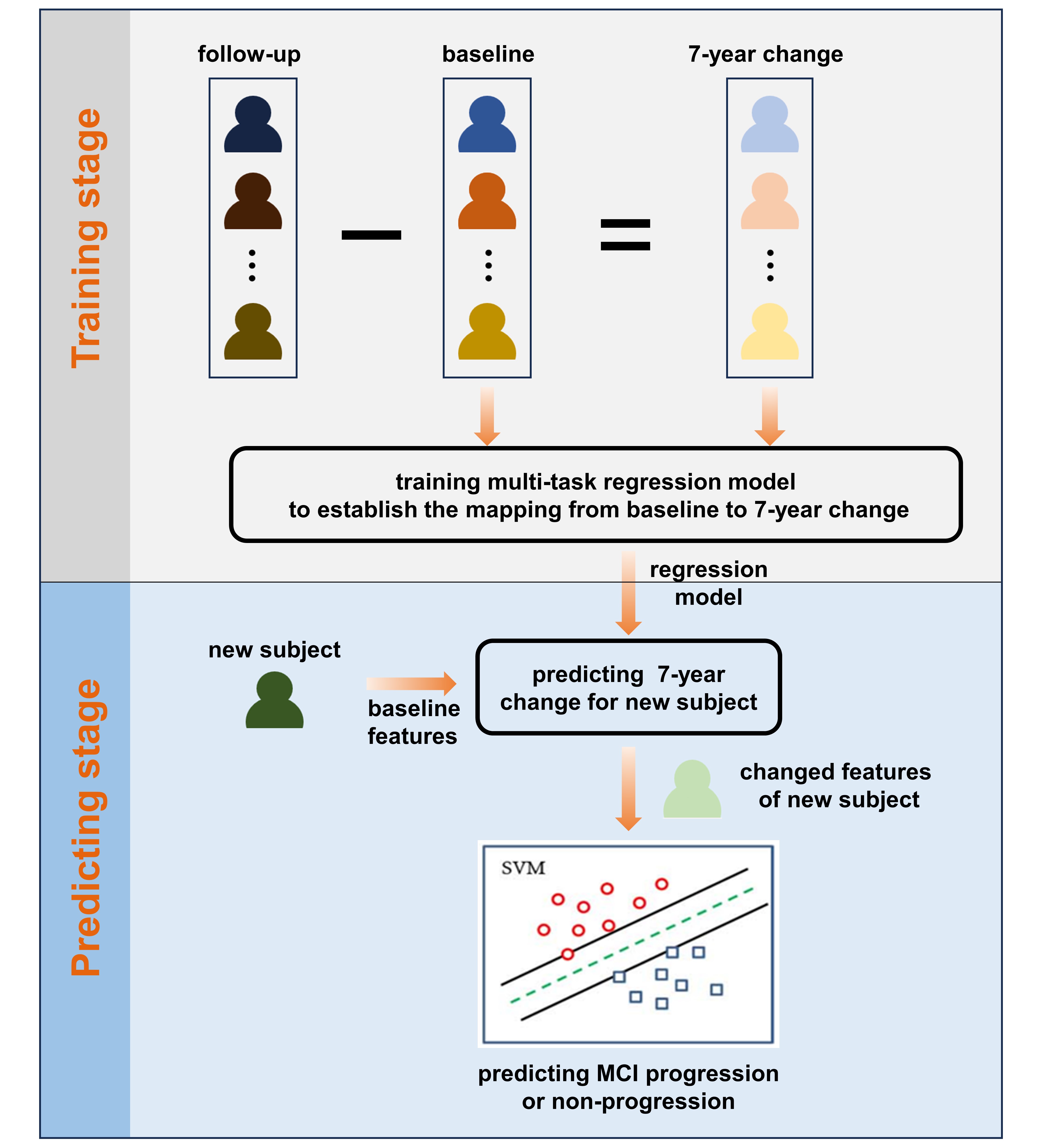
Approach: We conducted a 7-year longitudinal study on 222 community-dwelling elderly and built a two-stage intelligent prediction model to establish the mapping relationship from the baseline to 7-year changes, using brain T1 MRI scans and comprehensive neuropsychological tests.
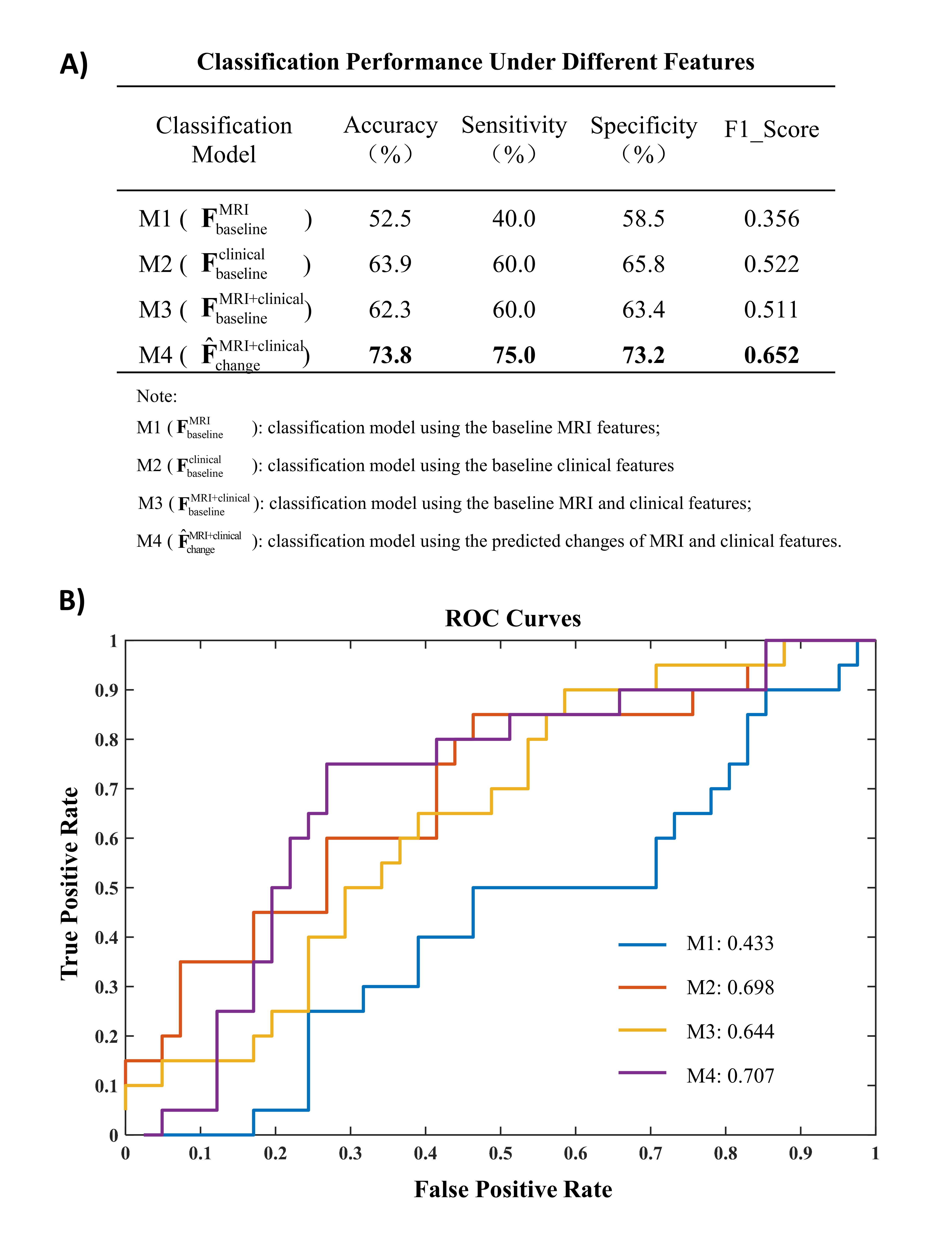
Results: The model, with forecasted 7-year changed features, achieved promising conversion predictions (accuracy=73.8%). Cortical thickness changes, particularly in the visual and default mode cortices, played a significant role in prediction.
Impact: Long-term (7-year) brain cortical changes could be predicted and further used to help disease progression prediction for community elderly. Leveraging pre-built predictive model, physicians can evaluate the progression risk at the preclinical phase, well before the onset of Alzheimer's disease.
Introduction
Recent studies have demonstrated the effectiveness of early intervention in delaying the progression of the disease during the early stages of dementia1. Limited clinical trials have been initiated among cognitively normal (CN) elderly individuals considered at risk of developing mild cognitive impairment (MCI) 2-6. However, predicting the conversion from normal to MCI at a very early stage is extremely challenging because the at-risk population hardly exhibit visible changes in behavior and cognitive function. These changes can be easily confounded by the relatively large individual variability in the course of aging. Therefore, we conducted a 7-year follow-up study on the community's elderly population with normal cognitive function and developed a 7-year prediction model.Methods
- Study Cohort, Clinical Assessment & MRI Acquisition
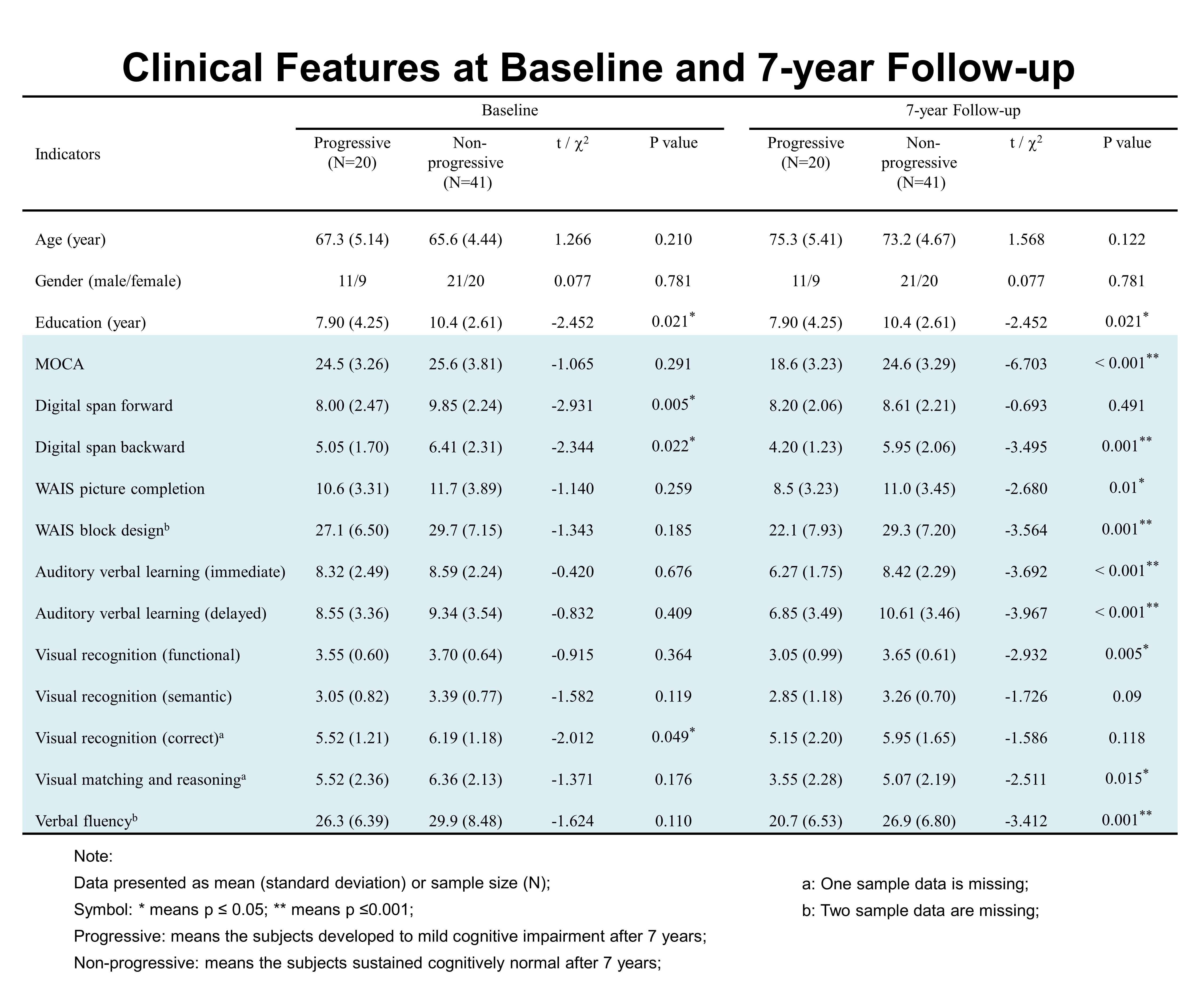
At both the baseline and follow-up visits (Table 1), we administered a comprehensive battery of neuropsychological tests to all participants8. In addition, every subject underwent a T1-weighted MRI scan. We performed structural MRI preprocessing using FreeSurfer 7.1.0 through the 'recon-all' command, which yielded a total of 415 structural MRI features9.
- Two-stage Progression Prediction Model
Results
In Table 1, 20/61 (32.7%) subjects progressed to cognitive impairment. There were no significant differences in most neuropsychology test scores at the baseline stage. However, after 7 years' variation, more indicators show noticeable between-group differences with greater significance.In Figure 2, we constructed contrastive SVM classification models without utilizing predicted changed features (M1~M3). When we used baseline MRI and clinical features separately, the classification performance fell short in effectively distinguishing progressive MCI from normal aging. Even when combining baseline MRI and clinical features, the classification performance did not improve. The optimal results were obtained when we employed both predicted changed MRI and clinical features, achieving an accuracy of 73.8% and an F1 score of 0.652. ROC curves underscored that the predicted change features outperformed others, displaying the highest AUC of 0.707.
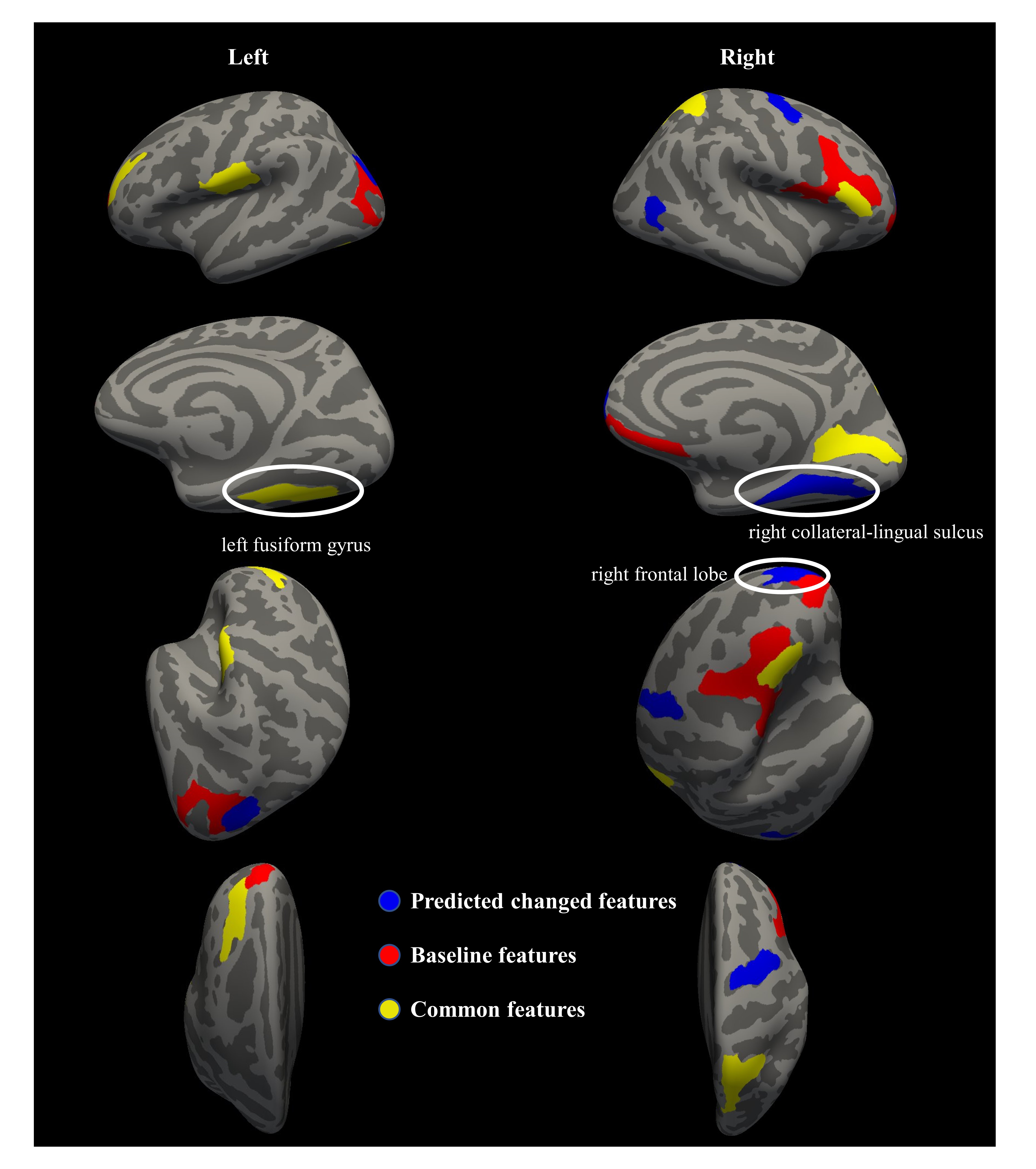
In Figure 3, the most discriminative MRI features were predominantly situated in the middle frontal, superior occipital, superior parietal lobe, and the ventral portion of the temporal and occipital lobes, Comparing to the predicted changed features, the corresponding baseline features had adjacent spatial distributions.
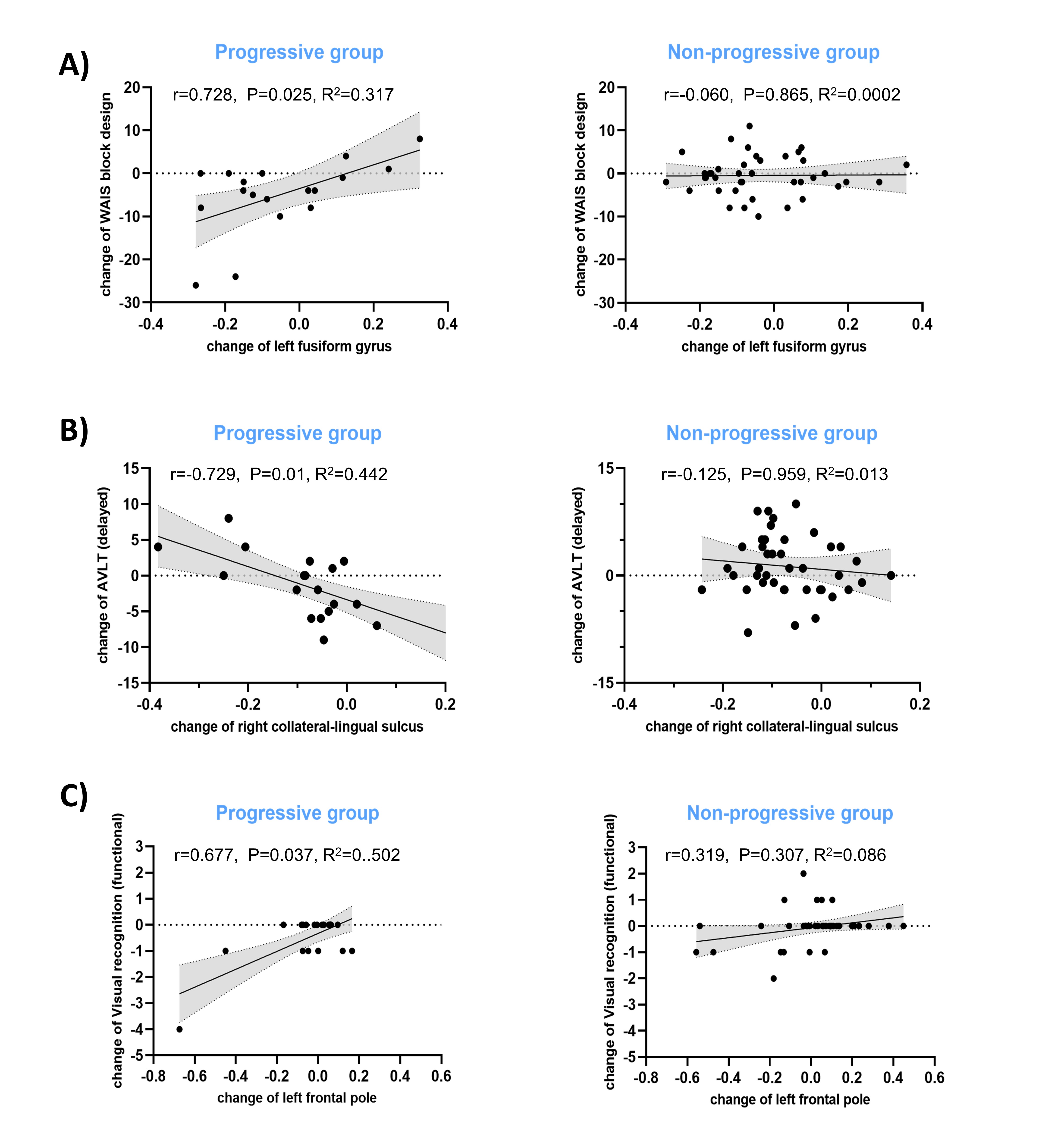
In Figure 4, we found three significant correlations: (A) left fusiform gyrus vs. WAIS block design; (B) right collateral-lingual sulcus vs. AVLT (delayed); (C) right frontal lobe vs. Visual recognition (functional). The progressive group showed significant correlations between the predicted changes in the most discriminative MRI features (i.e. brain structure alteration) and changes in cognitive function, while no such correlations were observed in the non-progressive group.
Discussion
We utilized longitudinal pairwise data to construct a predictive model to investigate the progression from cognitively normal to MCI with a 7-year follow-up. In contrast to other longitudinal studies launched during the asymptomatic stage, our longer follow-up period provides a more comprehensive view of the evolving neurodegenerative pathologies3, 10-13.Following a 7-year timespan, within-subject changes exhibit greater significance compared to cross-sectional features. Longitudinal changed features are better suited to distinguish the MCI progressive group from the stable group14. Our intelligent prediction model excels in this regard, as it not only explores longitudinal feature changes but also mitigates the adverse effects of individual heterogeneity.
Conclusion
With predicted brain alteration features, our two-stage prediction model is intelligent and cost-effective for identifying older adults who are likely to progress to MCI at 7 years post-baseline.Acknowledgements
This research was supported by China Scholarship Council, National Natural Science Foundation of China (Grant No.62301160), Nature Science Foundation of Fujian Province (Grant No.2022J01607).References
1. Sevigny J, Chiao P, Bussière T, et al. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature. 2016;537(7618):50-6.
2. Albert M, Zhu Y, Moghekar A, et al. Predicting progression from normal cognition to mild cognitive impairment for individuals at 5 years. Brain. 2018;141(3):877-87.
3. Parnetti L, Chipi E, Salvadori N, et al. Prevalence and risk of progression of preclinical Alzheimer’s disease stages: a systematic review and meta-analysis. Alzheimer's research & therapy. 2019;11:1-13.
4. Chen Y, Denny KG, Harvey D, et al. Progression from normal cognition to mild cognitive impairment in a diverse clinic-based and community-based elderly cohort. Alzheimer's & Dementia. 2017;13(4):399-405.
5. Jia L, Zhu M, Kong C, et al. Blood neuro‐exosomal synaptic proteins predict Alzheimer's disease at the asymptomatic stage. Alzheimer's & Dementia. 2021;17(1):49-60.
6. Pang Y, Zhou J, Albin RL, et al. Predicting Conversions from Normal to MCI and from MCI to AD with Clinical Variables in the National Alzheimer’s Coordinating Center Uniform Data Set Version 3: Application of Big Data Analytics and Transition Probability Calculators. Alzheimer's & Dementia. 2022;18:e065231.
7. Petersen RC. Mild cognitive impairment. New England Journal of Medicine. 2011;364(23):2227-34.
8. Xiao S, Lewis M, Mellor D, et al. The China longitudinal ageing study: overview of the demographic, psychosocial and cognitive data of the Shanghai sample. Journal of Mental Health. 2016; 25(2):131-136.
9. Destrieux C, Fischl B, Dale A, et al. Automatic parcellation of human cortical gyri and sulci using standard anatomical nomenclature. Neuroimage. 2010;53(1):1-15.
10. Ebenau JL, Timmers T, Wesselman LM, et al. ATN classification and clinical progression in subjective cognitive decline: The SCIENCe project. Neurology. 2020;95(1):e46-e58.
11. Snitz BE, Wang T, Cloonan YK, et al. Risk of progression from subjective cognitive decline to mild cognitive impairment: The role of study setting. Alzheimer's & Dementia. 2018;14(6):734-42.
12. Van der Kall LM, Truong T, Burnham SC, et al. Association of β-amyloid level, clinical progression, and longitudinal cognitive change in normal older individuals. Neurology. 2021;96(5):e662-e70.
13. Johnson DK, Storandt M, Morris JC, et al. Longitudinal study of the transition from healthy aging to Alzheimer disease. Archives of neurology. 2009;66(10):1254-9.
14. Huiskamp M, Eijlers AJ, Broeders TA, et al. Longitudinal network changes and conversion to cognitive impairment in multiple sclerosis. Neurology. 2021;97(8):e794-e802.
Figures