3863
Prediction of ATRX Gene Status in IDH-mutant grade 2/3 Gliomas by ADC and APT Histogram Analysis1Department of Radiology, Zhujiang Hospital of Southern Medical University, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, Glioma; Amide proton transfer imaging; apparent diffusion coefficient; Gene
Motivation: To the best of our knowledge, no study has explored the predictive ability of APT for ATRX mutations in gliomas.
Goal(s): Investigating APT and ADC's predictive capacities for ATRX mutations in WHO grade 2/3 gliomas with IDH mutations, we conducted a retrospective analysis.
Approach: We retrospectively analyzed data from these patients and extracted features for modeling.
Results: The results revealed the APT-median became the key diagnostic parameter, and the model developed showed the highest diagnostic efficiency. The histogram analysis method based on APT and ADC is an effective non-invasive tool for predicting ATRX gene status.
Impact: Our study, to our knowledge, pioneered the use of APT in predicting ATRX mutations in gliomas and established histogram analysis of APT and ADC as an effective non-invasive tool for ATRX gene prediction in IDH mutant WHO grade 2/3 gliomas.
Objective
In line with the 2021 WHO Classification of Central Nervous System Tumors, ATRX gene mutations hold significance in IDH-mutant gliomas, particularly in lower-grade gliomas (WHO2/3 grade).1,2,3,4This study aims to assess the utility of noninvasive imaging techniques (CEST/APT-MRI and ADC) for predicting ATRX gene status in IDH-mutant lower-grade gliomas, with the goal of enhancing prognostic accuracy and providing personalized treatment insights.Materials and methods
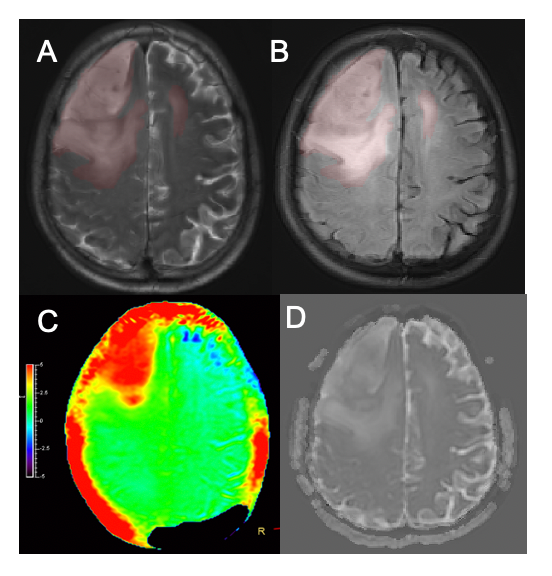
We retrospectively analyzed clinical and imaging data from 69 patients with surgically confirmed IDH-mutated low-grade gliomas (WHO 2/3) at Zhujiang Hospital of Southern Medical University between June 2017 and June 2023. Among these, 20 were ATRX-mutant (ATRX-), and 49 were ATRX-wild (ATRX+).APTw, ADC, and conventional clinical MR images were combined to manually segment regions of interest (ROI), encompassing both the tumor and its surrounding edema (Figure 1). Histogram features were extracted. Various statistical methods were employed to compare clinical and quantitative imaging data between the two groups. Additionally, a binary logistic model was constructed to assess the diagnostic performance of different parameters and the multiparametric model.Results
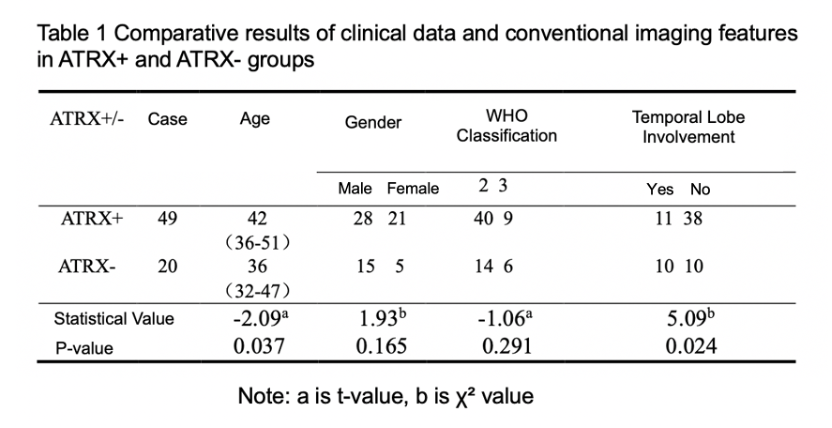
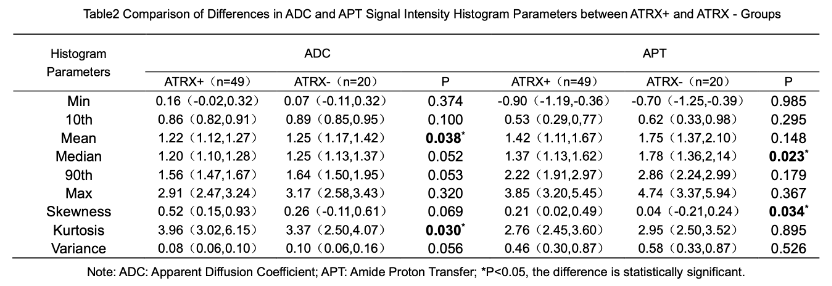
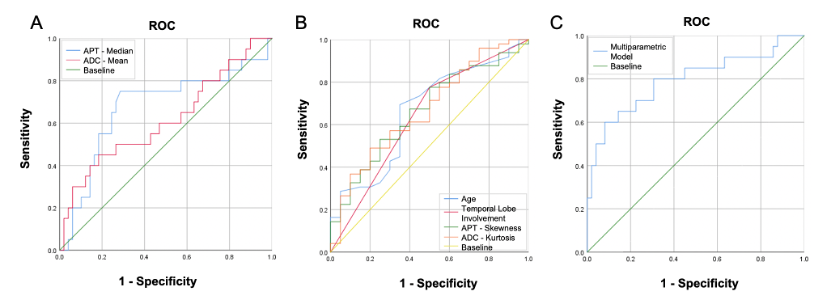
When comparing clinical and conventional imaging features, no statistical differences were observed in terms of gender and WHO grading between the two groups. However, significant differences emerged in age and temporal lobe involvement (Table 1). As for the comparison of ADC and APT histogram parameters, we identified notable distinctions in APT-Median, ADC-Mean, APT-Skewness, and ADC-Kurtosis. APT-Median and ADC-Mean were lower in the ATRX+ group, while APT-Skewness and ADC-Kurtosis were higher (Table 2).Further ROC analysis of these statistically distinct features revealed that APT-Median had the highest AUC (0.675) and demonstrated strong predictive capabilities for ATRX gene mutations, with a sensitivity of 75.0% and a specificity of 71.4%.When using the six statistically distinct features mentioned above as independent variables and ATRX gene status as the dependent variable to construct a binary logistic model, the AUC of this ATRX gene status prediction model reached 0.795, with a specificity of 99.20% (Figure 2).Discussion
In this study, we observed a higher prevalence of ATRX gene mutations in IDH-mutant WHO 2/3 grade gliomas among younger patients, which aligns with findings from previous research by other scholars.5 The identification of ATRX mutant tumors being more likely to involve the temporal lobe raised questions, and we hypothesized that variations in glioma inclusion criteria and the proportion of ATRX mutations may contribute to the disparities with Zhang et al’s 6 findings.Histogram analysis, as opposed to traditional statistics methods, offers richer information and excels in characterizing tumor heterogeneity. It has found extensive application in glioma molecular typing, treatment response assessment, and survival prediction.7,8 Our study revealed that while some ADC parameters exhibited statistical differences, their diagnostic efficacy remained moderate, suggesting a potential overlap in phenotypes between ATRX-mutated and unmutated lower-grade gliomas on the ADC map. Additionally, the smaller ADC-Kurtosis in the ATRX- group may indicate a more concentrated distribution of ADC values in ATRX-mutant gliomas, implying lower tumor heterogeneity.
APT signal is intricately correlated with tumor cell density, invasiveness, and prognosis.9 Recent research has demonstrated that the addition of ATRX mutations to the backdrop of IDH1/p53 mutations amplifies the invasiveness of astrocytoma cells.10 Furthermore, the frequent co-occurrence of P53 gene mutations with ATRX mutations can induce uncontrolled cell proliferation and cancerous transformation.10 Consequently, we posit that ATRX-mutated glioma cells, characterized by heightened invasiveness and increased number, account for their elevated APT-Median values.
Conclusion
APT- and ADC-based histogram analyses offer valuable predictive insights into ATRX gene status in IDH-mutant WHO grade 2/3 gliomas, introducing a novel noninvasive predictive tool for clinical applications.Acknowledgements
No acknowledgment found.References
[1]. Louis, D.N., et al., The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol, 2021. 23(8): p. 1231-1251.
[2]. Louis, D.N., et al., The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol, 2016. 131(6): p. 803-20.
[3]. Wiestler, B., et al., ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol, 2013. 126(3): p. 443-51.
[4]. Han, B., et al., Loss of ATRX suppresses ATM dependent DNA damage repair by modulating H3K9me3 to enhance temozolomide sensitivity in glioma. Cancer Lett, 2018. 419: p. 280-290.
[5]. Haase, S., et al., Mutant ATRX: uncovering a new therapeutic target for glioma. Expert Opin Ther Targets, 2018. 22(7): p. 599-613.
[6]. Zhang, L., et al., Multicenter clinical radiomics-integrated model based on [(18)F]FDG PET and multi-modal MRI predict ATRX mutation status in IDH-mutant lower-grade gliomas. Eur Radiol, 2023. 33(2): p. 872-883.
[7]. Qi, X.X., et al., Histogram analysis of diffusion kurtosis imaging derived maps may distinguish between low and high grade gliomas before surgery. Eur Radiol, 2018. 28(4): p. 1748-1755.
[8]. Hempel, J.M., et al., Diffusion kurtosis imaging histogram parameter metrics predicting survival in integrated molecular subtypes of diffuse glioma: An observational cohort study. Eur J Radiol, 2019.
[9]. Su, C., et al., Amide Proton Transfer Imaging Allows Detection of Glioma Grades and Tumor Proliferation: Comparison with Ki-67 Expression and Proton MR Spectroscopy Imaging. AJNR Am J Neuroradiol, 2017. 38(9): p. 1702-1709.
[10]. Hu, C., et al., ATRX loss promotes immunosuppressive mechanisms in IDH1 mutant glioma. Neuro Oncol, 2022. 24(6): p. 888-900.
Figures