3861
Mapping cellular proliferation activity of glioma by water exchange DCE-MRI at high spatial resolution1Key Laboratory of Biomedical Engineering of Ministry of Education, College of Biomedical Engineering and Instrument Science, Zhejiang University, Hangzhou, China, Hangzhou, China, 2MR Research Collaboration Team, Siemens Healthineers Ltd, Shanghai, China, 3Department of Radiology, Qilu Hospital of Shandong University, jinan, China, 4Department of Neurosurgery, Provincial Hospital Affiliated to Shandong First Medical University, jinan, China
Synopsis
Keywords: Tumors (Pre-Treatment), MR-Guided Interventions, Glioma, Ki67, transmembrane water-efflux rate, Aquaporins4.
Motivation: Cell proliferation abnormalities (e.g., Ki67 status) are key features of glioma. Conventional biopsy is used to characterize Ki67 expression levels in vivo, but it lacks spatial and temporal information because of intratumorally heterogeneity.
Goal(s): To identify MRI parameters representing the intracellular water-efflux rate regulated by aquaporin-4, a noninvasive biomarker sensitive to Ki67 quantitative expression, in glioma.
Approach: Human tumors, animal models, and cell lines were investigated by water-exchange DCE-MRI and immunohistochemistry.
Results: Ki67 and transmembrane water-efflux rate showed a strong linear relationship. The underlying mechanism was the close symbiotic expression pattern between aquaporin-4 and Ki67.
Impact: Transmembrane water-efflux rate is a sensitive biomarker of Ki67 because rapidly growing cells upregulate aquaporin-4 expression for enhanced transmembrane transport.
Introduction
Cell proliferation status is an important histology biomarker for glioma grading and prognosis1. Conventional biopsy is generally used to characterize Ki67 (proliferation marker) expression, but this approach may lead to underestimation of Ki67 and incorrect diagnosis2. We explored whether glioma proliferation activity could accelerate transmembrane water exchange, a physiological process that can be accurately measured via water-exchange DCE-MRI3. We also explored the underlying mechanism involving aquaporin-4 (AQP4) channels, which constitute the dominant transmembrane water transport pathway in the central nervous system.Methods
Glioma patients were recruited according to inclusion criteria of the Institutional Review Board (IRB) of Shandong Provincial Hospital, Shandong First Medical University. Water-exchange DCE-MRI (Fig 1) were performed and analyzed as previously described3,4 1~2 days before stereotactic biopsy. The resulting intracellular water efflux rate constant (kio) map was registered to structural MRI for stereotactic biopsy planning. For each patient, multiple biopsy samples were selected with varying kio values. “Point-to-point” AQP4 expression levels were obtained by immunohistochemistry (IHC) (Fig. 2A). Subcutaneous and orthotopic glioma models was established by injecting C6 glioma cells in the leg or brain of Sprague Dawley rats. The rats were then subjected to water-exchange DCE-MRI on a 7T MRI research system (Siemens Healthcare, Erlangen, Germany); immediately thereafter, tissue was collected and fixed with 4% paraformaldehyde for IHC staining of AQP4. For pharmacological inhibition of AQP4, each animal was intravenously injected with TGN020 (3 mg/kg).Results and Discussion
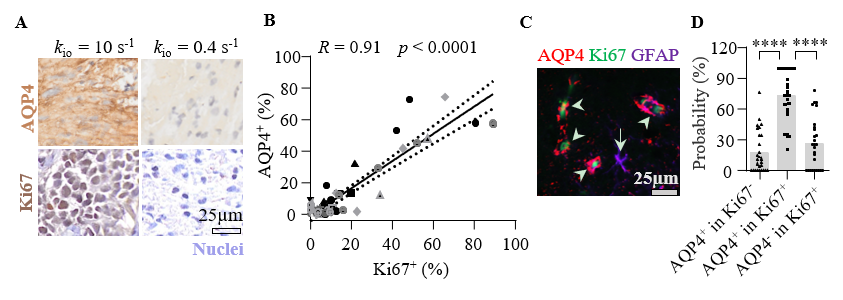
Water-exchange DCE-MRI revealed intratumoral heterogeneity of kio in human glioma (Fig 2). MRI-guided stereotactic biopsy enabled direct comparison of kio with biopsy histology results in a “point-to-point” manner. On visual inspection, the sample with kio = 10.0s-1 shows much higher Ki67 expression than samples with kio =0.11 s-1. A significant linear correlation (R2=0.82, p<0.0001) was identified between kio and Ki67+ (kio=12.2s-1 × Ki67+ % + 0.2s-1) using 69 biopsies from 36 glioma patients (Fig 2E).IHC showed that higher kio samples exhibited faster proliferation and stronger AQP4 expression (Fig 3A). Pearson correlation analysis demonstrated a positive relationship between Ki67 and AQP4 quantitative expression (Fig 3B), consistent with prior studies5,6.We investigated Ki67 and AQP4 synchronous expression in proliferating glioma cells using the total fluorescent signal intensities of Ki67 and AQP4 (Fig 3C), and the AQP4+&AQP4- ratio in Ki67+/Ki67- cells. In Ki67+ glioma cells, AQP4+ percent was significantly more than AQP4- percent (73.6 ± 4.8% Vs 26.4 ± 4.8%, p<0.0001). In AQP4+ glioma cells, Ki67+ percent was significantly more than Ki67- percent (73.6 ± 4.8% Vs 18.1 ± 4.0%, p<0.0001) (Fig 3D). These results showed that proliferating cells (Ki67+) was colocalized with AQP4+. The close correlation of kio and Ki67 is presumably related to the dynamic co-expression of AQP4 and Ki67.
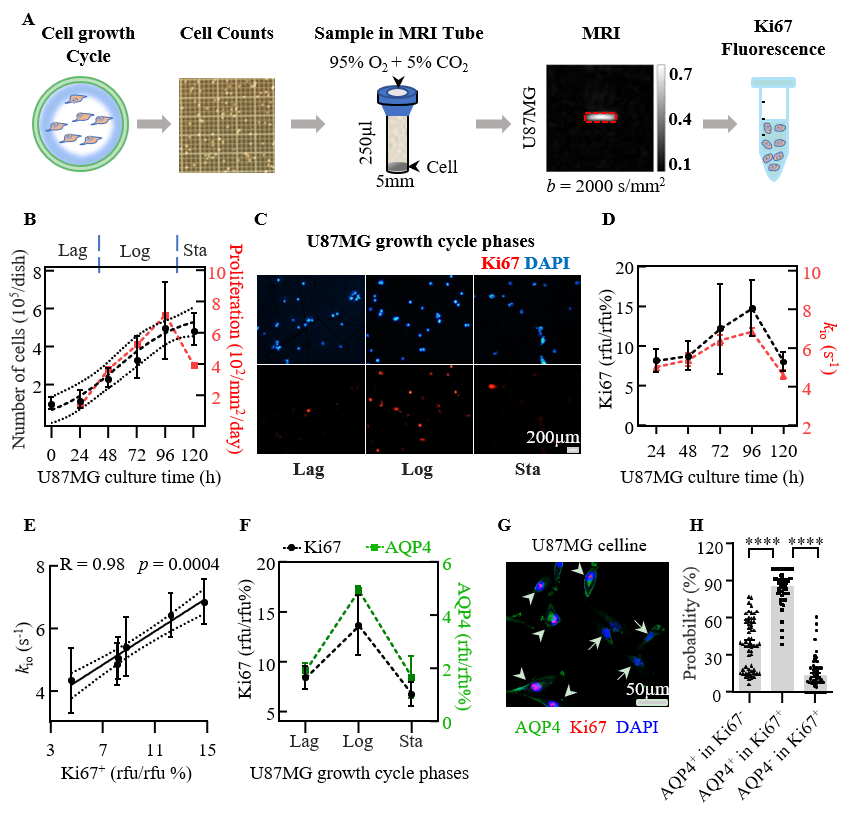
As in a previous study3, we loaded U87MG cells in a custom-built MR tube with phosphate buffered saline + Gd+, then centrifuged them to obtain cell pellets that would provide an accurate estimate of kio. We found that U87MG growth rate (Fig 4B) and Ki67 expression level (Fig 4C) were consistent with cell proliferation status [Lag-phase (Lag), adapt the new dish environment and slow growth, Log-phase (Log) of exponential growth, and Sta-phase (Sta), stationary-phase of growth drops nearly to zero]. kio and Ki67 expression level showed similar trends regarding cell growth (Fig 4D). Additionally, we observed a significant linear correlation between Ki67 and kio (Fig 4E), along with synchronous changes involving Ki67 and AQP4 (Fig 4F-H).
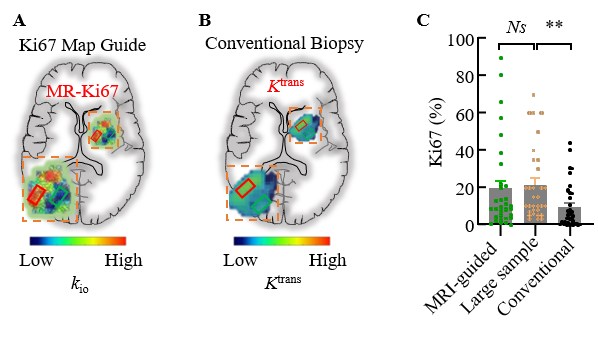
Disagreements in Ki67 expression assessment, based on biopsy and subsequent surgical samples, complicate glioma treatment decisions. We performed pairwise comparisons of biopsy tissues with MR-Ki67 mapping guidance (MRI-guided) (Fig 5A), conventional biopsy based on Ktrans map (or the contrast enhanced map) (Fig 5B), and Large sample (bulk sample from surgery) Ki67 IHC results. We discovered that the conventional biopsy Ki67 expression was significantly less than Large sample (p = 0.0019), and no significant difference between Large sample and MRI-guided group (p =0.6856) (Fig 5C). These results confirmed MR-Ki67 mapping could represent true glioma proliferation status better than the selection based on conventional MRI.
Conclusion
We showed that kio is a sensitive and reproducible biomarker of the Ki67 expression in glioma. Higher Ki67 expression was correlated with greater AQP4 expression, leading to increased kio. Cellular AQP4 water-exchange functions influence key pathways in glioma tumor proliferation supporting the use of MR-Ki67 mapping as a biomarker to guide biopsy, dynamic monitoring of treatment sensitivity, and therapy options of gliomas.Acknowledgements
References
1. Komori T. Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System. Lab. Investig., 2022, 102(2): 126–133.
2. Melguizo-Gavilanes I, Bruner J M, Guha-Thakurta N, et al. Characterization of pseudoprogression in patients with glioblastoma: is histology the gold standard? J. Neurooncol., 2015, 123(1): 141–150.
3. Jia Y, Xu S, Han G, et al. Transmembrane water-efflux rate measured by magnetic resonance imaging as a biomarker of the expression of aquaporin-4 in gliomas. Nat. Biomed. Eng., England: 2022, 7(3): 236–252.
4. Bai R, Springer C S, Plenz D, et al. Fast, Na+/K+ pump driven, steady-state transcytolemmal water exchange in neuronal tissue: A study of rat brain cortical cultures. Magn. Reson. Med., 2018, 79(6): 3207–3217.
5. Du L, Xing Z, Tao B, et al. Both IDO1 and TDO contribute to the malignancy of gliomas via the Kyn–AhR–AQP4 signaling pathway. Signal Transduct. Target. Ther., Springer US, 2020, 5(1): 1–13.
6. Lan Y L, Chen C, Wang X, et al. Gamabufotalin induces a negative feedback loop connecting ATP1A3 expression and the AQP4 pathway to promote temozolomide sensitivity in glioblastoma cells by targeting the amino acid Thr794. Cell Prolif., 2020, 53(1): 1–21.
Figures
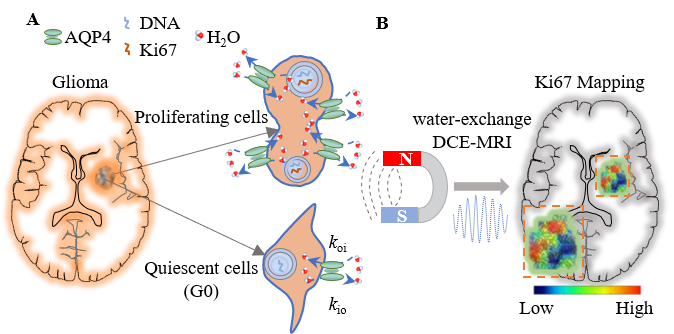
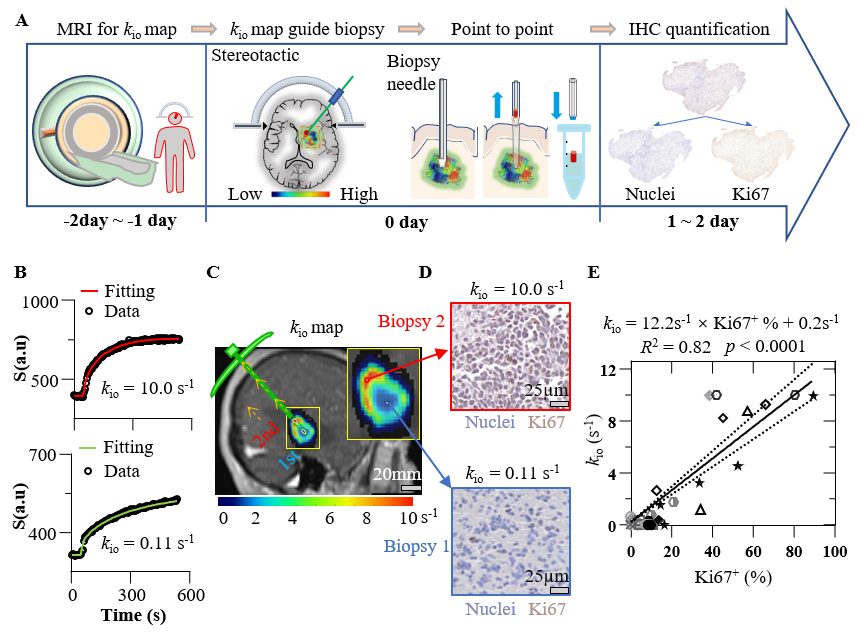
Fig 2. kio shows a close linear correlation with Ki67 expression in human glioma. A: Experimental workflow. B: Fitted models of water-exchange DCE-MRI. C: kio map to guide biopsy acquisition with single needle. D: Higher (lower) Ki67 expression was observed in tissue with larger (smaller) kio. E: Linear correlation present between kio and Ki67+.