3858
Improved Detection of Target Metabolites in Brain Tumors with Intermediate TE High SNR and High Bandwidth Spin Echo Sequence at 5.0T1Zhongnan Hospital of Wuhan University, Wuhan, China, 2United Imaging Healthcare, Shanghai, China
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, MRS
Motivation: challenges emerge at ultra-high fields when measuring metabolites using 1H-MRS.
Goal(s): To investigate how well the high SNR and high bandwidth spin echo (HISE) technique performs at 5.0T for detecting target metabolites in brain tumors.
Approach: 26 Subjects suspected of having brain tumors were enrolled. HISE and point-resolved spectroscopy (PRESS) single-voxel spectroscopy (SVS) scans were collected with a 5.0T clinical scanner with an intermediate echo time (TE=144ms).
Results: HISE outperformed the clinical standard PRESS technique in detecting target metabolites of brain tumors at 5.0T, particularly Lac and Ala.
Impact: In a recently developed whole-body 5.0T clinical scanner, the HISE technique has been demonstrated to be more preferable than PRESS for the clinical diagnosis of brain tumors.
Introduction
Brain tumors encompass more than 120 different types, with some common primary tumors being highly malignant.1The gold standard for clinical diagnosis of brain tumors involves pathological testing conducted after invasive surgical resection or needle biopsy.2 Still, the development of non-invasive diagnostic tools is necessary.Recently, a 5.0T clinical scanner has also shown its capabilities in neuroimaging.As far, the performance of 1H-MRS in diagnosing brain tumors has never been investigated at 5.0T.the high SNR and high bandwidth spin echo (HISE) technique, also named semi-LASER by some MRI manufacturers, has been recently applied.3Since 5.0T belongs to the ultra-high field, we hypothesize that the HISE will show significant advantages over STEAM and PRESS at 5.0T. The objective of this study is to validate the application of the HISE technique at 5.0T in the clinic and compare its performance in detecting target metabolites of brain tumors to that of the clinical standard PRESS technique.Method
26 Subjects suspected of having brain tumors were enrolled. HISE and point-resolved spectroscopy (PRESS) single-voxel spectroscopy (SVS) scans were collected with a 5.0T clinical scanner with an intermediate echo time (TE=144ms). Main metabolites, including total N-acetyl-aspartate (tNAA), creatine (Cr) and total choline (tCho), were accessed and compared between HISE and PRESS using a paired Student's t-test, with the full width at half maximum (FWHM) and signal-to-noise ratio (SNR) as covariates. The detection rate of specific metabolites, including lactate (Lac), alanine (Ala) and lipid (Lip), and subjective spectral quality were accessed and compared between HISE and PRESS. by two radiologists with 5 and 10 years of experience, using a 5-point Likert scale. The Likert scale was used with the following grading: 1 = not diagnostic; 2 = spectra is markedly distorted with poor diagnostic value; 3 = spectral is minimally distorted with reduced diagnostic value; 4 = no distorted with good diagnostic value; and 5 = spectra with excellent diagnostic quality by presenting more peaks of metabolites. Two radiologists reached a consensus over the scores.The diagnosis was made by a pathologist with 10 years of experience following the guidelines outlined in the 2016 World Health Organization Classification of Tumors of the Central Nervous System. All statistical analyses were performed using SPSS v24.0 software (Chicago, IL).Result
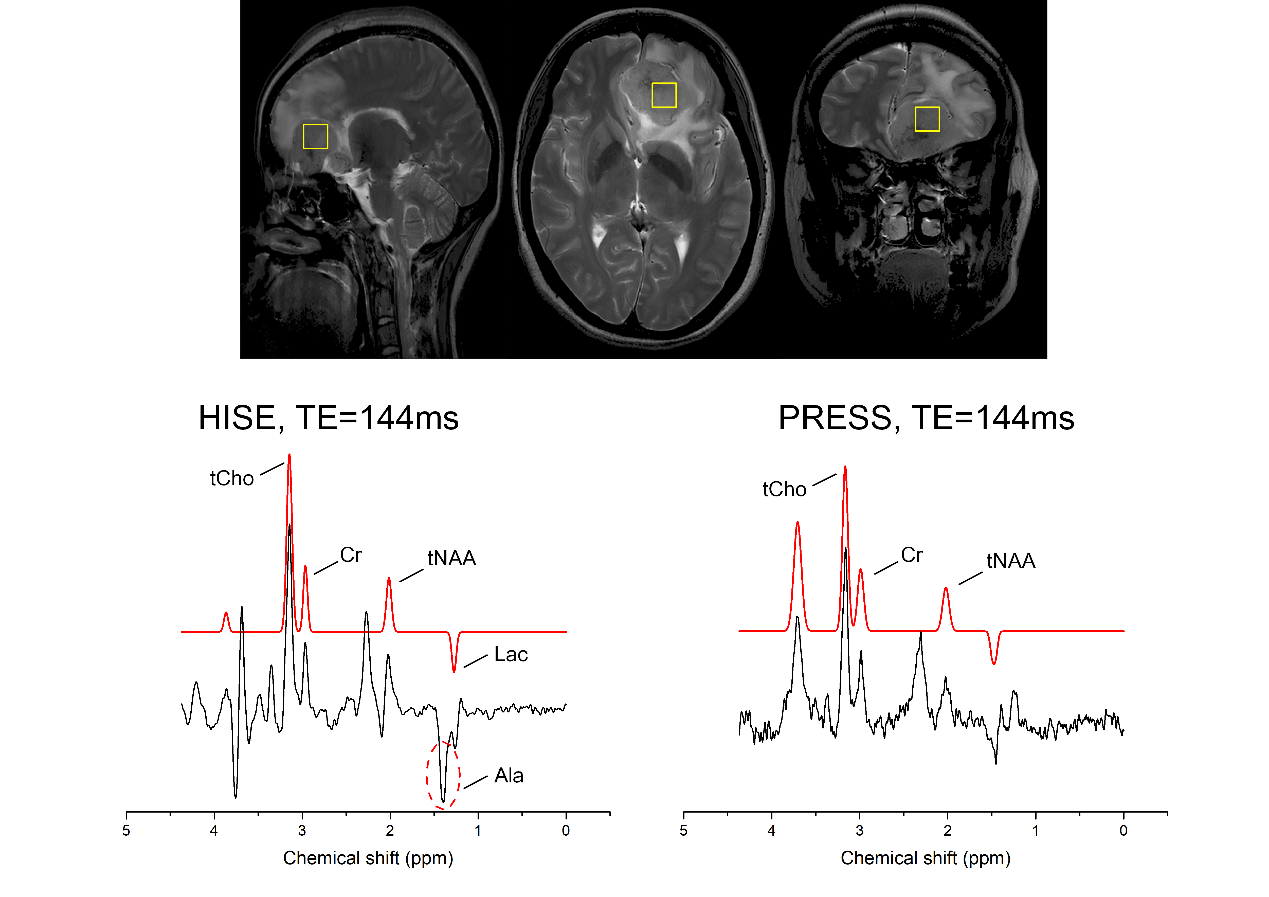
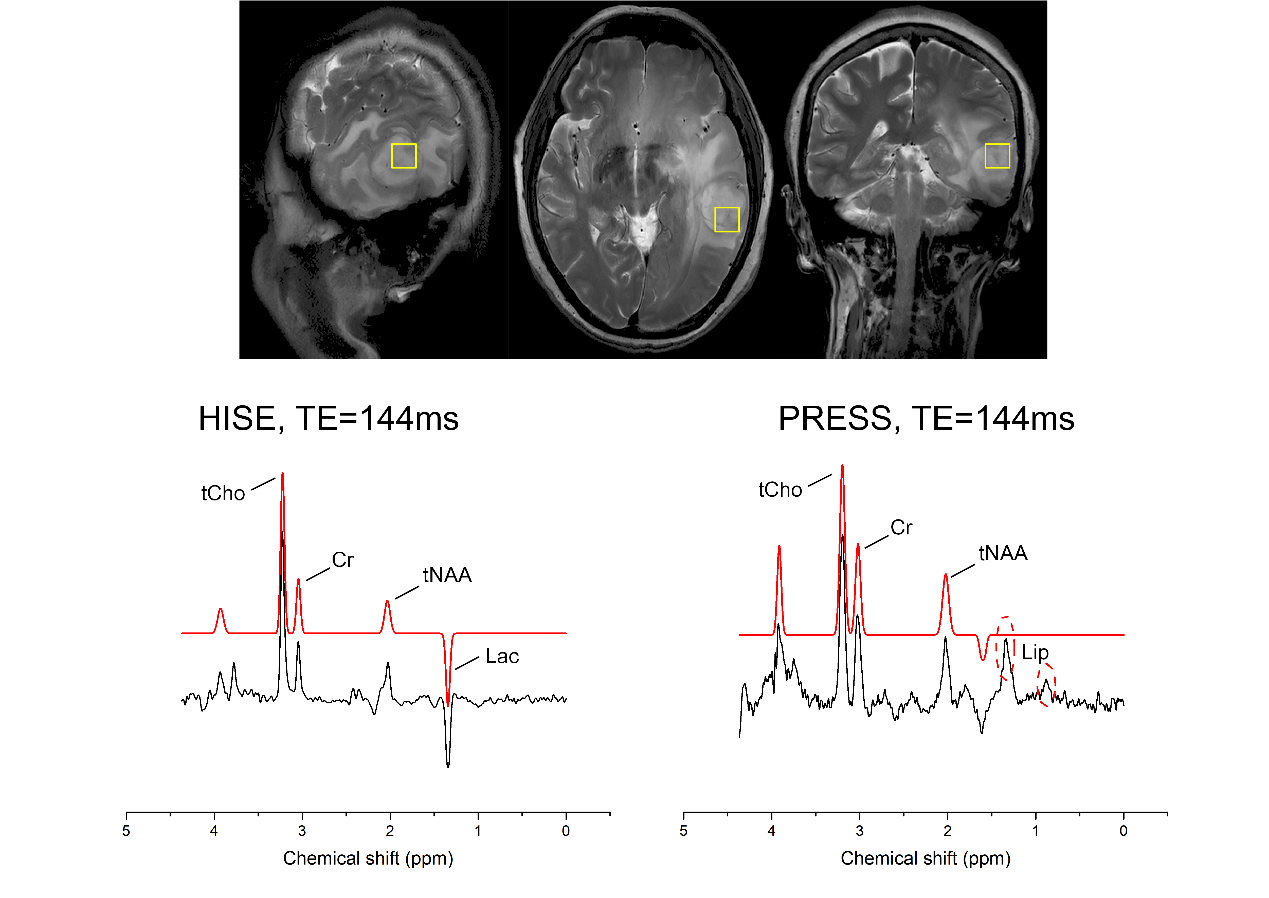
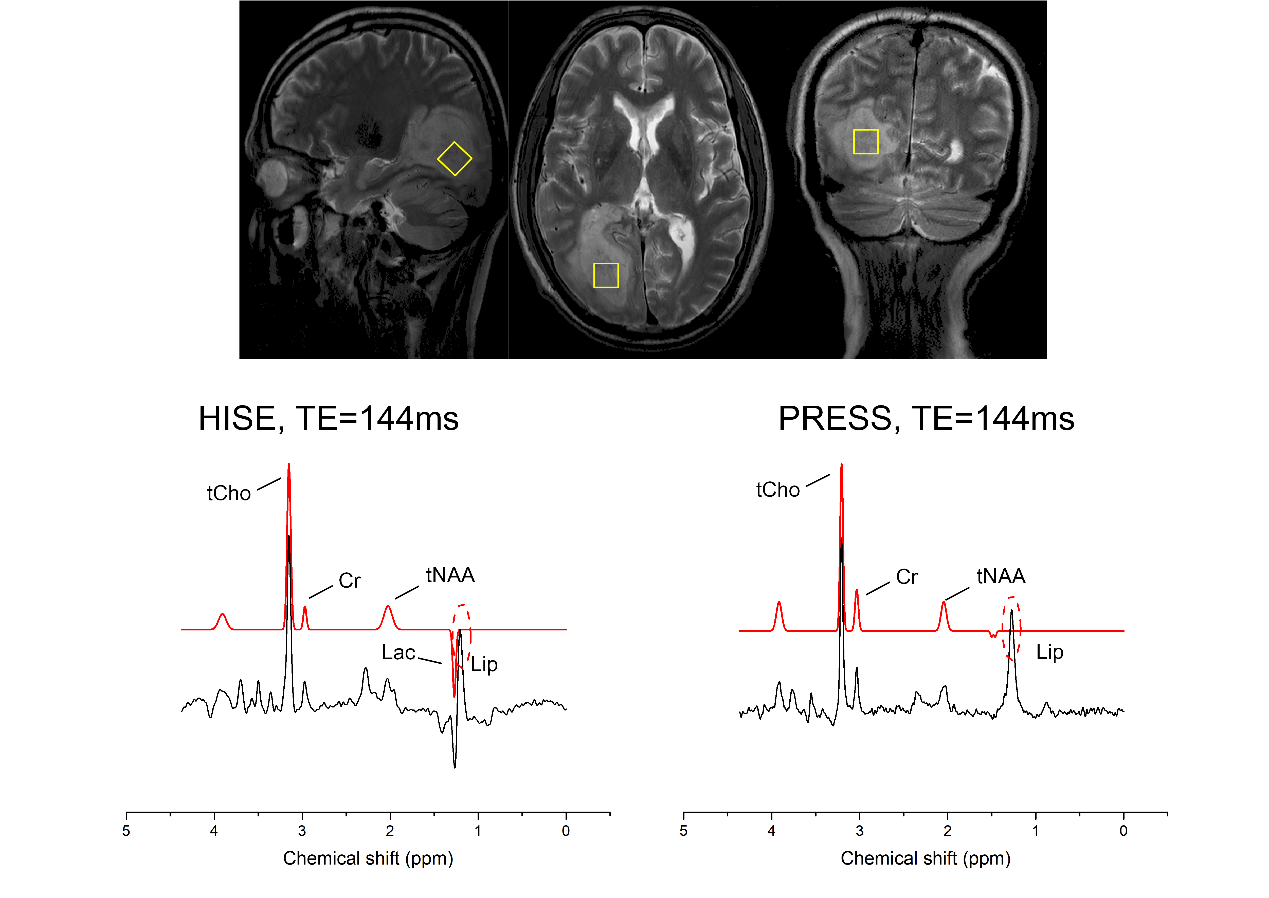
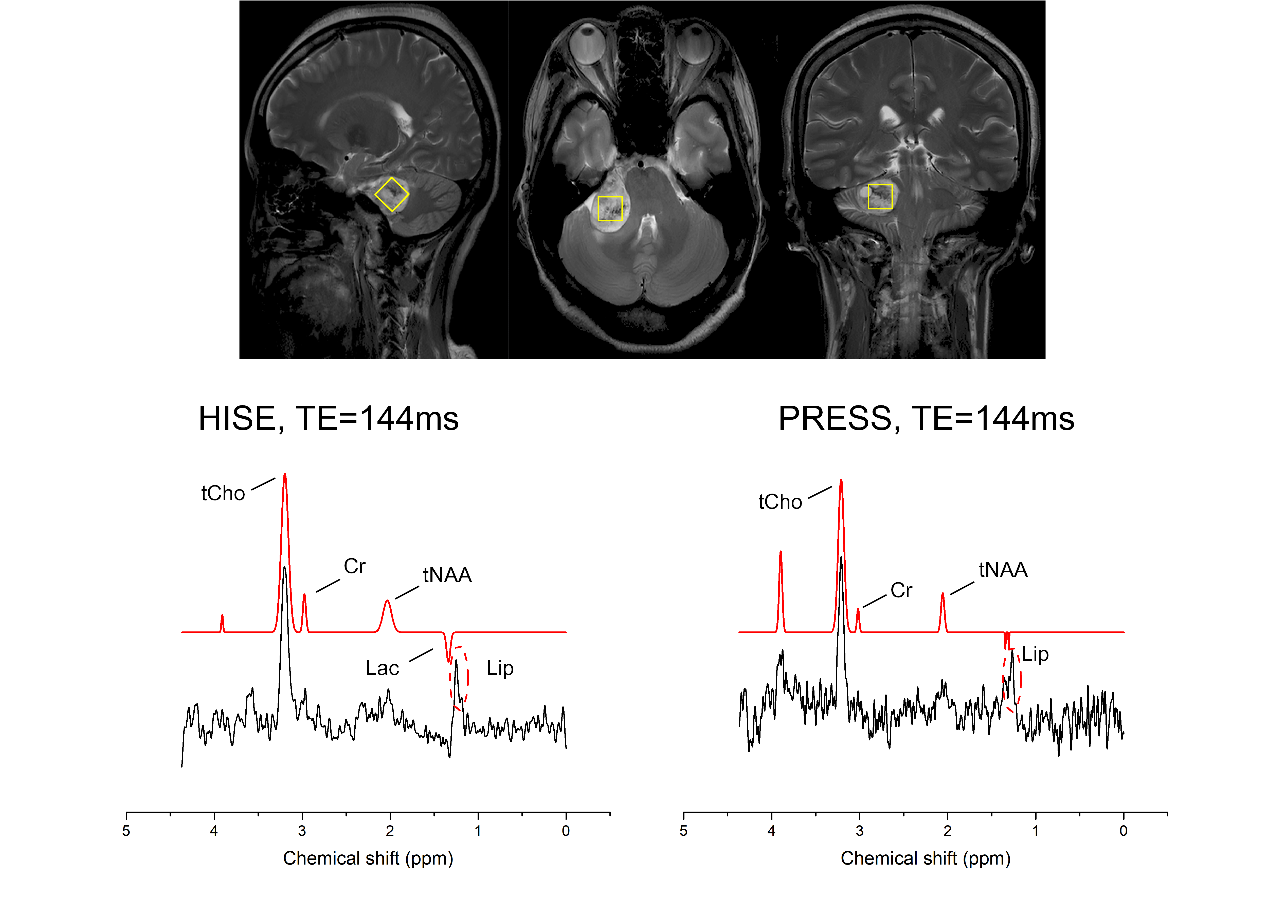
A total of 23 patients (mean age: 55.39 11.17 years, male: n=8) were finally included in this study, consisting of acoustic neuroma (n=2), non-Hodgkin's lymphoma (n=1), meningiomas (n=9), gliomas (n=9), and metastasis (n=2). Representative spectra for typical patients (meningioma, glioma, metastases and acoustic neuroma) were demonstrated from Figure 1 to Figure 4, respectively. Only the FWHM for tNAA was significantly lower with HISE than PRESS (P<0.05). HISE showed significantly higher SNR for tNAA, Cr, and tCho compared to PRESS (P<0.05). Lac was detected in 21 of the 23 cases using HISE, but only in 4 cases using PRESS. HISE detected Ala in 8 out of 9 meningiomas, whereas PRESS detected Ala in just 3 meningiomas. PRESS found Lip in more cases than HISE, which could be owing to PRESS's difficulty in completely suppressing scalp lipid signals. Besides,HISE outperformed PRESS in terms of subjective spectral quality.Discussion and Conclusion
Previous findings at 7.0T support the experts’ consensus that ultra-high fields generally favor HISE over PRESS, however, these results have never been repeated at 5.0T and there is little evidence for the routine use of HISE for brain tumors at 5.0T, hence a comparison study of HISE and PRESS at 5.0T is still essential. In a recently developed whole-body 5.0T clinical scanner, the HISE technique has been demonstrated to be more preferable than PRESS for the clinical diagnosis of brain tumors. It might be due to the following reasons: When the magnetic field strength increases, a larger RF field is needed to flip the spin. Due to the limitation of the RF field amplitude of the system, and in order to minimize CSDE, the return flip angle of PRESS sequence is usually less than 180 degrees. However, by using adiabatic refocusing pulse in HISE sequence, the return flip angle can reach 180 degrees under the same condition, resulting in a lower sensitivity to field inhomogeneities and a higher SNR. HISE increased the band-width of the RF pulses, thus reduced the signal cancellation in Lac.3The high detection rate of Ala in meningiomas could be attributed to the enhanced spectral resolution and little CSDE of HISE at 5.0T, as shown in Figure 1. Lastly, PRESS showed more cases with lipid signals. This could be the unsuppressing scalp lipid signals, as demonstrated in Figure 2. In all, HISE showed advantages over PRESS at 5.0T.Acknowledgements
The authors do not have any possible conflicts of interest.References
Reference:
1. Mack SC, Hubert CG, Miller TE,et al. Nat Neurosci. 2016 Jan;19(1):10-9.
2. Di Bonaventura R, Montano N, Giordano M, et al. J Pers Med. 2021 Sep 12;11(9):909.
3.Fernandes CC, Lanz B, Chen C, Morris PG. NMR Biomed. 2020 Apr;33(4):e4223.
4. Wilson M, Andronesi O, Barker PB, et al. Magn Reson Med. 2019 Aug;82(2):527-550
Figures