3854
Radiomics nomogram based on multiparametric MRI features for preoperative prediction of MGMT promoter methylation status in glioblastomas1Beijing Friendship Hospital, Capital Medical University, Beijing, China, 2Henan Cancer Hospital; Affiliated Cancer Hospital of Zhengzhou University, Zhengzhou, China
Synopsis
Keywords: Tumors (Pre-Treatment), Brain, Neuro
Motivation: Noninvasive measurement of the MGMT methylation status has great clinical significance for making a tailored treatment plan and prognosis assessment.
Goal(s): This study aimed to establish and validate a radiomics nomogram with robust radiomics features from ADC and ISO-CE-T1-weighted images.
Approach: The radiomics features were selected using LASSO regression. A radiomics nomogram combined radiomics signature and clinical factors were established with multivariate logistic regression analysis.
Results: The radiomics nomogram is a promising method. The Hosmer-Lemeshow test concluded that the radiomics nomogram showed goodness of fit. The decision curve showed that the addition of clinical characteristics to the nomogram showed incremental predictive value.
Impact: The multiparametric MRI-based radiomics nomogram was a promising method to preoperatively predict the MGMT mpromoter ethylation status noninvasively. Besides, the nomogram transformed the prediction signature into a visual and readable graph, making it easier to understand.
Introduction
Glioblastoma(GBM) is the most common malignant primary central nervous system tumor in adults1. Despite a comprehensive therapeutic approach combining maximum safe resection with radiotherapy and chemotherapy, prognosis is poor2. The O6-methylguanine-DNA methyltransferase(MGMT) is a DNA repair enzyme3. The methylation of the MGMT promoter can epigenetically silence the MGMT gene and increase the sensitivity of GBM to alkylating agents such as temozolomide(TMZ), making it a strong prognostic and predictive biomarker4-6. However, MGMT promoter methylation status is assessed invasively through biopsy or surgical resection with comparatively long detection periods and expensive fee7. The sample could not represent whole tumor and tissue in vitro is likely to degrade at any moment. The spatial and temporal heterogeneity could result in inaccurate results. Therefore, noninvasive measurement of the MGMT methylation status has great clinical significance.Radiomics, a recently emerging technique with high-throughput radiomics features, allows description of tumor heterogeneity8,9. Current studies showed potential correlations between MRI features and WHO grading10,11, molecular characteristics12-14, prognosis15,16 and clinical manifestations17. Several studies have focused on predicting MGMT methylation status based on conventional MRI18-21. Xi et al. focused on building radiomics signatures for predicting MGMT methylation status but the single sequence radiomics signatures showed unsatisfying accuracy of 67.54%(T1WI), 69.25%(T2WI) and 82.01%(CE-T1WI), respectively20.
The purpose of this study was, therefore, to investigate the imaging characteristics from multiparametric MRI images using a radiomics approach to construct a reliable radiomics nomogram for preoperative prediction of MGMT promoter methylation status in glioblastoma patients.
Methods
216 GBM patients in the local institution(151 in the training dataset and 65 in the test dataset) were retrospectively enrolled. MGMT promoter methylation status was assessed by pyrosequencing. GBM was defined as methylated if the average methylation rate ≥ 8%22,23. The external validation dataset(n=68) were collected with available MGMT methylation status and corresponding preoperative MRI from The Cancer Genome Atlas(TCGA) and The Cancer Imaging Atlas(TCIA)24,25. 851 features were extracted from ADC and ISO-CE-T1-weighted images using PyRadiomics software(Fig. 1).The radiomics features were selected using the least absolute shrinkage and selection operator(LASSO) method and three radiomics signatures were built based on ADC, ISO-CE-T1-weighted and joint sequences. The signature showing the best performance was selected for building a radiomics nomogram with clinical data using multivariate logistic regression. Hosmer-Lemeshow test were used to evaluate the calibration of the nomogram. The performance was assessed using receiver operating characteristic curve. Accuracy, sensitivity and specificity were calculated. Decision curve analysis was applied to reflect the clinical utility.
Results
The joint signature including six radiomics features showed the best performance(Fig. 2). A radiomics nomogram including the joint radscore and clinical characteristics(age and sex) was established(Fig. 3). The accuracy, sensitivity, specificity and AUC were 86.75%, 80.88 %, 90.36 %, 0.920(95%CI: 0.865-0.958) and 84.62%, 82.76%, 86.11%, 0.903(95%CI: 0.804-0.963) and 80.88%, 81.25%, 80.56%, 0.845(0.737-0.922) in the training, test and external validation dataset, respectively. The Hosmer-Lemeshow test concluded that the radiomics nomogram showed goodness of fit. The calibration curves were showed in Fig.4. The decision curve showed that the using the nomogram to predict MGMT promoter methylation status may add more benefit than using pyrosequencing after biopsy or surgical resection-all scheme or pyrosequencing-none scheme. Besides, adding the clinical data could obtain more net benefit(Fig. 5).Discussion
In this study, we described the tumor characteristics quantitatively with more comprehensive high-throughput radiomics features. A radiomics nomogram was constructed and validated in an entirely independent external validation cohort. The joint radiomics signature performed better than the single ADC and ISO-CE radiomics signature, suggesting that multiparametric MRI radiomics features may improve the prediction performance, which is consistent with Wei et al.’s conclusions18. Xi et al. constructed a prediction radiomics signature based on multi-sequence MRI(T1WI, T2WI and CE-T1WI) and increased the accuracy from 67.54% to 86.59% compared to single sequence radiomics signature20, which also showed the advantages of multiparametric MRI.The radiomics nomogram indicated the strong clinical potential to predict the MGMT promoter methylation status and the nomogram transformed the prediction signature into a visual and readable graph, making it easier to understand. A major reason for the excellent prediction performance may be the combination of both sequences, where ADC features offer distinguishable information of cell proliferation and ISO-CE-T1WI features provide accurate information of angiogenesis thanks to the injection of gadolinium, thin slice thickness (1 mm) compared to previous studies with the slice thickness of 3.0-5.0 mm20.
Conclusion
The radiomics nomogram is a promising approach for preoperatively predicting the MGMT promoter methylation status in glioblastomas patients noninvasively. The multiparametric MRI radiomics features may improve the prediction performance. The addition of clinical characteristics to the nomogram showed incremental predictive value.Acknowledgements
No acknowledgement found.References
1. Louis DN, Perry A, Wesseling P et al (2021) The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol 23:1231-1251
2. Ostrom QT, Gittleman H, Fulop J et al (2015) CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol 17 Suppl 4:v1-v62
3. Hegi ME, Diserens AC, Gorlia T et al (2005) MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 352:997-1003
4. Stupp R, Hegi ME, Mason WP et al (2009) Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncology 10:459-466
5. Bell EH, Zhang P, Fisher BJ et al (2018) Association of MGMT Promoter Methylation Status With Survival Outcomes in Patients With High-Risk Glioma Treated With Radiotherapy and Temozolomide: An Analysis From the NRG Oncology/RTOG 0424 Trial. JAMA Oncology 4:1405-1409
6. Gorlia T, van den Bent MJ, Hegi ME et al (2008) Nomograms for predicting survival of patients with newly diagnosed glioblastoma: prognostic factor analysis of EORTC and NCIC trial 26981-22981/CE.3. Lancet Oncology 9:29-38
7. Quillien V, Lavenu A, Sanson M et al (2014) Outcome-based determination of optimal pyrosequencing assay for MGMT methylation detection in glioblastoma patients. J Neurooncol 116:487-496
8. Lambin P, Leijenaar R, Deist TM et al (2017) Radiomics: the bridge between medical imaging and personalized medicine. Nature Reviews Clinical Oncology 14:749-762
9. Soni N, Priya S, Bathla G (2019) Texture Analysis in Cerebral Gliomas: A Review of the Literature. AJNR Am J Neuroradiol 40:928-934
10. Hwan-Ho C, Hyunjin P (2017) Classification of low-grade and high-grade glioma using multi-modal image radiomics features. Annu Int Conf IEEE Eng Med Biol Soc 2017:3081-3084
11. Lu CF, Hsu FT, Hsieh KL et al (2018) Machine Learning-Based Radiomics for Molecular Subtyping of Gliomas. Clinical Cancer Research 24:4429-4436
12. Park YW, Han K, Ahn SS et al (2018) Prediction of IDH1-Mutation and 1p/19q-Codeletion Status Using Preoperative MR Imaging Phenotypes in Lower Grade Gliomas. AJNR Am J Neuroradiol 39:37-42
13. Lu J, Li X, Li H (2021) Perfusion parameters derived from MRI for preoperative prediction of IDH mutation and MGMT promoter methylation status in glioblastomas. Magnetic Resonance Imaging 83:189-195
14. Li C, Yin J (2021) Radiomics Nomogram Based on Radiomics Score from Multiregional Diffusion-Weighted MRI and Clinical Factors for Evaluating HER-2 2+ Status of Breast Cancer. Diagnostics (Basel) 11
15. Zhou H, Vallieres M, Bai HX et al (2017) MRI features predict survival and molecular markers in diffuse lower-grade gliomas. Neuro Oncol 19:862-870
16. Kickingereder P, Neuberger U, Bonekamp D et al (2018) Radiomic subtyping improves disease stratification beyond key molecular, clinical, and standard imaging characteristics in patients with glioblastoma. Neuro Oncol 20:848-857
17. Liu Z, Wang Y, Liu X et al (2018) Radiomics analysis allows for precise prediction of epilepsy in patients with low-grade gliomas. Neuroimage Clin 19:271-278
18. Wei J, Yang G, Hao X et al (2019) A multi-sequence and habitat-based MRI radiomics signature for preoperative prediction of MGMT promoter methylation in astrocytomas with prognostic implication. European Radiology 29:877-888
19. Huang WY, Wen LH, Wu G et al (2021) Comparison of Radiomics Analyses Based on Different Magnetic Resonance Imaging Sequences in Grading and Molecular Genomic Typing of Glioma. J Comput Assist Tomogr 45:110-120
20. Xi YB, Guo F, Xu ZL et al (2018) Radiomics signature: A potential biomarker for the prediction of MGMT promoter methylation in glioblastoma. Journal of Magnetic Resonance Imaging 47:1380-1387
21. Li ZC, Bai H, Sun Q et al (2018) Multiregional radiomics features from multiparametric MRI for prediction of MGMT methylation status in glioblastoma multiforme: A multicentre study. European Radiology 28:3640-3650
22. Jiang C, Kong Z, Liu S et al (2019) Fusion Radiomics Features from Conventional MRI Predict MGMT Promoter Methylation Status in Lower Grade Gliomas. European Journal of Radiology 121:108714
23. Kong Z, Lin Y, Jiang C et al (2019) (18)F-FDG-PET-based Radiomics signature predicts MGMT promoter methylation status in primary diffuse glioma. Cancer Imaging 19:58
24. TCGA (2008) Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 455:1061-1068
25. Clark K, Vendt B, Smith K et al (2013) The Cancer Imaging Archive (TCIA): maintaining and operating a public information repository. Journal of Digital Imaging 26:1045-1057
Figures
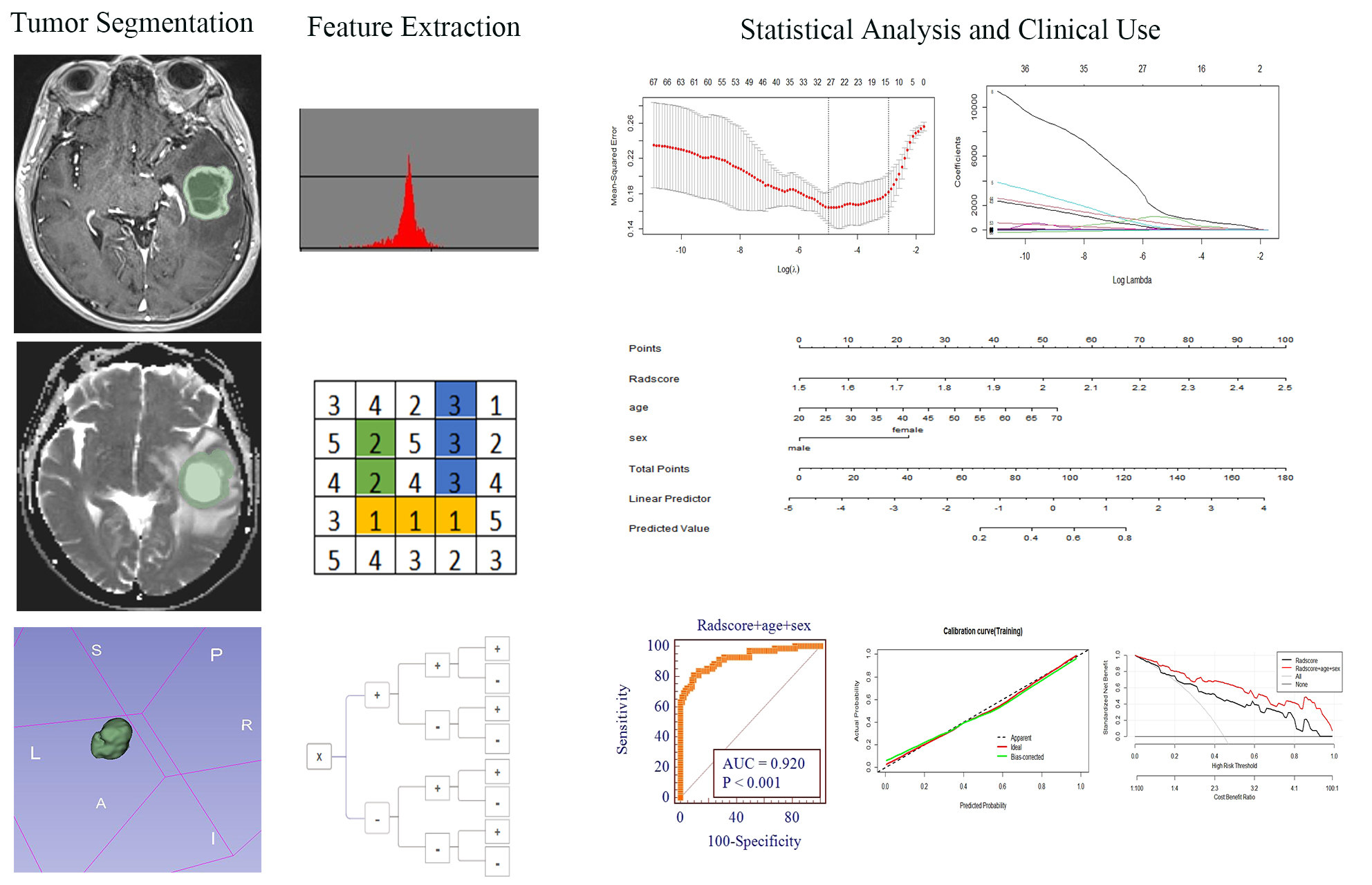
Fig. 1 Flow chart of study design. The case is a 50-year-old female glioblastoma patient with MGMT promoter methylation. The green area represents the volume of interest(VOI) of the whole tumor. Contours were drawn carefully to avoid involving peritumoral edema.
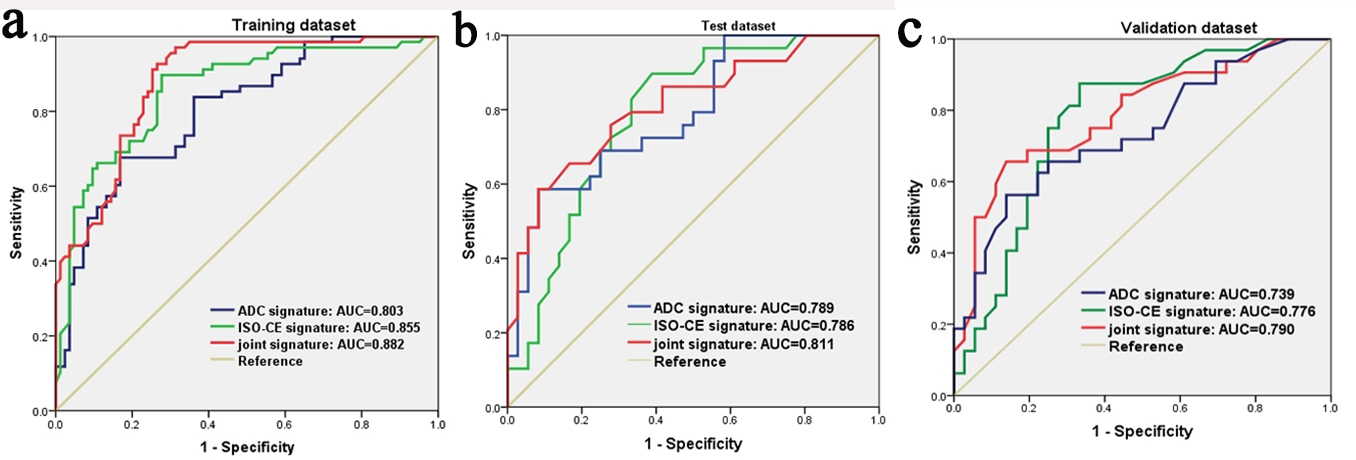
Fig. 2 Graph shows ROC curves of three radiomics signatures for predicting the MGMT promoter methylation status in the (a)training, (b)test and (c)validation dataset.
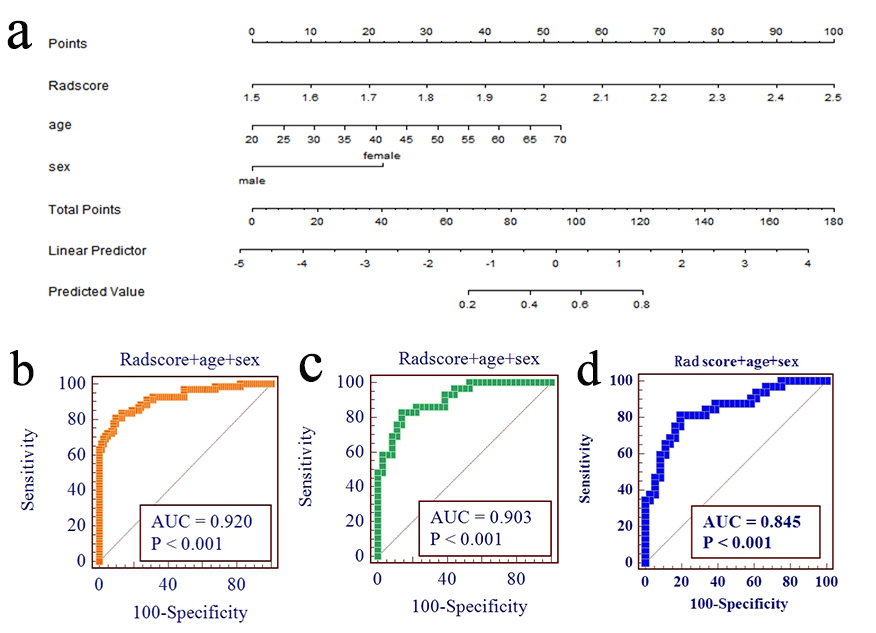
Fig. 3 (a)The radiomics nomogram included the radscore based on joint radiomics features and clinical characteristics(age and sex). ROC curves of the radiomics nomogram for predicting the MGMT promoter methylation status in the training(b), test(c) and validation(d) dataset.
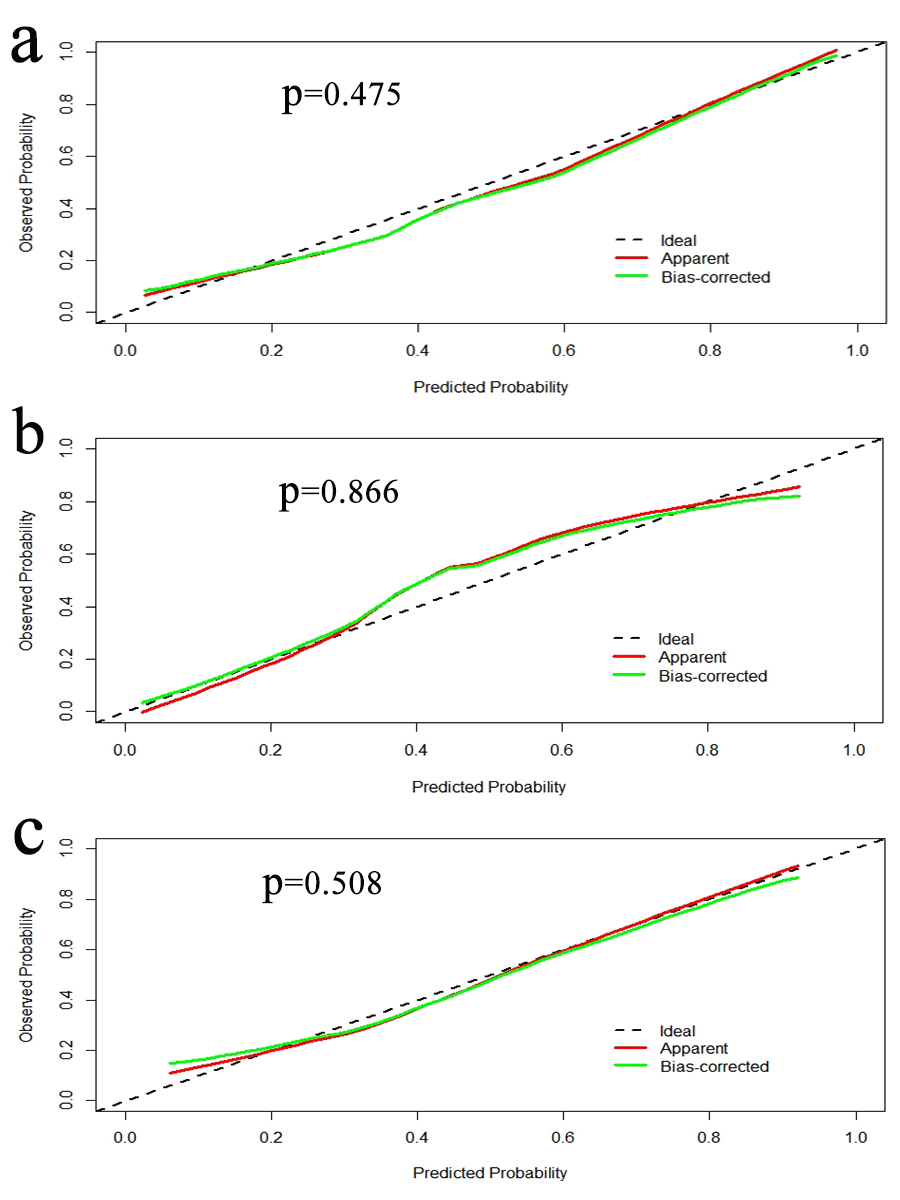
Fig. 4 Calibration curves of the radiomics nomogram in the training(a),test(b) and validation(c) datasets.
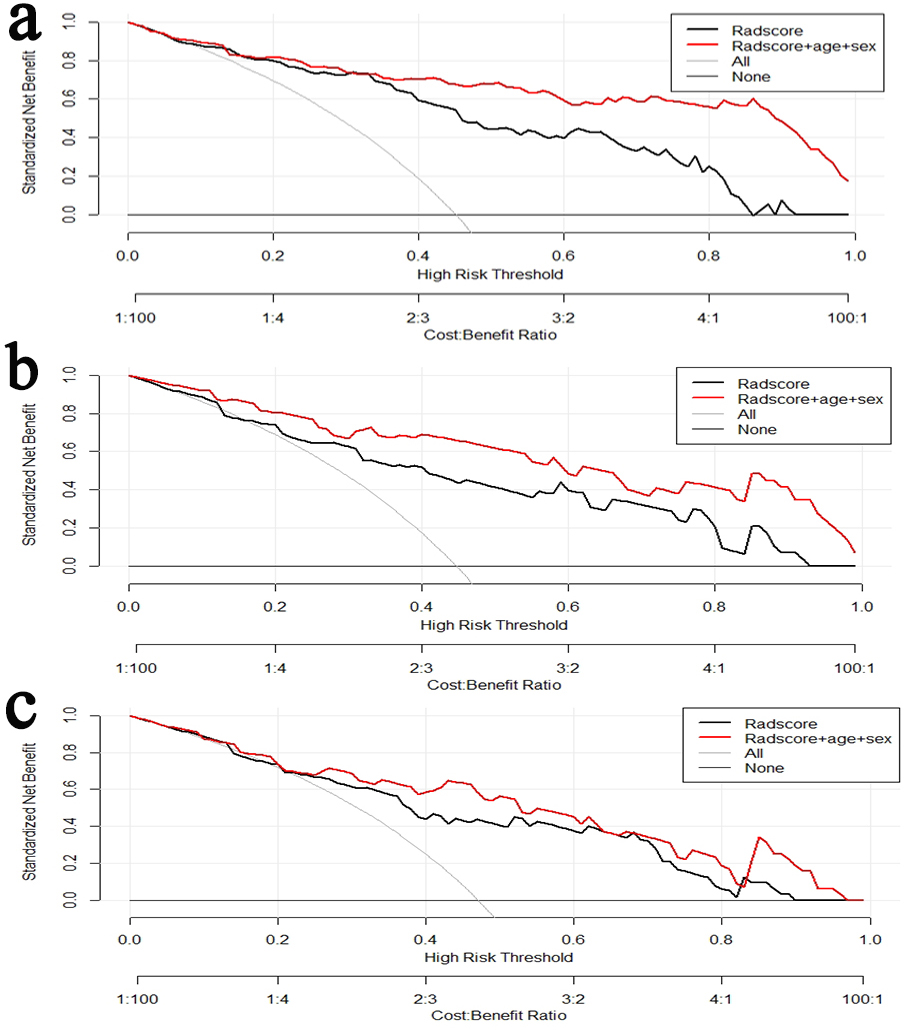
Fig. 5 Decision curve analysis for the radiomics nomogram(Radscore, age and sex) in the training(a), test(b) and validation(c) dataset. The y-axis represents the net benefit.