3850
Epilepsy and NANO scale are associated with pre-treatment glioblastoma lesion size and distinct brain regions1Radiology, German Cancer Research Center, Heidelberg, Germany, 2Neuroradiology, Heidelberg University Hospital, Heidelberg, Germany, 3Faculty of Medicine, Heidelberg University, Heidelberg, Germany, 4Neurology, Heidelberg University Hospital, Heidelberg, Germany, 5Functional Neuroanatomy, Heidelberg University, Heidelberg, Germany
Synopsis
Keywords: Tumors (Pre-Treatment), Brain
Motivation: Identifying brain regions where glioblastoma is associated with epilepsy or neurological deficits could help recognize patients with a higher risk of developing neurological symptoms based on MRI.
Goal(s): We aim to correlate clinical and radiological findings to improve diagnostic evaluation of pre-treatment glioblastoma patients.
Approach: MRIs from 557 patients with de-novo glioblastoma were analyzed retrospectively. We used NANO scale to report neurological deficits and analyzed lesion-frequency-maps for identifying deficits-associated regions.
Results: There was a significant correlation between the NANO scale and lesion volume. For each investigated domain with the NANO scale, radiologically correlated brain regions could be identified.
Impact: We showed that MRI examinations of pre-treatment glioblastoma patients can provide clinicians and patients valuable information regarding risk of developing certain neurological deficits and symptoms. Furthermore, NANO scale and epilepsy-status can provide information regarding the characteristics of the tumor lesion.
INTRODUCTION
Neurologic Assessment in Neuro-Oncology (NANO) evaluates neurological deficits in nine domains based on simple clinical examination1. We aim to correlate clinical and radiological findings to improve diagnostic evaluation of pre-treatment glioblastoma patients. Identifying brain regions where glioblastoma is associated with epilepsy, or any other neurological deficits and characterizing brain tumor characteristics could help recognize patients with developing a higher risk of seizures or symptoms based on magnetic resonance imaging (MRI).METHODS
We evaluated 3 Tesla MRI with Gadolinium contrast administration from 557 patients with pre-treatment IDH-wild-type glioblastoma retrospectively. Neurological deficits were assessed according to the NANO scale. Furthermore, 145 patients had a history of epilepsy before receiving the first-line treatment and 412 patients did not have any epileptic seizure before treatment. Contrast-enhancing tumor (CE) was segmented semi-automatically from postcontrast T1-weighted MRIs using HD-GLIO2,3. Lesion volumes from patients without any NANO scale relevant deficits or epilepsy were compared with symptomatic patients in at least one domain using Mann-Whitney U-tests. Images were registered to MNI-152-space. Voxel-wise Fisher-exact-test followed by random permutation analysis (ADIFFI) for multiple comparison correction4 was performed to identify regions with higher occurrence of tumors associated with the deficits. ADIFFI was performed for epilepsy and each domain of NANO: gait, strength, ataxia, sensation, visual fields, facial strength, language, level of consciousness and behavior.RESULTS
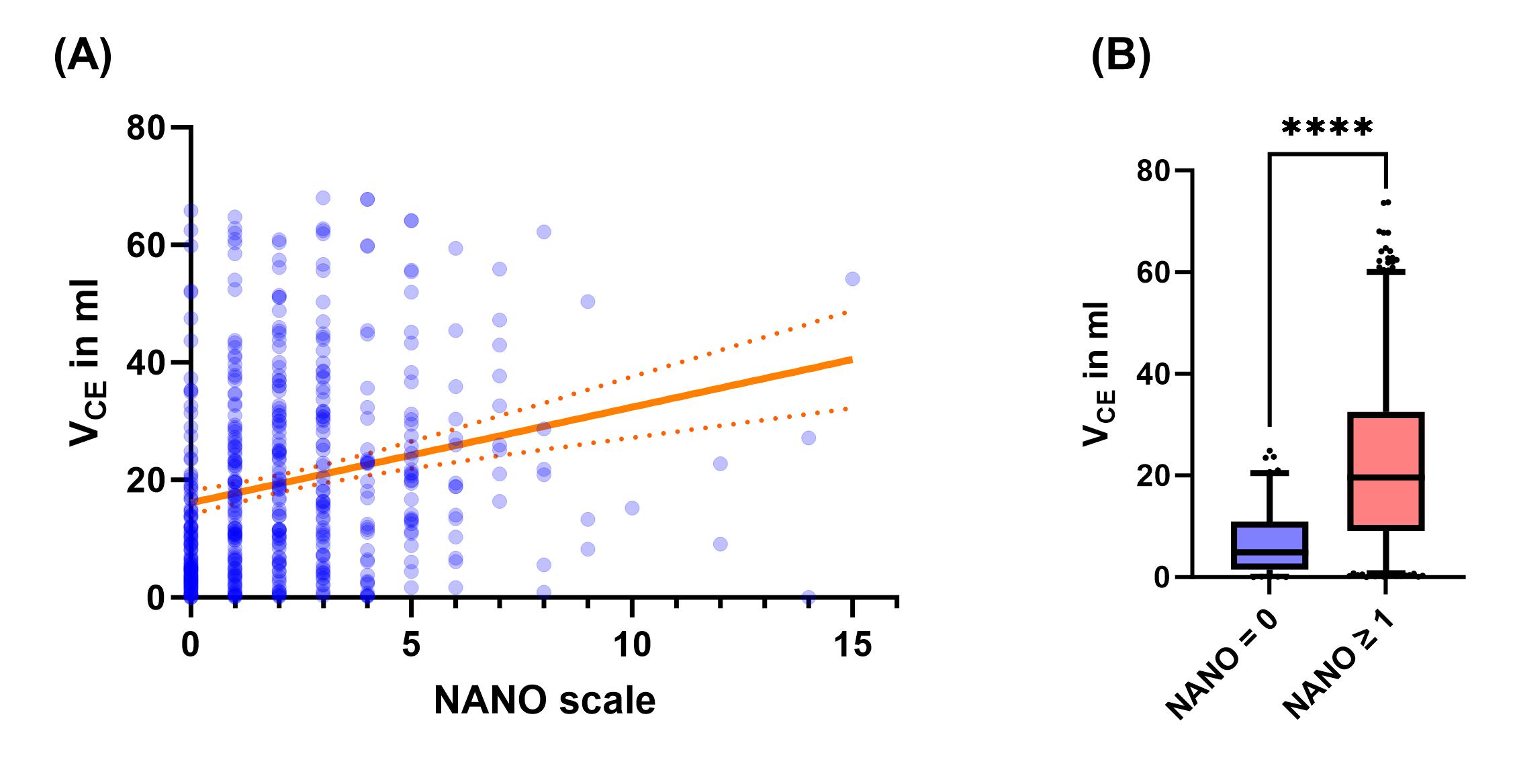
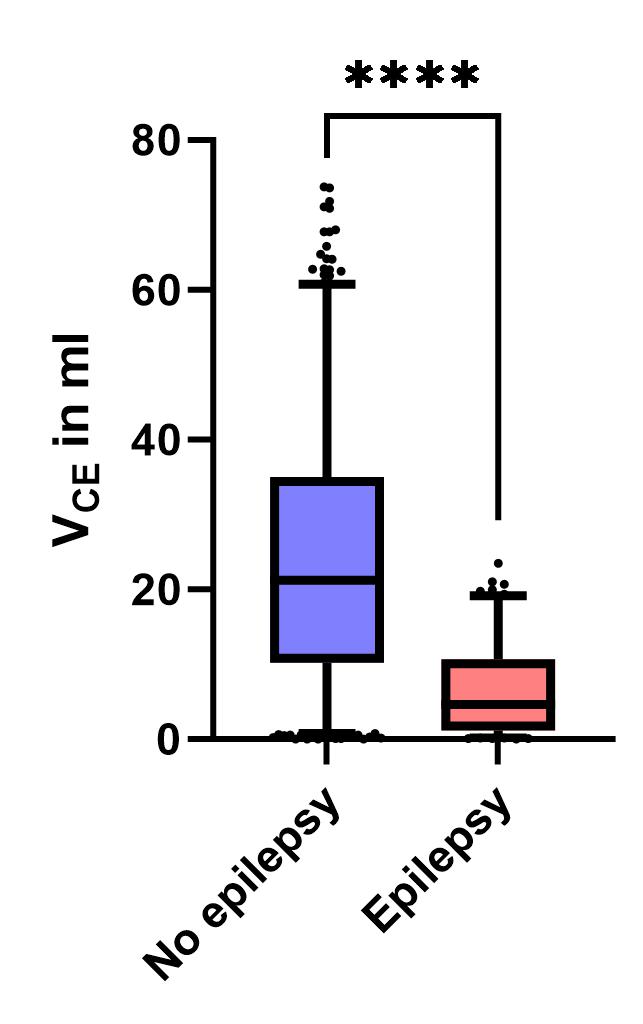
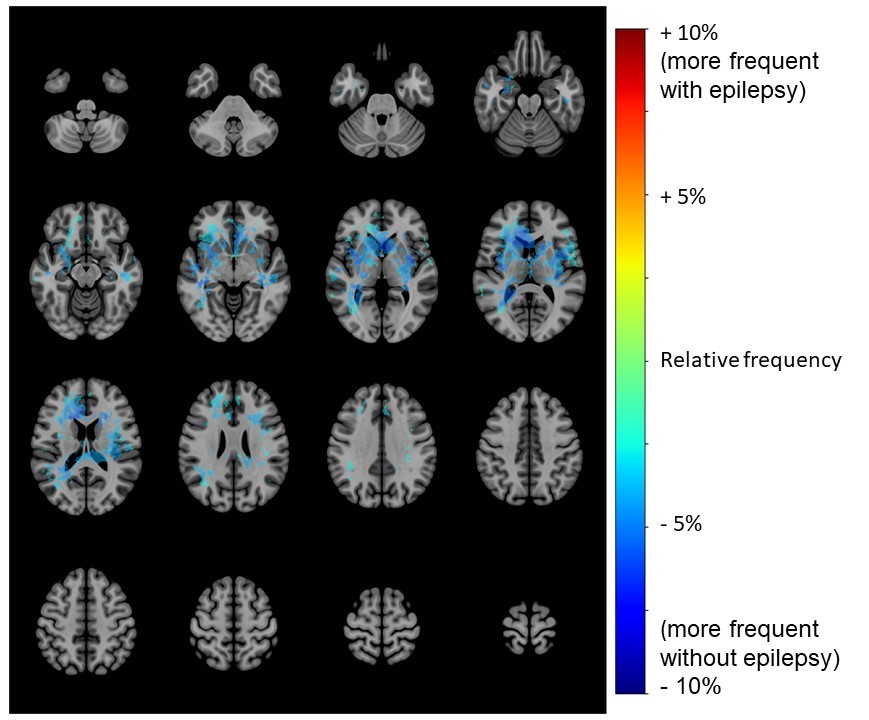
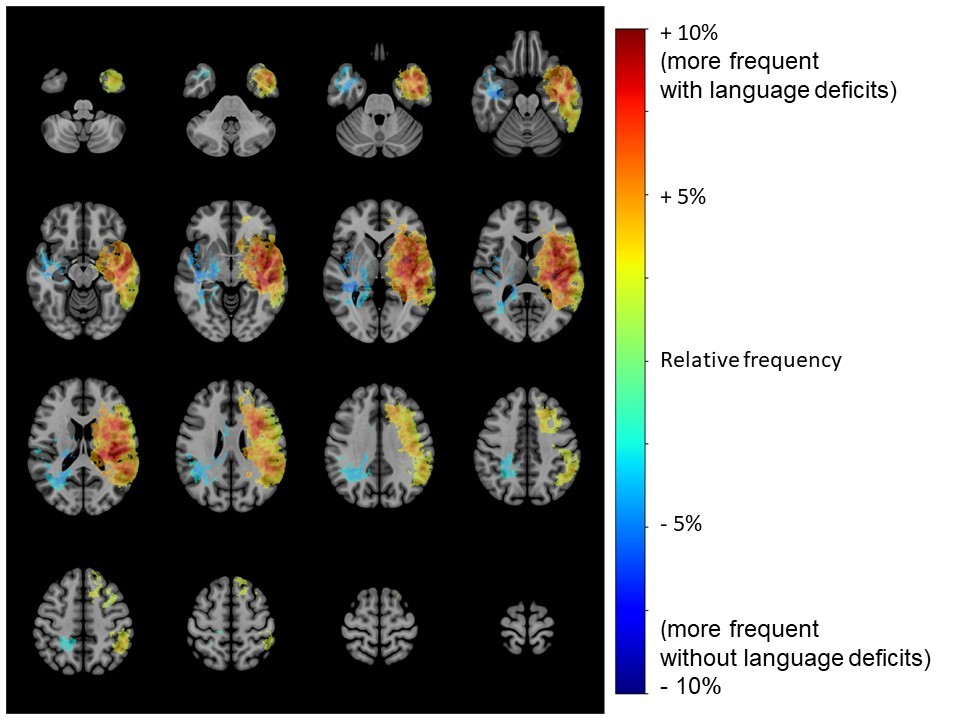
There was a significant correlation between NANO scale and CE lesion volume (Spearman r = 0.3098, p<0.0001, see figure 1). The volume of CE associated without any deficits (n=106, 6.93 ml ± 0.63 ml) was significantly smaller (p<0.0001) than lesions with deficits (n=373, 22.8 ml ± 0.9 ml), see figure 1. However, the CE lesion volume associated with epilepsy was smaller than lesions without epilepsy (6.57 ml ± 0.53 ml vs. 18.04 ml ± 0.90 ml; p<0.0001, see figure 2). For each investigated domain with the NANO scale, radiologically correlated brain regions could be identified with ADIFFI (example NANO domain: language – see figure 4). Regions, where epilepsy-related lesions were significantly more frequent, could not be found with ADIFFI. However, clusters were found in subcortical regions and in white matter (WM) around the thalamus, where occurrence of lesions without epilepsy was higher, suggesting a preference for grey matter (GM) in epilepsy-related lesions (see figure 3).DISCUSSION
The heterogeneous distribution of epilepsy-associated lesions and preference of GM is in accordance with previous studies5. However, the volume of symptomatic lesions was smaller, signifying that location and/or fraction of grey matter and white matter in tumor composition may be more important than tumor size. Furthermore, we found a clear association between NANO scale and glioblastoma lesion size and location, in line with other works using symptom lesion mapping6.CONCLUSION
Glioblastoma lesion located in subcortical regions are less associated with epilepsy. In cortical regions, the association of lesions with epilepsy was indeterminate according to ADIFFI analysis. NANO scale may provide an estimate of glioblastoma lesion volume. In addition, for certain domains of the NANO scale, neurological deficits are well associated with glioblastoma location. These findings suggest further investigations into the correlation between NANO and RANO criteria over time and their usefulness in the clinical management of glioblastoma.Acknowledgements
No acknowledgement found.References
- Nayak, L., et al., The Neurologic Assessment in Neuro-Oncology (NANO) scale: a tool to assess neurologic function for integration into the Response Assessment in Neuro-Oncology (RANO) criteria. Neuro-Oncology, 2017. 19(5): p. 625-635.
- Isensee, F., et al., nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nature Methods, 2021. 18(2): p. 203-211.
- Kickingereder, P., et al., Automated quantitative tumour response assessment of MRI in neuro-oncology with artificial neural networks: a multicentre, retrospective study. The Lancet Oncology, 2019. 20(5): p. 728-740.
- Ellingson, B.M., et al., Anatomic localization of O6-methylguanine DNA methyltransferase (MGMT) promoter methylated and unmethylated tumors: A radiographic study in 358 de novo human glioblastomas. NeuroImage, 2012. 59(2): p. 908-916.
- Schaper, F.L.W.V.J., et al., Mapping Lesion-Related Epilepsy to a Human Brain Network. JAMA Neurology, 2023. 80(9): p. 891-902. 6. Schiemanck, S.K., et al., Relationship between Ischemic Lesion Volume and Functional Status in the 2nd Week after Middle Cerebral Artery Stroke. Neurorehabilitation and Neural Repair, 2005. 19(2): p. 133-138
- Schiemanck, S.K., et al., Relationship between Ischemic Lesion Volume and Functional Status in the 2nd Week after Middle Cerebral Artery Stroke. Neurorehabilitation and Neural Repair, 2005. 19(2): p. 133-138.
Figures