3843
Value of whole-lesion histogram analysis based on ADC and ASL in predicting the response to chemotherapy and prognosis of PCNSL1Radiology, The First Medical Center, Chinese People’s Liberation Army General Hospital, Beijing, China
Synopsis
Keywords: Tumors (Pre-Treatment), Quantitative Imaging
Motivation: Primary central nervous system lymphoma (PCNSL) is a rare malignant non-Hodgkin's lymphoma with a poor prognosis, the combination chemotherapy regimen based on methotrexate is the main therapeutic regimen. There are no reliable indicators to predict the treatment response and survival outcome of PCNSL patients.
Goal(s): To predict the response to methotrexate (MTX) chemotherapy and prognosis in primary central nervous system lymphoma (PCNSL) patients by the histogram parameters based on apparent diffusion coefficient (ADC) and arterial spin labeling (ASL).
Approach: Use the univariate and multivariate logistic regressions to identify the independent predictors for the response of MTX chemotherapy. The predictive performance was assessed by the receiver operating characteristic. The Kaplan-Meier analysis and Cox regression were used to analyze the OS.
Results: Number of lesions (NL), the maximum of ADC values and the 95th percentile of CBF values were independent predictive factors of chemotherapy response.
Impact: ADC and CBF values are promising predictive factors of chemotherapy response and outcome in PCNSL patients.
Objective
To predict the chemotherapy response and overall survival (OS) in primary central nervous system lymphoma (PCNSL) patients by the histogram parameters of apparent diffusion coefficient (ADC) and cerebral blood flow (CBF) derived from diffusion-weighted imaging (DWI) and arterial spin labeling (ASL) respectively.Method
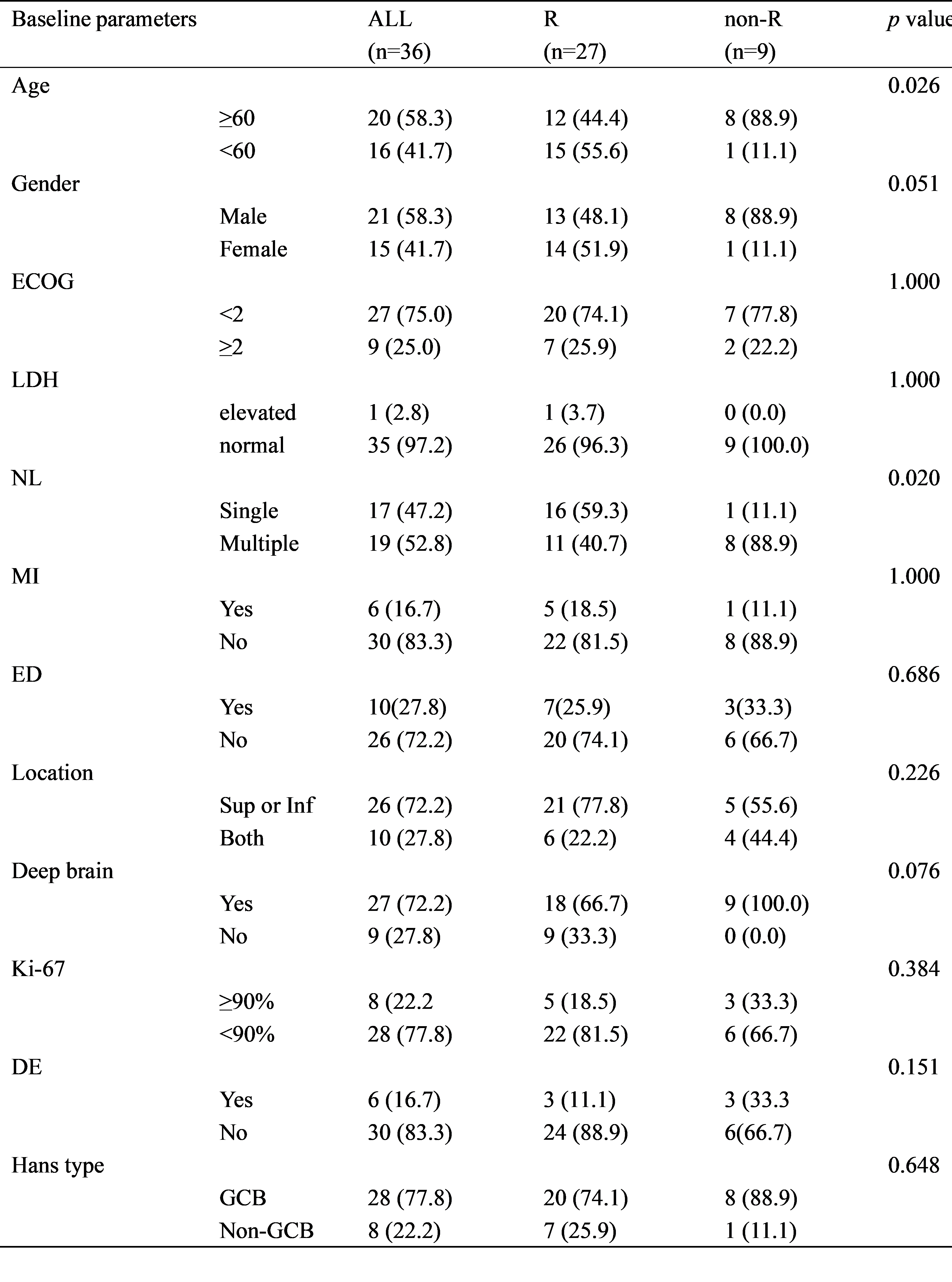
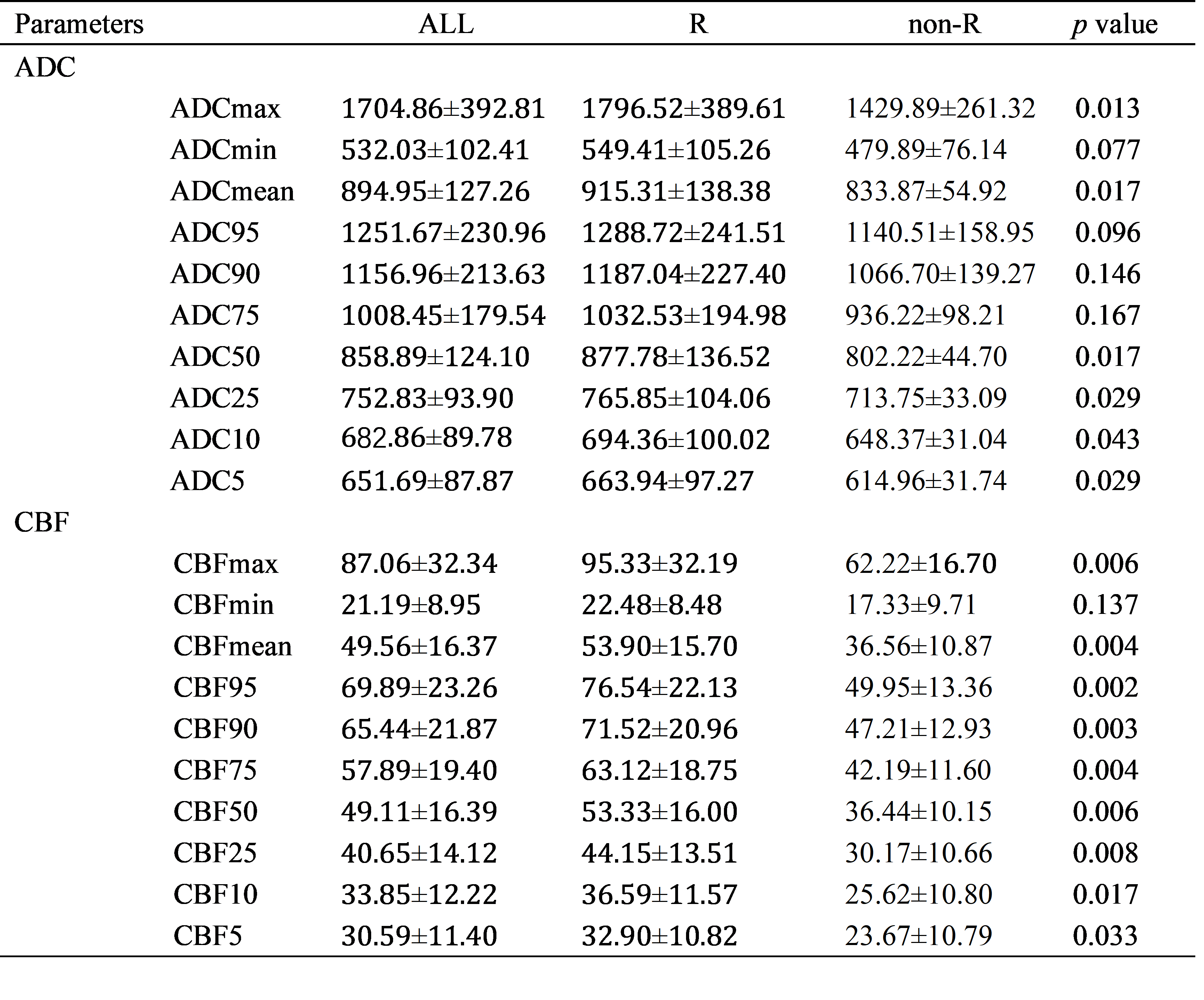
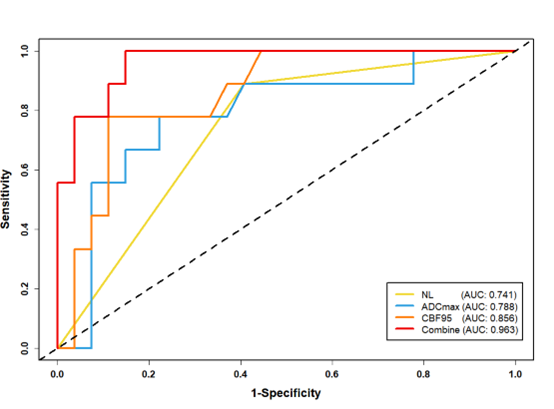
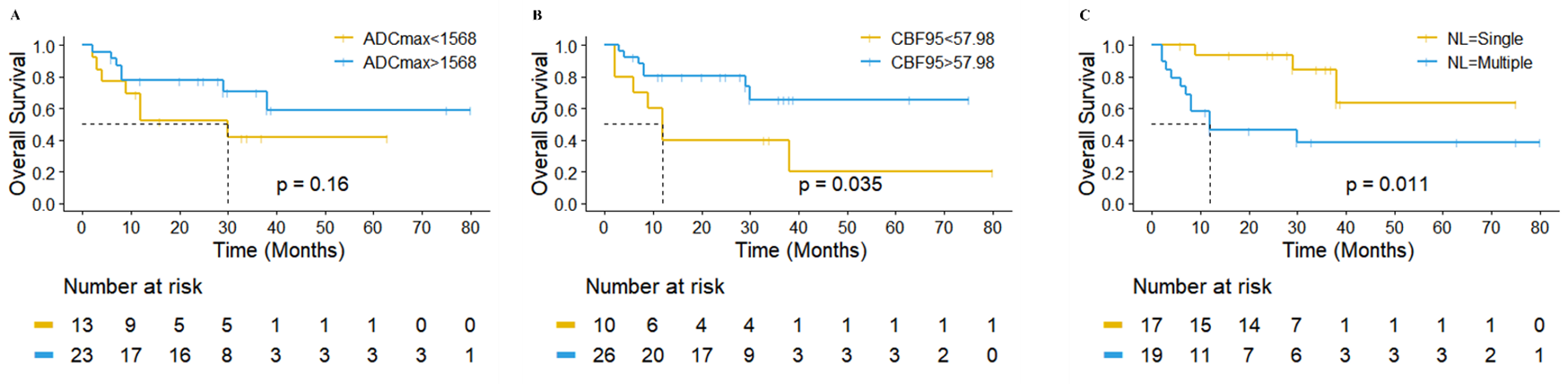
Thirty-six patients pathologically confirmed as primary central nervous system diffuse large B-cell lymphoma and treated with a combined MTX-based chemotherapy regimens were retrospectively involved in this study. The patients were divided into response group (R) and non-response group (non-R). The differences in Histogram parameters, including maximum, minimum, mean and the 5th, 10th, 25th, 50th, 75th 90th, and 95th percentiles extracted from ADC and CBF maps were analyzed between R and non-R groups. The univariate and multivariate logistic regressions were performed to identify the independent predictors for MTX chemosensitivity. The performance of independent predictive parameters and their combine prediction model were assessed by the receiver operating characteristic (ROC) analysis. The Kaplan-Meier analysis with Log-rank test and Cox regression were used to analyze the overall survival.Results
The proportion of patients with age>60 (p=0.026) and multiple lesions (p=0.020) in non-R group was significantly higher than R group. ADCmax, ADCmean, ADC5-50 percentiles, CBFmax, CBFmean and CBF5-95 percentiles in R group were significantly higher than non-R patients (all p<0.05). The number of lesions (NL), ADCmax and CBF95 were independent predictive factors of chemotherapy (p=0.034, p=0.048 and p=0.045). The combination model consisted of ADCmax, CBF95 and NL showed the best performance with the area under the ROC curve (AUC) of 0.963 (95% CI=0.910-1.000, p<0.001). The ROC analysis showed that the cut-off points of ADCmax was 1568.00 (AUC=0.788, 95%CI=0.605-0.972, p=0.011) and CBF95 was 57.98 (AUC=0.856, 95%CI=0.725-0.987, p=0.002). The patients with CBF95<57.98 (χ2=4.460, p=0.035) and multiple lesions (χ2=6.396, p=0.011) have significantly shorter OS. Multivariate Cox regression test showed that multiple lesions (HR, 3.796; 95%CI, 1.024-14.073; p =0.046) was an independent risk factor for poor OS.Conclusion
ADC and CBF quantitative histogram paraments are promising factors for the pre-treatment prediction of MTX chemotherapy response and outcome in PCNSL patients.Acknowledgements
Throughout the writing of this dissertation I have received a great deal of support and assistance.I would first like to thank my supervisor, Lin Ma, whose expertise was invaluable in formulating the research questions and methodology. Your insightful feedback pushed me to sharpen my thinking and brought my work to a higher level.I would particularly like to acknowledge my group mates for their wonderful collaboration and patient support.References
[1] Grommes C, Rubenstein J L, DeAngelis L M, et al. Comprehensive approach to diagnosis and treatment of newly diagnosed primary CNS lymphoma[J]. Neuro-Oncology, 2019, 21(3): 296-305.
[2] Schaff L R, Grommes C. Primary central nervous system lymphoma[J]. Blood, 2022, 140(9): 971-979. [3] Chen T, Liu Y, Wang Y, et al. Evidence-based expert consensus on the management of primary central nervous system lymphoma in China[J]. Journal of Hematology & Oncology, 2022, 15(1): 136.
[4] van der Meulen M, Dinmohamed A G, Visser O, et al. Improved survival in primary central nervous system lymphoma up to age 70 only: a population-based study on incidence, primary treatment and survival in the Netherlands, 1989-2015[J]. Leukemia, 2017, 31(8): 1822-1825.
[5] Zhang Y, Zhou D B. Primary central nervous system lymphoma: status and advances in diagnosis, molecular pathogenesis, and treatment[J]. Chinese Medical Journal, 2020, 133(12): 1462-1469.
[6] Calimeri T, Steffanoni S, Gagliardi F, et al. How we treat primary central nervous system lymphoma[J]. ESMO Open, 2021, 6(4).
[7] Hoang-Xuan K, Deckert M, Ferreri A J M, et al. European Association of Neuro-Oncology (EANO) guidelines for treatment of primary central nervous system lymphoma (PCNSL)[J]. Neuro-Oncology, 2023, 25(1): 37-53.
[8] Fox C P, Phillips E H, Smith J, et al. Guidelines for the diagnosis and management of primary central nervous system diffuse large B-cell lymphoma[J]. British Journal of Haematology, 2019, 184(3): 348-363.
[9] Abrey L E, Ben-Porat L, Panageas K S, et al. Primary Central Nervous System Lymphoma: The Memorial Sloan-Kettering Cancer Center Prognostic Model[J]. Journal of Clinical Oncology, 2006, 24(36): 5711-5715.
[10] A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma - PMC[EB].
[11] Barajas R F, Politi L S, Anzalone N, et al. Consensus recommendations for MRI and PET imaging of primary central nervous system lymphoma: guideline statement from the International Primary CNS Lymphoma Collaborative Group (IPCG)[J]. Neuro-Oncology, 2021, 23(7): 1056-1071.
[12] Cui Y, Yang W, Ren J, et al. Prognostic value of multiparametric MRI-based radiomics model: Potential role for chemotherapeutic benefits in locally advanced rectal cancer[J]. Radiotherapy and Oncology, 2021, 154: 161-169.
[13] Schmainda K M, Prah M, Connelly J, et al. Dynamic-susceptibility contrast agent MRI measures of relative cerebral blood volume predict response to bevacizumab in recurrent high-grade glioma[J]. Neuro-Oncology, 2014, 16(6): 880-888.
[14] Kim S Y, Cho N, Park I A, et al. Dynamic Contrast-enhanced Breast MRI for Evaluating Residual Tumor Size after Neoadjuvant Chemotherapy[J]. Radiology, 2018, 289(2): 327-334.
[15] Wong E C. An introduction to ASL labeling techniques[J]. Journal of magnetic resonance imaging: JMRI, 2014, 40(1): 1-10.
[16] Pang H, Dang X, Ren Y, et al. 3D-ASL perfusion correlates with VEGF expression and overall survival in glioma patients: Comparison of quantitative perfusion and pathology on accurate spatial location-matched basis[J]. Journal of magnetic resonance imaging: JMRI, 2019, 50(1): 209-220.
[17] Iima M, Partridge S C, Le Bihan D. Six DWI questions you always wanted to know but were afraid to ask: clinical relevance for breast diffusion MRI[J]. European Radiology, 2020, 30(5): 2561-2570.
[18] Chong, Ostrom, Khan, et al. Whole Tumor Histogram Analysis Using DW MRI in Primary Central Nervous System Lymphoma Correlates with Tumor Biomarkers and Outcome[J]. Cancers, 2019, 11(10): 1506.
[19] Ferreri A J M, Blay J Y, Reni M, et al. Prognostic Scoring System for Primary CNS Lymphomas: The International Extranodal Lymphoma Study Group Experience[J]. Journal of Clinical Oncology, 2003, 21(2): 266-272.
[20] Staiger A M, Ziepert M, Horn H, et al. Clinical Impact of the Cell-of-Origin Classification and the MYC/ BCL2 Dual Expresser Status in Diffuse Large B-Cell Lymphoma Treated Within Prospective Clinical Trials of the German High-Grade Non-Hodgkin’s Lymphoma Study Group[J]. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 2017, 35(22): 2515-2526.
[21] Swerdlow S H, Campo E, Pileri S A, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms[J]. Blood, 2016, 127(20): 2375-2390.
[22] Cho U, Oh W J, Hong Y K, et al. Prognostic Significance of High Ki-67 Index and Histogenetic Subclassification in Primary Central Nervous System Lymphoma[J]. Applied immunohistochemistry & molecular morphology: AIMM, 2018, 26(4): 254-262.
[23] Abrey L E, Batchelor T T, Ferreri A J M, et al. Report of an International Workshop to Standardize Baseline Evaluation and Response Criteria for Primary CNS Lymphoma[J]. Journal of Clinical Oncology, 2005, 23(22): 5034-5043.
[24] Guo Y, Kong Q C, Zhu Y Q, et al. Whole-lesion histogram analysis of the apparent diffusion coefficient: Evaluation of the correlation with subtypes of mucinous breast carcinoma[J]. Journal of magnetic resonance imaging: JMRI, 2018, 47(2): 391-400.
[25] Cao T, Jiang R, Zheng L, et al. T1 and ADC histogram parameters may be an in vivo biomarker for predicting the grade, subtype, and proliferative activity of meningioma[J]. European Radiology, 2023, 33(1): 258-269.
[26] Ma X, Ren X, Shen M, et al. Volumetric ADC histogram analysis for preoperative evaluation of LVSI status in stage I endometrioid adenocarcinoma[J]. European Radiology, 2022, 32(1): 460-469.
[27] Liang H Y, Huang Y Q, Yang Z X, et al. Potential of MR histogram analyses for prediction of response to chemotherapy in patients with colorectal hepatic metastases[J]. European Radiology, 2016, 26(7): 2009-2018.
[28] Gao A, Zhang H, Yan X, et al. Whole-Tumor Histogram Analysis of Multiple Diffusion Metrics for Glioma Genotyping[J]. Radiology, 2022, 302(3): 652-661.
[29] Hatzl S, Posch F, Deutsch A, et al. Immunohistochemistry for c-myc and bcl-2 overexpression improves risk stratification in primary central nervous system lymphoma[J]. Hematological Oncology, 2020, 38(3): 277-283.
[30] Kim S, Nam S J, Kwon D, et al. MYC and BCL2 overexpression is associated with a higher class of Memorial Sloan-Kettering Cancer Center prognostic model and poor clinical outcome in primary diffuse large B-cell lymphoma of the central nervous system[J]. BMC cancer, 2016, 16: 363.
[31] Lossos C, Bayraktar S, Weinzierl E, et al. LMO2 and BCL6 are associated with improved survival in primary central nervous system lymphoma[J]. British Journal of Haematology, 2014, 165(5): 640-648.
[32] Bessell E M, Graus F, Lopez-Guillermo A, et al. Primary non-Hodgkin’s lymphoma of the CNS treated with CHOD/BVAM or BVAM chemotherapy before radiotherapy: long-term survival and prognostic factors[J]. International Journal of Radiation Oncology*Biology*Physics, 2004, 59(2): 501-508.
[33] Zhang Y, Zhang Q, Wang X x., et al. Value of pretherapeutic DWI in evaluating prognosis and therapeutic effect in immunocompetent patients with primary central nervous system lymphoma given high-dose methotrexate-based chemotherapy: ADC-based assessment[J]. Clinical Radiology, 2016, 71(10): 1018-1029.
[34] Luo X, Zhu Y, Zhang Y, et al. Parameters of MR perfusion-weighted imaging predict the response and prognosis to high-dose methotrexate-based chemotherapy in immunocompetent patients with primary central nervous system lymphoma[J]. Journal of Clinical Neuroscience: Official Journal of the Neurosurgical Society of Australasia, 2022, 95: 151-158.
[35] Takeuchi H, Matsuda K, Kitai R, et al. Angiogenesis in primary central nervous system lymphoma (PCNSL)[J]. Journal of Neuro-Oncology, 2007, 84(2): 141-145.
[36] Valles F E, Perez-Valles C L, Regalado S, et al. Combined Diffusion and Perfusion MR Imaging as Biomarkers of Prognosis in Immunocompetent Patients with Primary Central Nervous System Lymphoma[J]. American Journal of Neuroradiology, 2013, 34(1): 35-40.
Figures