3838
Differentiating Brain Metastases Recurrence from Treatment-Induced Changes Using Velocity-Selective ASL: Initial Experience1F.M. Kirby Research Center, Kennedy Krieger Institute, Baltimore, MD, United States, 2Department of Radiology and Radiological Science, Johns Hopkins School of Medicine, Baltimore, MD, United States, 3Department of Radiation Oncology and Molecular Radiation Sciences, Johns Hopkins School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: Tumors (Post-Treatment), Arterial spin labelling, Brain Metastasis
Motivation: Brain metastases (BM) have increased frequency of treatment-related changes difficult to distinguish from progressive disease. To date, there are no studies evaluating arterial spin labeling (ASL) for BM patients during post-therapy follow-up.
Goal(s): To evaluate the feasibility of velocity-selective ASL (VSASL) derived cerebral blood flow (CBF) mapping in differentiating metastases recurrence from treatment-induced changes.
Approach: VSASL was applied to 9 BM patients, and compared with pseudo-continuous ASL (PCASL), dynamic susceptibility contrast perfusion-weighted imaging (DSC-PWI), and pathologic confirmation for some patients.
Results: VSASL is clinically feasible and more comparable with DSC-PWI than PCASL in patients with treated BM at suspicion of tumor progression.
Impact: This study showed that velocity-selective arterial spin labeling has the potential to offer a non-invasive alternative to dynamic susceptibility contrast perfusion-weighted imaging in differentiating tumor recurrence from treatment-induced changes among patients with brain metastases.
Introduction
Brain metastases (BM) after radiation therapy have increased frequency of treatment-related changes including radiation necrosis that are difficult to distinguish from progressive disease, as both manifest as enhancing masses. While perfusion provides useful additional characterization, associated hemorrhage in BM and treated BM brings susceptibility artifacts and limits the usage of dynamic susceptibility contrast perfusion-weighted imaging (DSC-PWI). Arterial spin labeling (ASL) is ideal for frequent non-invasive longitudinal monitoring and may serve as a viable alternative. However, most ASL studies were conducted among brain glioma patients.1 To date, there are no studies evaluating ASL methods for BM patients during their post-therapy follow-up. In this work, we evaluated the feasibility of velocity-selective ASL (VSASL) derived cerebral blood flow (CBF) mapping in differentiating metastases recurrence from treatment-induced changes, and compared to pseudo-continuous ASL (PCASL) and DSC-PWI.Methods
Experiments were conducted on a 3T Philips scanner using a 32-channel head-only receive coil. Nine patients with BM (age 63.1±6.0yo, 5F) (Table 1) were enrolled with written informed consent for a total of 10 scans (patient #1 was scanned twice 11 weeks apart).VS-inversion-based VSASL2 was applied with a global pre-saturation followed by a 2s delay, Vcut=2.0cm/s (duration=64ms),3 bolus duration=1400ms,3 and 3 background suppression (BS) pulses. PCASL was applied with labeling duration=1800ms, post labeling delay=2000ms, and 4 BS pulses. Both ASL applied vascular crushing modules with Vcut=2.0cm/s. ASL images were acquired in axial view with FOV=220×220×120mm3 and resolution=3.4×3.4×5mm3. 3D stack-of-spiral turbo FLASH readout4 was adopted with turbo factor=24 in the slice direction, centric ordering, flip angle=15°, TR/TE=18/2.6ms, readout time=11ms, 3-shot per image, label/control pairs=8, shot interval=4.3/3.9s and scan time=3.4/3.1min for PCASL/VSASL respectively. A proton-density weighted image (TR=10s) was acquired for CBF normalization.
In addition, DSC-PWI images were acquired during the first pass of gadoteridol using EPI sequence with 100 dynamic scans, TR/TE=1499/29ms, flip angle=60°, EPI factor=33, SENSE factor=2.5, FOV=212×185mm2, resolution=2.2×2.3mm2, and 28 total slices with thickness=4mm without gap. After that, a post-contrast T1-weighted image was acquired using 3D MPRAGE sequence with TR/TE=6.2/2.9ms, flip angle=9°, TFE factor=256, shot interval=2.5s, inversion time=900ms, CS-SENSE factor=3, sagittal FOV=220×220×192mm3 and resolution=1×1×1mm3.
All images were reconstructed online by the vendor, including spiral reconstruction/deblurring, SNESE and CS-SENSE. ASL-derived CBF maps (ASL-CBF) were quantified with formulas in publications2,3. DSC-PWI-derived CBF maps (DSC-CBF) were processed with Olea Sphere software (Olea Medical, La Ciotat, France).
Pearson correlation coefficients (PCC) of the whole map were calculated between the DSC-CBF (reference) and ASL-CBF as a similarity metric. The PCCs of DSC-CBF vs. VSASL-derived CBF (VSASL-CBF) and DSC-CBF vs. PCASL-derived CBF (PCASL-CBF) were calculated respectively and compared. Pathologic confirmation was available for some patients.
Results and Discussion
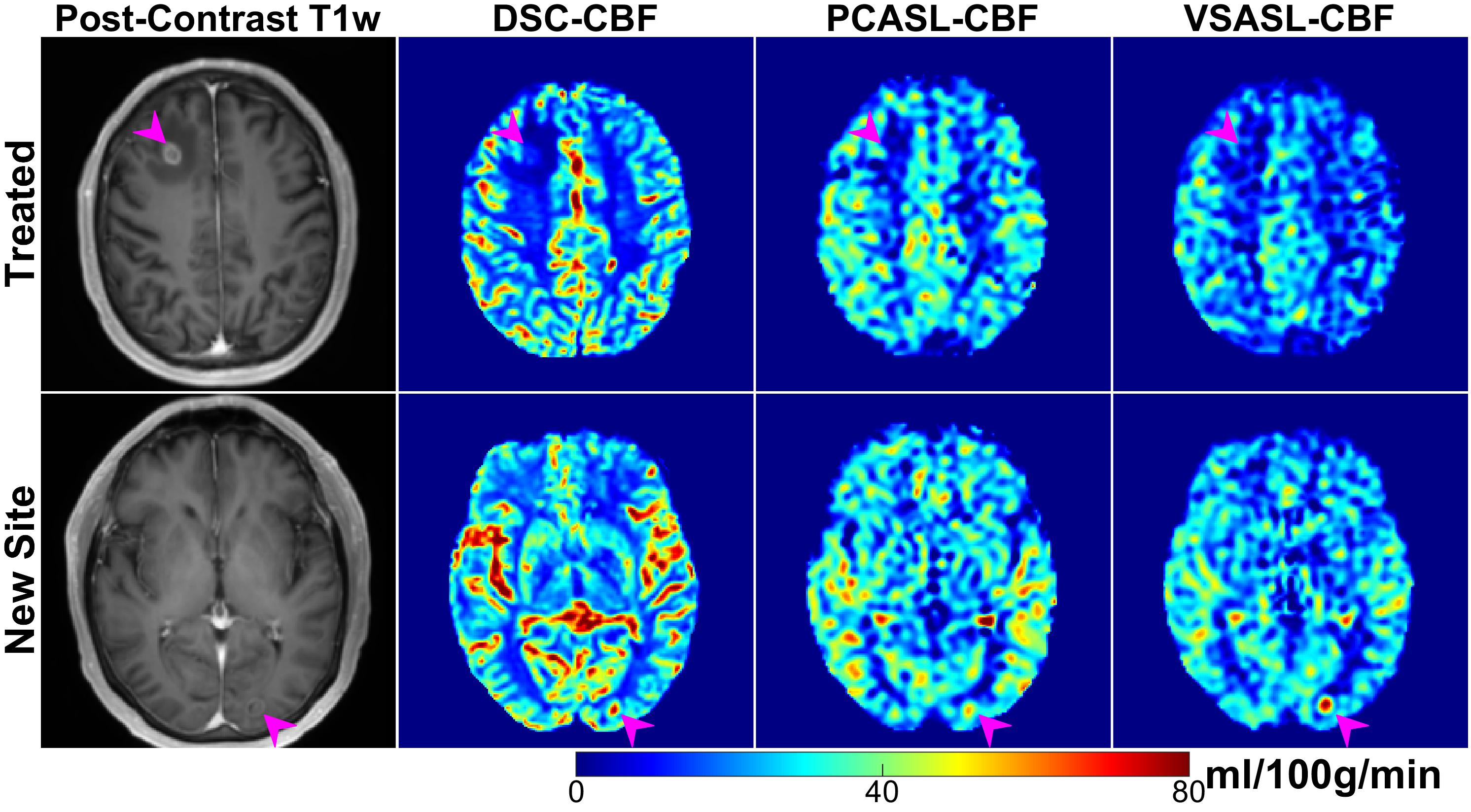
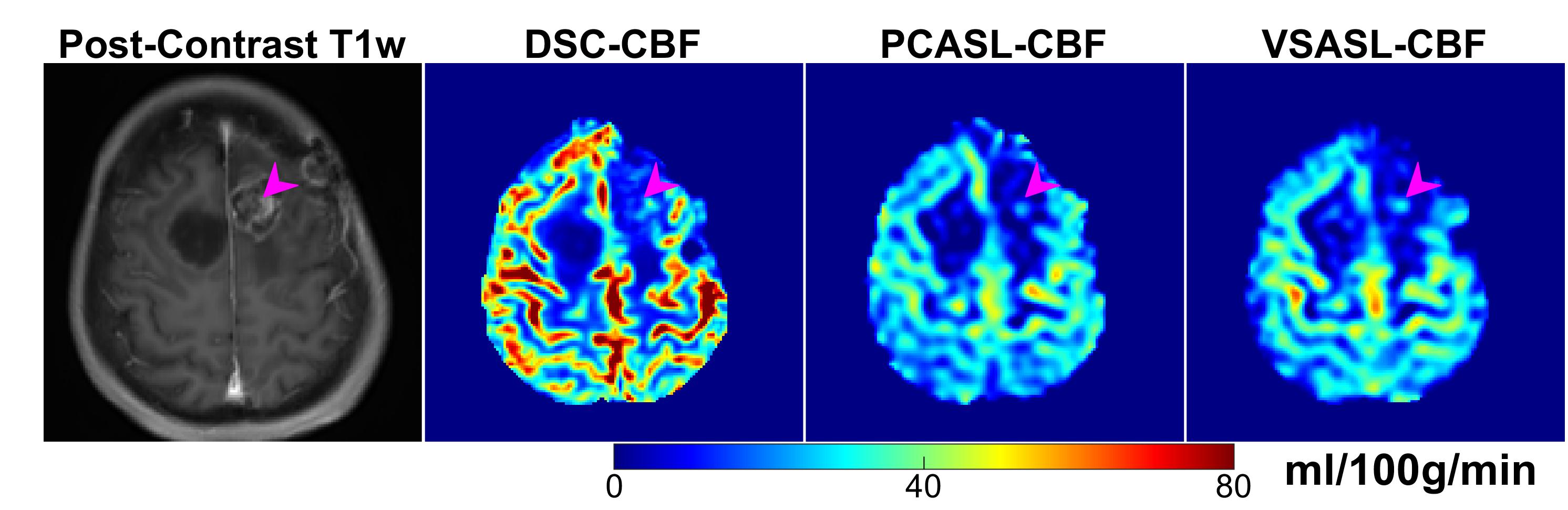
Figure 1 demonstrates a patient with lung cancer metastasis 5 years after radiosurgery to the right frontal lesion (top) and a new left occipital lesion (bottom). Both ASL-CBF maps revealed hypoperfusion of the right frontal lesion (top) progressing on contrast-enhanced imaging, agreed with DSC-CBF, and a surgical pathology exam 2 months later suggested reactive changes compatible with treatment effect and no evidence of viable carcinoma. The new concurrently identified and untreated left occipital lesion (bottom) had hyperperfusion on all CBF maps and both DSC-CBF and VSASL-CBF were more sensitive than PCASL-CBF.Figure 2 displays the recurrence of a radiosurgery-treated metastatic gallbladder spread to the left frontal lobe. All CBF maps showed hyperperfusion at the lesion spot, which is more visible in VSASL-CBF than in PCASL-CBF. Surgical resection confirmed tumor.
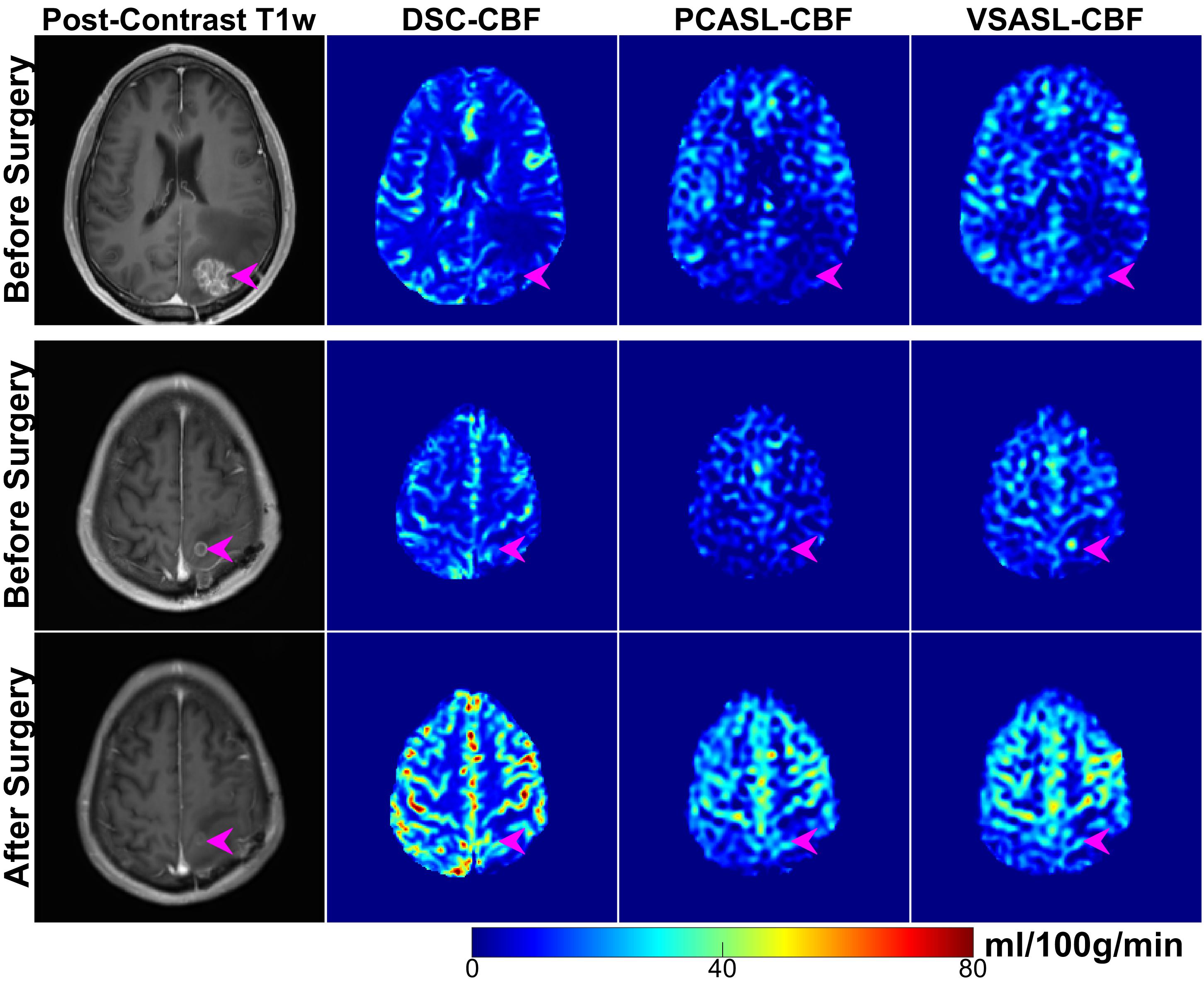
Figure 3 is from a patient with rectal cancer after radiosurgery to a left occipital lesion (top). Although the occipital lesion progressed on contrast-enhanced imaging, it was hypoperfused (top) whereas a newly detected small lesion was hyperperfused (middle). VSASL-CBF revealed the hyperperfusion better than DSC-CBF and PCASL-CBF. The new metastasis was treated with radiosurgery and was normal on follow-up 8 weeks later (bottom), indicating potential as a biomarker for treatment response.
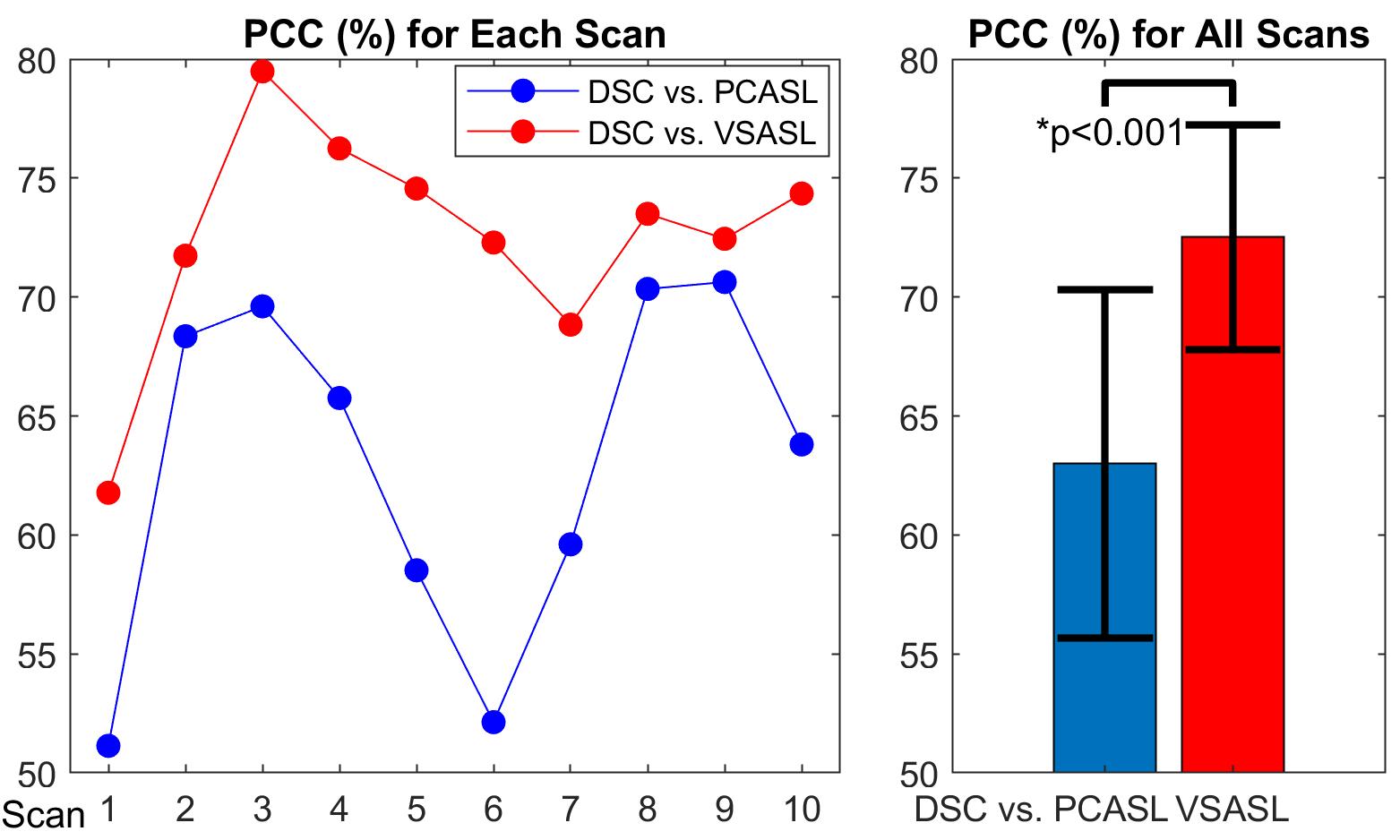
In Figure 4, the PCCs of DSC-CBF vs. VSASL-CBF were higher than DSC-CBF vs. PCASL-CBF for all 10 scans (left) and about +10% higher (t-test p<0.001) overall (right). The better performance of VSASL compared to PCASL agreed with the result from a recent study on patients with untreated high-grade glioma,5 both attributed to the mitigated susceptibility of VSASL to the prolonged arterial transit time of tortuous vessels within tumor vasculature.
Conclusion
These first results indicate that VSASL is clinically feasible and has the potential to offer a non-invasive alternative to DSC-PWI to guide clinical management in patients with treated BM at suspicion of tumor progression. Further research is needed to validate this perfusion method in a larger cohort for its robustness in distinguishing tumor recurrence from treatment effect.Acknowledgements
No acknowledgement found.References
1. Lindner T, Bolar DS, Achten E, et al. Current state and guidance on arterial spin labeling perfusion MRI in clinical neuroimaging. Magnetic Resonance in Med. 2023;89(5):2024-2047.
2. Qin Q, van Zijl PCM. Velocity-selective-inversion prepared arterial spin labeling: Velocity-Selective-Inversion Prepared ASL. Magn Reson Med. 2016;76(4):1136-1148.
3. Qin Q, Alsop DC, Bolar DS, et al. Velocity‐selective arterial spin labeling perfusion MRI: A review of the state of the art and recommendations for clinical implementation. Magnetic Resonance in Med. 2022;88(4):1528-1547.
4. Zhu D, Xu F, Liu D, et al. Evaluation of 3D stack‐of‐spiral turbo FLASH acquisitions for pseudo‐continuous and velocity‐selective ASL–derived brain perfusion mapping. Magnetic Resonance in Med. 2023;90(3):939-949.
5. Qu Y, Kong D, Wen H, et al. Perfusion measurement in brain gliomas using velocity-selective arterial spin labeling: comparison with pseudo-continuous arterial spin labeling and dynamic susceptibility contrast MRI. Eur Radiol. 2022;32(5):2976-2987.
Figures