3837
Differentiation of Brain Metastases from Different Pathological Types of Lung Cancers by Using Radiomic Features of the Edema and Tumor Region1Second Affiliated Hospital of Nanchang University, Nanchang, China
Synopsis
Keywords: Tumors (Pre-Treatment), Cancer
Motivation: Prediction of brain metastases from different pathological types of lung cancers.
Goal(s): To develop a radiomic model based on the peritumoral edema and tumor region for tumor type prediction of brain metastases from different pathological types of lung cancers.
Approach: Collect lung cancer patients, establish radiomics models, and test the model's differentiation of lesions.
Results: The radiomic model could effectively differentiate two pathological types of brain metastasis from lung cancer.
Impact: The radiomic model based on the edema and tumor region could effectively differentiate two pathological types of brain metastasis from lung cancer. It is expected to provide an imaging basis for clinicians to evaluate prognosis and formulate personalized treatment plans.
Purpose
To develop a radiomic model based on the peritumoral edema and tumor region for tumor type prediction of different brain metastases from different pathological types of lung cancers for patients with unknown primary lesion at the time of diagnosis.Materials and Methods
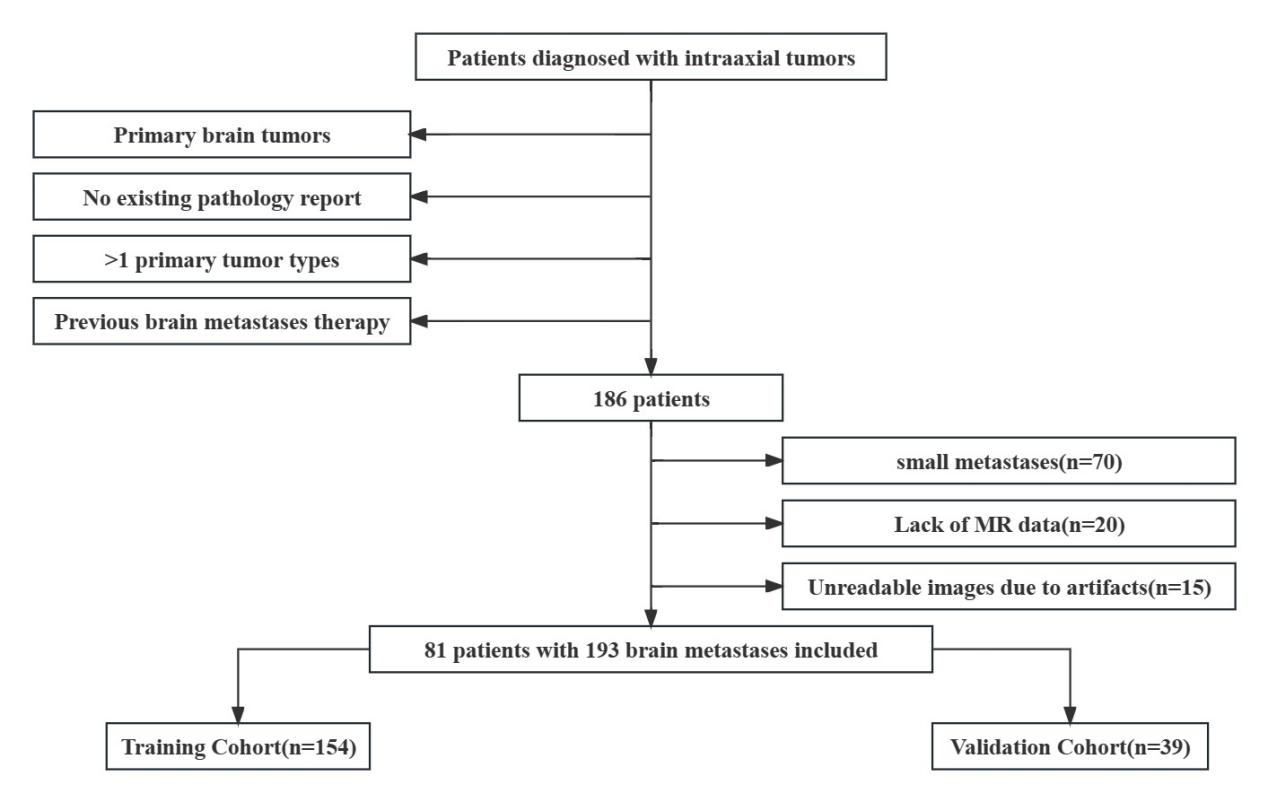
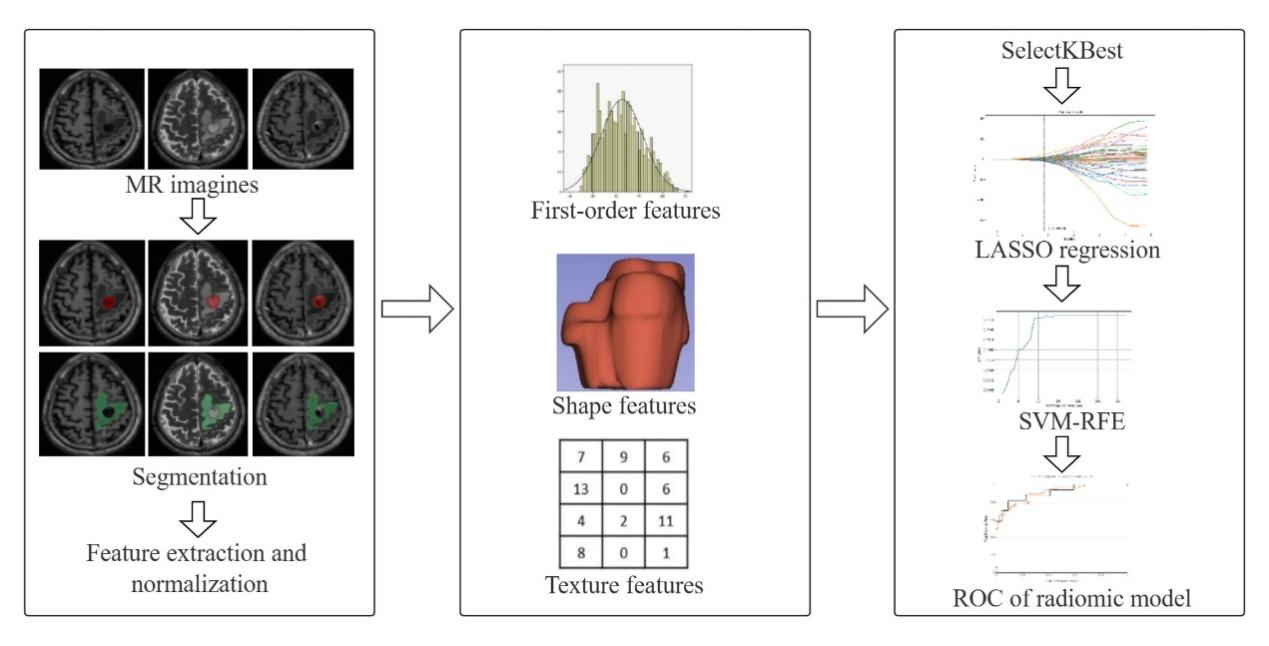
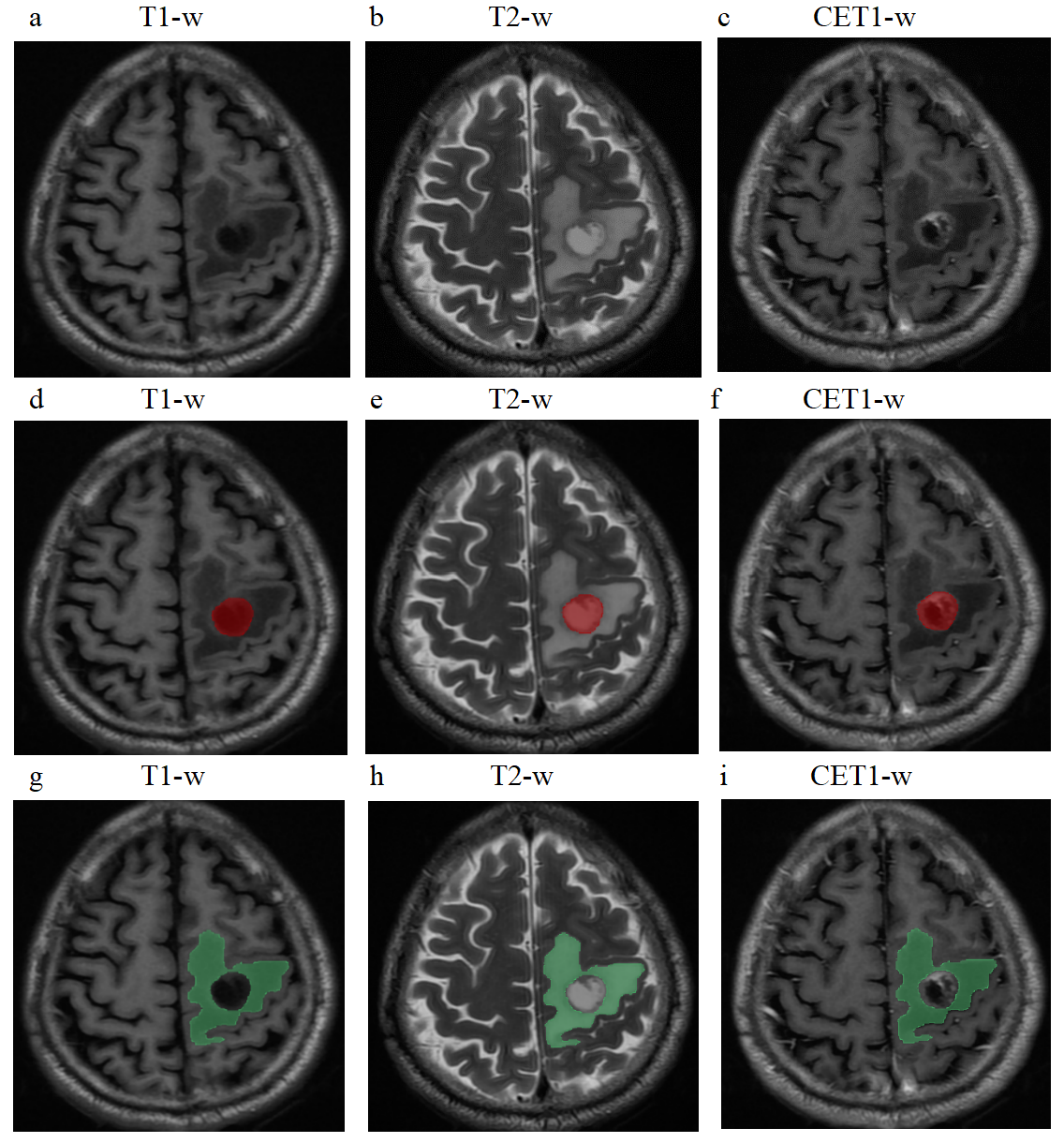
The data of patients with brain metastases from single center was collected. A total of 193 brain metastases from 81 patients were incorporated. Included metastases originated from non-small cell lung cancer (n = 110), and small cell lung cancer (n = 83). Metastases from all patients were randomly allocated to training and validation cohorts in an 8:2 ratio. The radiomics features were extracted from the peritumoral edema and tumor region of T1-weighted imaging (T1-w), T2-weighted imaging (T2-w), and contrast-enhanced T1-weighted imaging (CET1-w). Optimal radiomic feature selection was performed by SelectKBest, the least absolute shrinkage and selection operator algorithm, and support vector machine (SVM) with a recursive feature elimination algorithm. Models based on each sequence or combinations of sequences were built using a SVM classifier and used to differentiate pathological types of primary lesions of brain metastases in the training cohort and validation cohort. The area under the receiver operating characteristic curve (AUC) was used to assess the diagnostic performance of the radiomic models.Results
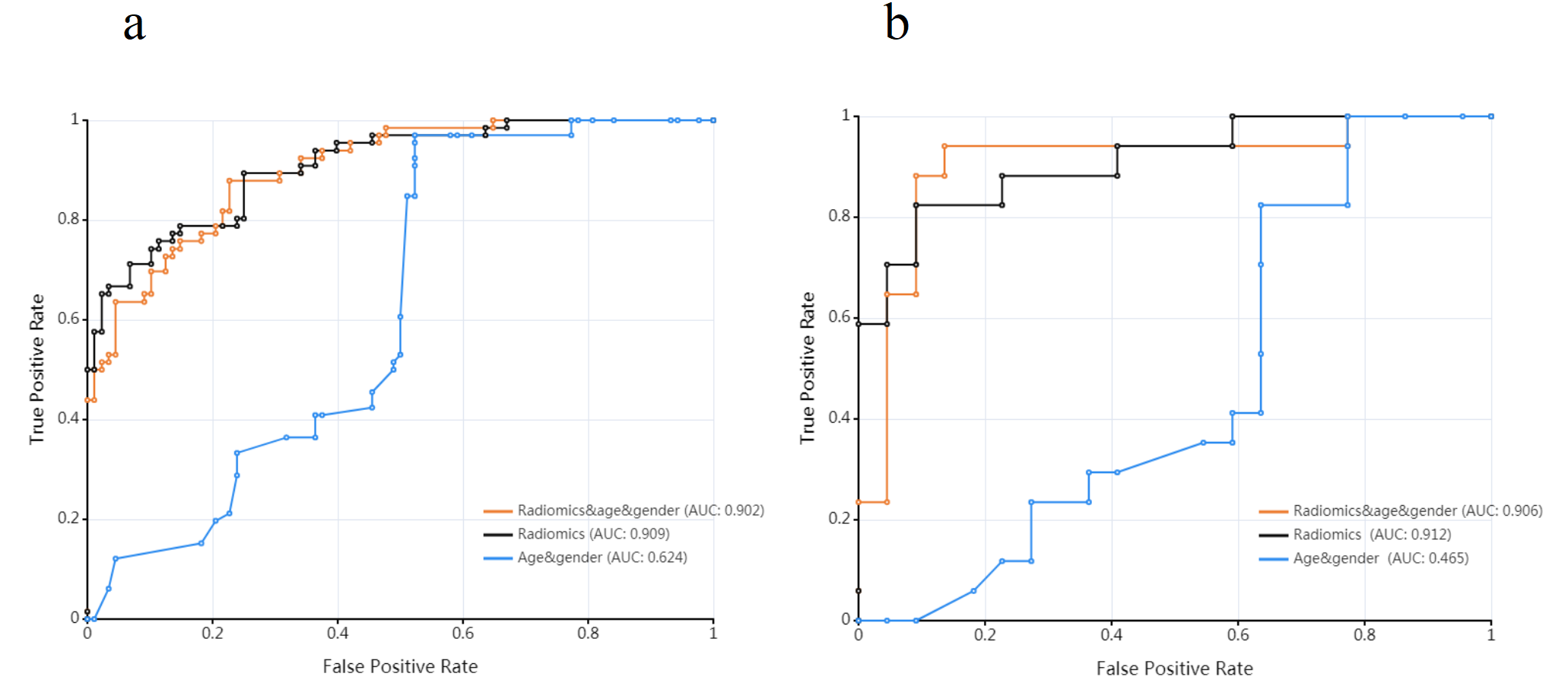
Twelve radiomic features, four from tumor region of T1-w, two from tumor region of T2-w, two from peritumoral edema of T2-w, and four from tumor region of CET1-w were selected and used to construct the best radiomic model. The AUC values of the radiomic model were 0.909 and 0.912 in the training cohort and validation cohort, respectively. The AUC values of the clinicoradiological model were 0.902 and 0.906 in the training cohort and validation cohort, respectively.Conclusions
The model based on the peritumoral edema and tumor region from T1-w, T2-w, and CET1-w has a high discriminatory ability in predicting the tumor type from different pathological types of lung cancers of brain metastases.Acknowledgements
This study was supported by Jiangxi Provincial Natural Science Foundation (grant number: 20232BAB206132).References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.214922.
2.Robnett TJ, Machtay M, Stevenson JP, Algazy KM, Hahn SM. Factors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinoma. J Clin Oncol. 2001;19(5):1344-1349. doi:10.1200/JCO.2001.19.5.13443.
3.Cooper WA, O’toole S, Boyer M, Horvath L, Mahar A. What’s new in non-small cell lung cancer for pathologists: the importance of accurate subtyping, EGFR mutations and ALK rearrangements. Pathology. 2011;43(2):103-115. doi:10.1097/PAT.0b013e328342629d
4. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71-96. doi:10.3322/CA.2007.00105.
5.Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Allen C, et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017;3(4):524-548. doi:10.1001/jamaoncol.2016.5688
6. Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022;40(5):492-516. doi:10.1200/JCO.21.02314
7. Bekaert L, Emery E, Levallet G, Lechapt-Zalcman E. Histopathologic diagnosis of brain metastases: current trends in management and future considerations. Brain Tumor Pathol. 2017;34(1):8-19. doi:10.1007/s10014-016-0275-3
8. Jiang J, Wu L, Yuan F, et al. Characterization of the immune microenvironment in brain metastases from different solid tumors. Cancer Med. 2020;9(7):2299-2308. doi:10.1002/cam4.2905
9. Mampre D, Ehresman J, Alvarado-Estrada K, et al. Propensity for different vascular distributions and cerebral edema of intraparenchymal brain metastases from different primary cancers. J Neurooncol. 2019;143(1):115-122. doi:10.1007/s11060-019-03142-x
10. Wang D, Wang ML, Li YH. Quantitative MRI study of the permeability of peritumoral brain edema in lung cancer patients with brain metastases. Brain Res. 2017;1669:126-130.doi:10.1016/j.brainres.2017.06.016
11. A Nomogram to Predict Brain Metastases of Resected Non-Small Cell Lung Cancer Patients - PubMed. Accessed October 5, 2023. https://pubmed.ncbi.nlm.nih.gov/27090794/
12. Kniep HC, Madesta F, Schneider T, et al. Radiomics of Brain MRI: Utility in Prediction of Metastatic Tumor Type. Radiology. 2019;290(2):479-487. doi:10.1148/radiol.2018180946
13. Abdel Razek AAK, Alksas A, Shehata M, et al. Clinical applications of artificial intelligence and radiomics in neuro-oncology imaging. Insights Imaging. 2021;12(1):152. doi:10.1186/s13244-021-01102-6
14. Varghese BA, Cen SY, Hwang DH, Duddalwar VA. Texture Analysis of Imaging: What Radiologists Need to Know. AJR Am J Roentgenol. 2019;212(3):520-528. doi:10.2214/AJR.18.20624
15. Deo RC. Machine Learning in Medicine. Circulation. 2015;132(20):1920-1930. doi:10.1161/CIRCULATIONAHA.115.001593
16. Choy G, Khalilzadeh O, Michalski M, et al. Current Applications and Future Impact of Machine Learning in Radiology. Radiology. 2018;288(2):318-328. doi:10.1148/radiol.2018171820
17. Kris MG, Johnson BE, Berry LD, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998-2006. doi:10.1001/jama.2014.3741
18. Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735-742. doi:10.1016/S1470-2045(11)70184-X
19. Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239-246. doi:10.1016/S1470-2045(11)70393-X
20. Wang Y, Jiang T, Qin Z, et al. HER2 exon 20 insertions in non-small-cell lung cancer are sensitive to the irreversible pan-HER receptor tyrosine kinase inhibitor pyrotinib. Ann Oncol. 2019;30(3):447-455. doi:10.1093/annonc/mdy542
21. First-Line Crizotinib versus Chemotherapy in ALK-Positive Lung Cancer. N Engl J Med. 2015;373(16):1582. doi:10.1056/NEJMx150034
22. Lambin P, Leijenaar RTH, Deist TM, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol. 2017;14(12):749-762. doi:10.1038/nrclinonc.2017.141
23. Ortiz-Ramón R, Larroza A, Ruiz-España S, Arana E, Moratal D. Classifying brain metastases by their primary site of origin using a radiomics approach based on texture analysis: a feasibility study. Eur Radiol. 2018;28(11):4514-4523. doi:10.1007/s00330-018-5463-6
24. Ortiz-Ramón R, Ruiz-España S, Mollá-Olmos E, Moratal D. Glioblastomas and brain metastases differentiation following an MRI texture analysis-based radiomics approach. Phys Med. 2020;76:44-54. doi:10.1016/j.ejmp.2020.06.016
25. Gillies RJ, Kinahan PE, Hricak H. Radiomics: Images Are More than Pictures, They Are Data. Radiology. 2016;278(2):563-577. doi:10.1148/radiol.2015151169
26. Martín-Noguerol T, Mohan S, Santos-Armentia E, Cabrera-Zubizarreta A, Luna A. Advanced MRI assessment of non-enhancing peritumoral signal abnormality in brain lesions. Eur J Radiol. 2021;143:109900. doi:10.1016/j.ejrad.2021.109900
Figures