3835
Diffusion and contrast-enhancement MRI phenotypes predict immune cell infiltration in brain metastases1Brain Tumor Imaging Laboratory (BTIL), Department of Radiological Sciences, University of California Los Angeles, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, United States, 3Division of Hematology/Oncology, Department of Medicine, University of California Los Angeles, Los Angeles, CA, United States, 4Department of Neurosurgery, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, United States, 5Department of Bioengineering, Henry Samueli School of Engineering and Applied Science, University of California Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Tumors (Post-Treatment), Treatment
Motivation: Immune checkpoint inhibitors (ICIs) can promote immune cell infiltration and increase anti-tumoral immune response in brain metastases (BM). Imaging proxies of immune infiltration would facilitate ICI-response monitoring in BM.
Goal(s): To test whether the combined assessment of diffusion and contrast-enhancement MRI phenotypes can provide insights into microscopic immune infiltration.
Approach: We studied the associations of diffusion and contrast-enhancement MRI phenotypes with histological immune cell infiltration and with ICI-treatment status
Results: Correlation analysis showed that high diffusivity and pronounced contrast-enhancement were positively associated with increased immune cell infiltration and were more likely observed in ICI-treated lesions.
Impact: Immune checkpoint inhibitors (ICIs) can promote immune cell infiltration and increase anti-tumoral immune response in brain metastases (BM). Diffusion and contrast-enhancement MRI phenotypes provide potential imaging biomarkers to non-invasively monitor tissue changes related to anti-tumoral immune response following ICIs.
Introduction
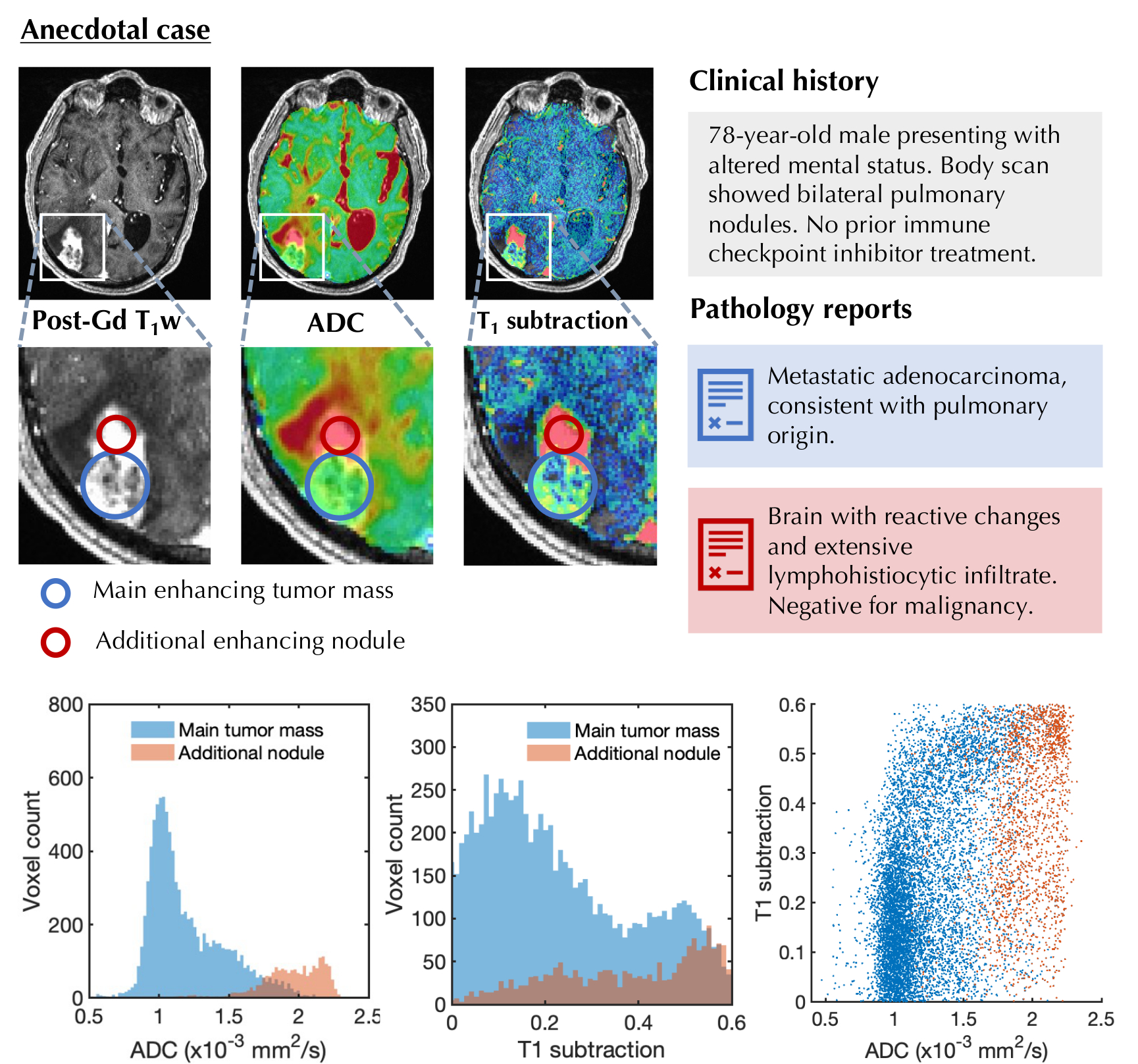
Immune checkpoint inhibitors (ICIs) are targeted therapies that promote immune cell infiltration in brain metastases (BM) [1], which potentially enhance immune response against tumor cells. Imaging biomarkers reflecting microscopic immune cell infiltration would aid in non-invasive treatment monitoring of BM patients receiving ICIs. The apparent diffusion coefficient (ADC) from diffusion MRI has been shown to detect ICI-induced microstructural changes in brain tumors [2]. Additionally, obervations in BM patients suggest that immune cell infiltration is potentially associated with higher ADC values and with more intense contrast-enhancement (CE) on T1-weighted images (Fig.1). We hypothesized that the degree of immune cell infiltration and the previous exposure to ICIs would influence diffusion and contrast-enhancement MRI phenotypes in BM.Methods
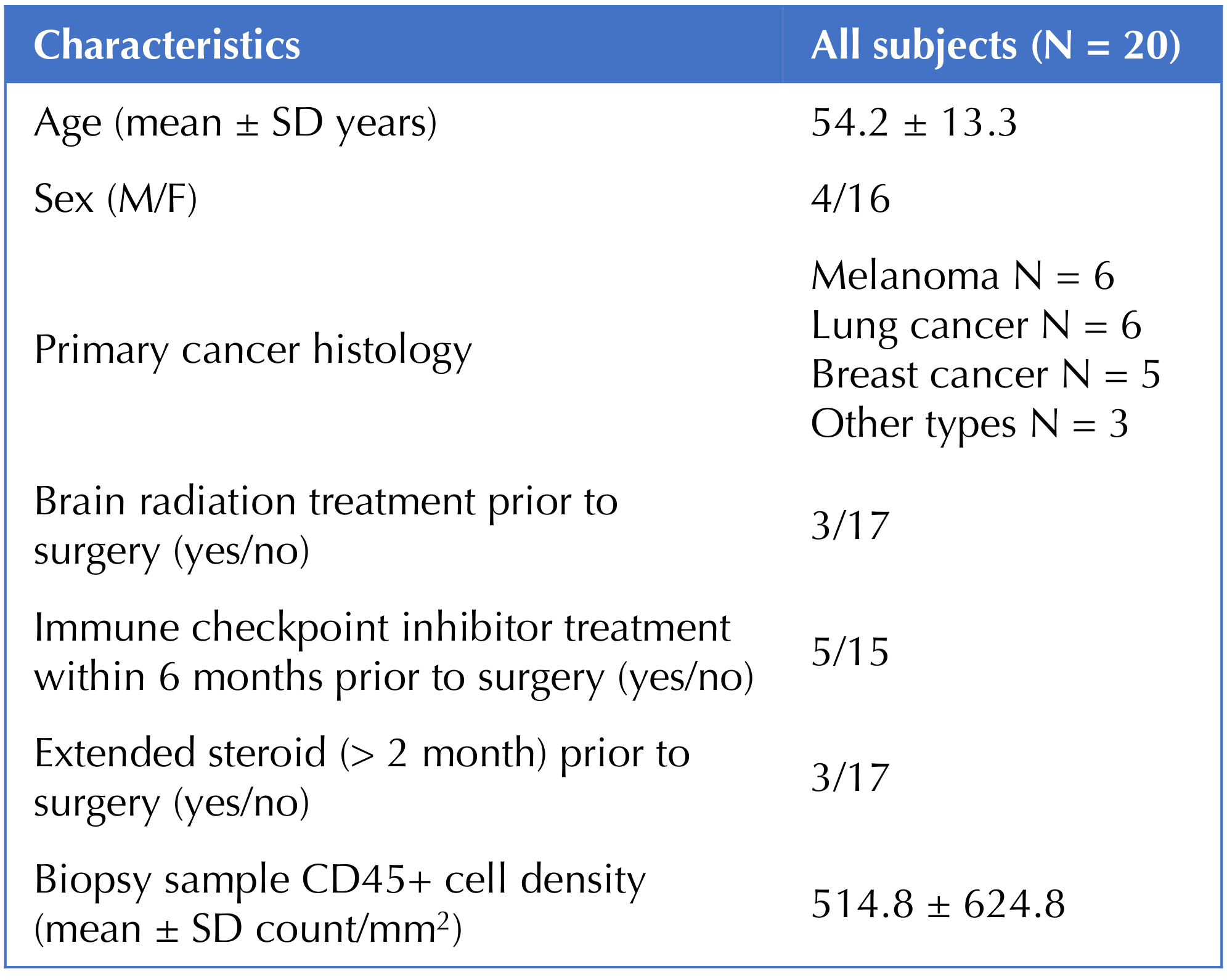
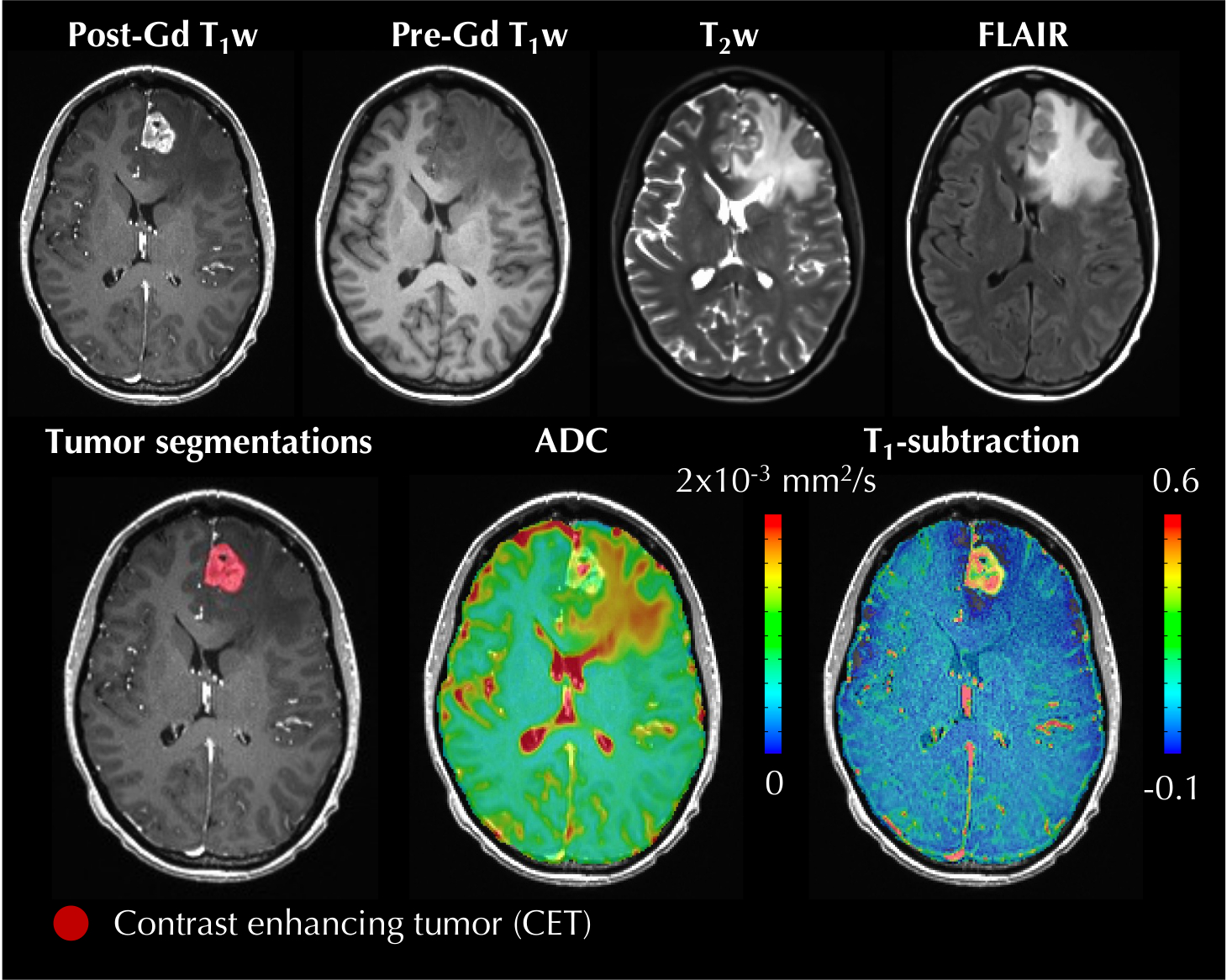
20 patients were retrospectively studied (Fig.2). Patients received preprocedural MRI scan at 1.5 (n=11) or 3.0T (n=9) including diffusion-weighted imaging and T1-weighted images, and then underwent a surgical procedure (either resection or stereotactic biopsy). ADC maps were generated from diffusion datasets on the scanner. Co-registration and signal intensity normalization were applied to pre- and post-CE T1-weighted images, then a voxel-wise subtraction was performed in order to obtain T1-subtraction maps (T1sub) [3]. T1sub provide a semi-quantitative measurement of CE, where non-enhancing voxels display negative values, while enhancing voxels display positive values proportional to the degree of enhancement (Fig.3). The contrast-enhancing tumor (CET) was segmented (Fig.3). Combined histograms representing frequency distributions for ADC and T1sub values within CET were evaluated through heatmaps to visualize diffusion and contrast-enhancement phenotypes.The tumor tissue collected during the surgical procedure was processed with histopathological staining of CD45 for immune cell quantification, and an immune infiltration measure was obtained by quantifying the density of CD45+ cells in the tissue.
For each bin in the combined histograms, the correlation between the bin-specific frequency and the histology-derived immune cell count across patients was tested using Spearman’s correlations. The resulting coefficients (ρ) and p-values for each bin were visually evaluated with heatmaps, and used to empirically determine thresholds that would optimally separate the clusters with positive and negative correlations. We tested the association between the identified diffusion and enhancement phenotypes (highADC-highCE and lowADC-lowCE) and the immune cell density using partial Spearman’s correlation (using prior steroid administration and radiation as covariates). Additionally, the imaging phenotypes were correlated with ICI-treatment status (ICI-naïve vs ICI-treated) and immune infiltration extent (high- vs low-CD45 tumors, based on a median cutoff of 281.69 CD45+ count/mm2) using Mann-Whitney U-test.
Results
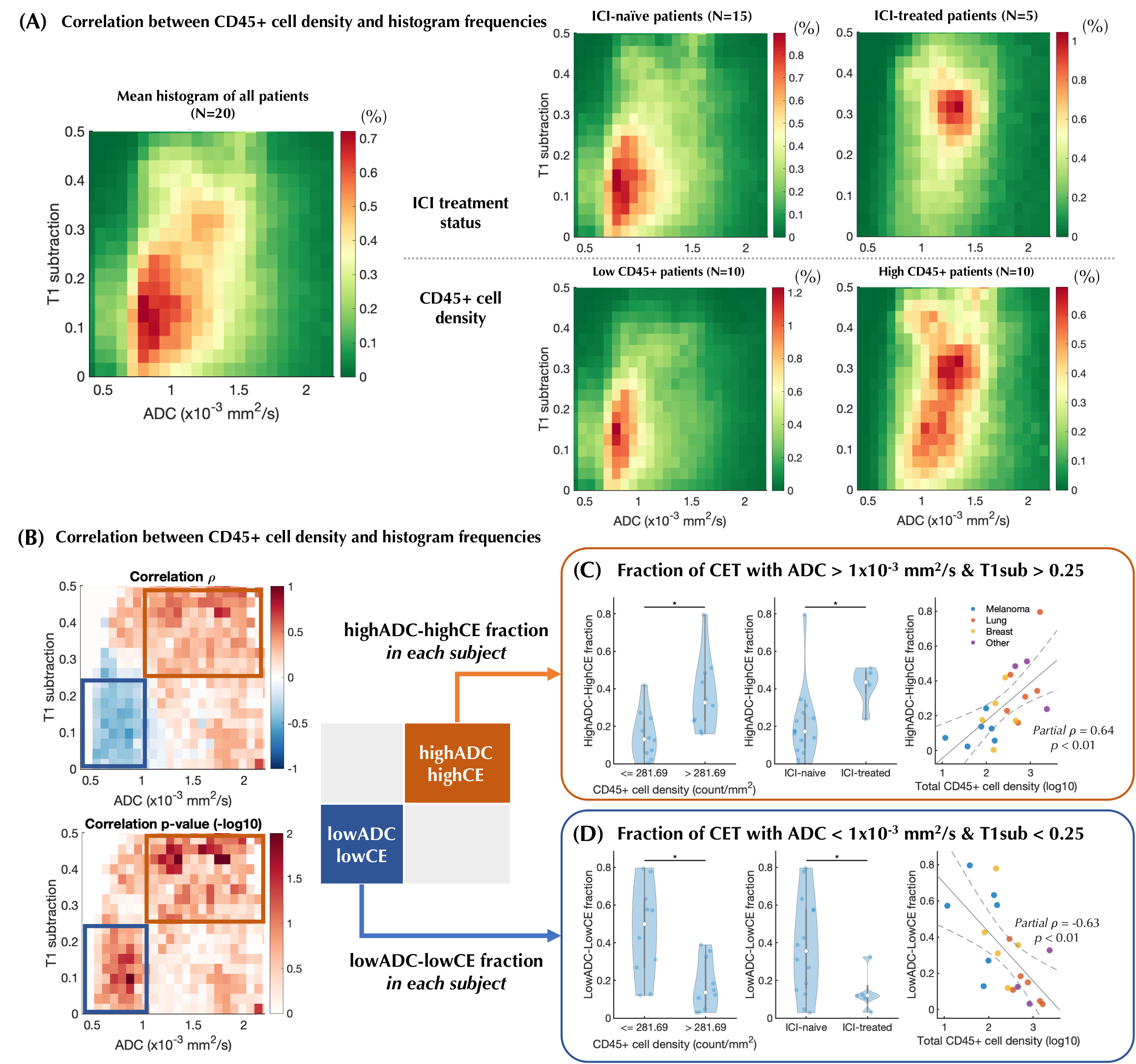
ICI-treated BM tended to show higher immune cell density than ICI-naïve BM (852.94±868.84 vs. 402.15±509.55 count/mm2, p=0.10).The mean ADC-T1sub histograms from all patients visually showed two clusters: one lowADC-lowCE (centered around 0.8x10-3 mm2/s of ADC and 0.12 of T1sub) and one highADC-highCE (centered around 1.4x10-3 mm2/s of ADC and 0.3 of T1sub) (Fig.4A, left). Cohort averaged histograms within subgroups revealed that the lowADC-lowCE cluster is mainly represented in the ICI-naïve patients and/or in the low immune cell density patients, while the highADC-highCE in the ICI-treated patients and/or in the high immune cell density patients (Fig.4A, right).
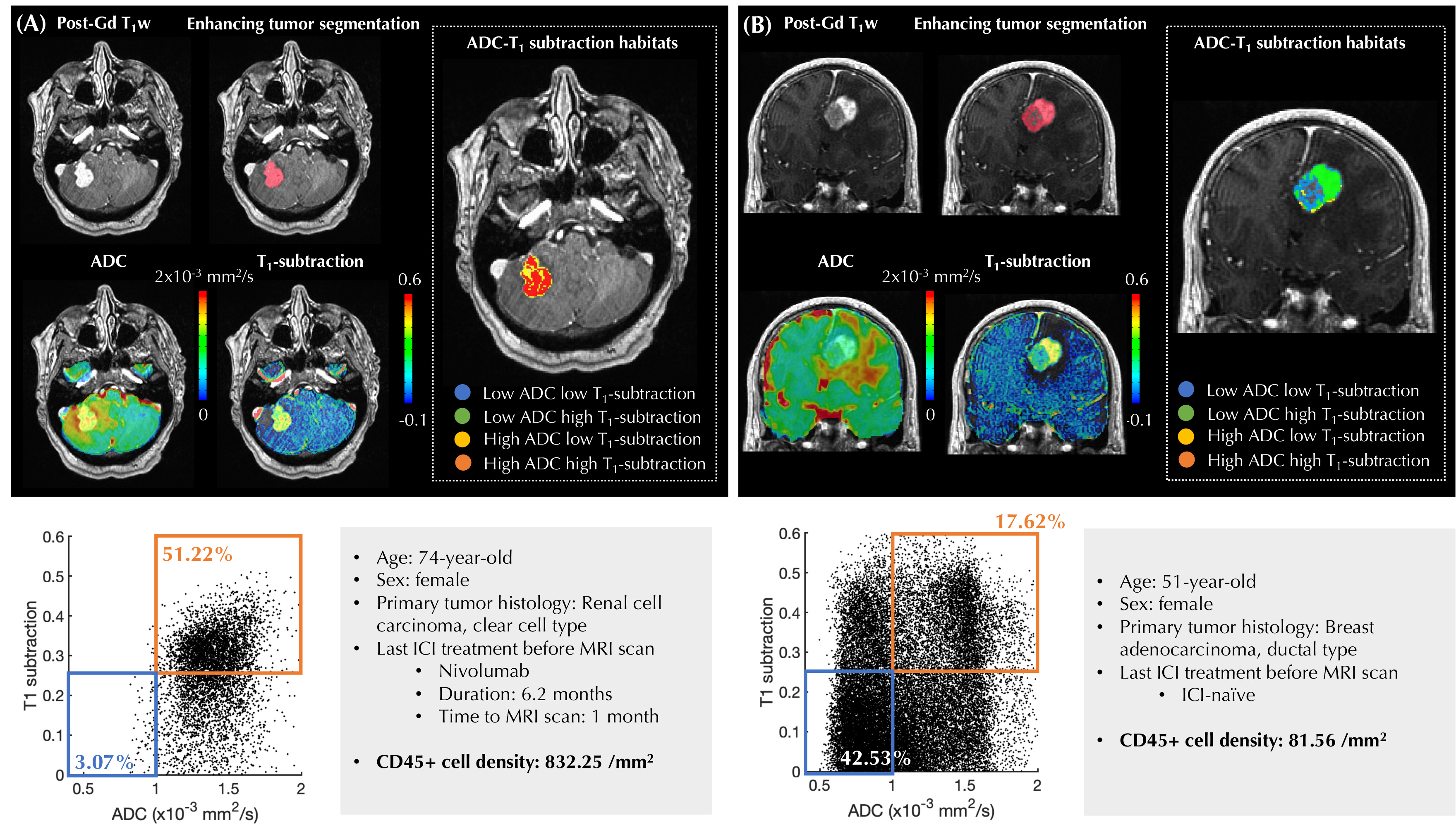
The heatmaps representing the correlations between the bin-specific frequencies and the immune cell density showed that highADC-highCE voxels were positively correlated with immune cell density, while the lowADC-lowCE voxels had a negative correlation (Fig.4B). Empiric thresholds of ADC=1.0x10-3 mm2/s and T1sub=0.25 were chosen to separate clusters with positive and negative correlations. ICI-treated BM had a higher fraction of highADC-highCE tumor compared to ICI-naïve BM (p<0.05 Fig.4C), as well as lower fraction of lowADC-lowCE tumor (p<0.05, Fig.4D). Similarly, BM with higher immune cell density had a higher fraction of highADC-highCE compared to BM with low immune cell density (p<0.05, Fig.4C), and vice versa (p<0.05, Fig.4D). Additionally, immune cell density positively correlated with the fraction of highADC-highCE voxels within CET (p<0.01, ρ=0.64, Fig.4C) and negatively correlated with the fraction of lowADC-lowCE (p<0.01, ρ=–0.63, Fig.4D). Fig.5 displays two representative cases with distinct ADC-CE phenotypes associated with different immune infiltration profiles and ICI-treatment status.
Discussion
Our results suggest that lesions with more predominant immune cell infiltration and/or previously exposed to ICI treatment show predominant highADC-highCE subregions, and smaller lowADC-lowCE subregions. This result is in line with previous studies on glioblastoma showing that ADC increase following ICIs was linked to a better prognosis, possibly due to a more pronounced anti-tumoral immune response [2].Conclusion
Immune cell infiltration in BM is associated with distinct diffusion and contrast-enhancement MRI phenotypes. Diffusion and contrast-enhancement imaging phenotypes can be useful to non-invasively monitor tissue changes related to anti-tumoral immune response following ICIs.Acknowledgements
No acknowledgement found.References
1. Sun L, Kienzler JC, Reynoso JG, et al. Immune checkpoint blockade induces distinct alterations in the microenvironments of primary and metastatic brain tumors. J Clin Invest 2023;133.2.
2. Hagiwara A, Oughourlian TC, Cho NS, et al. Diffusion MRI is an early biomarker of overall survival benefit in IDH wild-type recurrent glioblastoma treated with immune checkpoint inhibitors. Neuro Oncol 2022;24:1020–8.3.
3. Ellingson BM, Kim HJ, Woodworth DC, et al. Recurrent glioblastoma treated with bevacizumab: contrast-enhanced T1-weighted subtraction maps improve tumor delineation and aid prediction of survival in a multicenter clinical trial. Radiology 2014;271:200–10.
Figures