3834
Comparing non-invasive blood-brain barrier mapping with dynamic susceptibility contrast MRI in patients with high-grade glioma and metastasis1School of Medicine and Health, Department of Neuroradiology, Technical University of Munich, Munich, Germany, 2School of Medicine and Health, TUM-Neuroimaging Center, Technical University of Munich, Munich, Germany, 3School of Medicine and Health, Clinic of Neurology, Technical University of Munich, Munich, Germany, 4MR Physics, Fraunhofer Institute for Digital Medicine MEVIS, Bremen, Germany, 5MR-Imaging and Spectroscopy, University of Bremen, Bremen, Germany, 6mediri GmbH, Heidelberg, Germany, 7C.J. Gorter MRI Center, Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 8Leiden Institute of Brain and Cognition, Leiden University, Leiden, Netherlands, 9Philips GmbH Market DACH, Hamburg, Germany
Synopsis
Keywords: Tumors (Post-Treatment), Permeability, Blood Brain Barrier
Motivation: Glioma-induced blood-brain barrier (BBB) disruptions can be characterized by dynamic susceptibility contrast MRI via the leakage parameter K2. However, it may lack sensitivity to subtle impairments. Recently, non-invasive ASL-based water-exchange measurements (Tex) were proposed to measure even subtle BBB-impairments.
Goal(s): We hypothesized correlations of Tex with K2 in contrast-enhancing tissue (CET).
Approach: K2 & Tex were compared in 22 patients with brain tumors and 19 healthy controls.
Results: Tex agreed well with K2 in CET and was sensitive to pathophysiologically impaired BBB. Moreover, results indicate superior sensitivity to subtle impairments, which may improve therapy planning and progress monitoring.
Impact: ASL-based Tex allows non-invasive detection of the pathophysiologically impaired blood-brain barrier in tumors. Whereas its sensitivity to subtle impairments may improve treatment planning in tumors, it could also impact diagnosis of neurodegenerative diseases such as Alzheimer's or Parkinson’s.
Introduction
The blood-brain barrier (BBB) is a robust barrier hindering potentially harmful substances from leaking into the brain. Severe BBB damage in high-grade brain tumors is well-known.1-3 Clinically used contrast agent (CA) enhanced T1-weighted MRI allows qualitative analyses, but suffers from limited sensitivity due to comparably large Gadolinium (Gd) compounds. Quantitative information can be obtained by the dynamic susceptibility contrast (DSC) MRI-based leakage parameter K2.4-6 Generally K2 describes two effects: K2>0 represents a dominant T1-shortening and K2<0 relates to T2*-effects from susceptibility differences between intra- and extravascular space. Higher |K2| is associated with increased leakage.6,7 While correlations of K2 with ktrans from dynamic contrast enhanced (DCE) MRI and tumor grade were reported,7-10 sensitivity to subtle impairments is debated.11 Gd is also contraindicated in subjects with renal malfunction.12-15Using water as a freely diffusible tracer, we16 recently proposed non-invasive BBB mapping, which is expected to be sensitive to even subtle impairments.17-19 Based on Hadamard-encoded20,21 multi-echo (multi-TE) arterial spin labeling (ASL) data, an extended T2-based two-compartment model is applied and water exchange times Tex are calculated.16,22 Hypothesizing that reduced Tex indicates BBB impairment, we recently reported shorter Tex in tumorous tissue.23 However, validation with an independent measure is lacking.
The aim of this work is therefore to evaluate correlations between CA-based K2 and ASL-based Tex in tumors. We hypothesize that in areas with impaired BBB, reduced Tex correlates with increased K2. Additionally, we evaluated normal-appearing (NA) tissue for potential impairments.
Methods
MRI-data of 24 patients (68.5±12.8y,10f) with relapsed intra-axial, high-grade glioma (n=12) and metastases (n=12) were compared with 19 age-matched healthy controls (HCs,64±14.8y,14f). A 3T Elition Ingenia X was used (Philips,Best,Netherlands). Three subjects were excluded due to incomplete data acquisition or incidental findings. The imaging protocol included standard diagnostic imaging (CA-enhanced T1w&FLAIR), DSC for K2,4,6 and ASL-BBB for Tex16 (Fig.1). Anatomical images were co-registered, skull-stripped, and segmented into masks of CA-enhancing tissue (CET) and edema using an ensemble classifier (BraTS Toolkit).24 Segments of normal-appearing grey matter (NAGM) and NAWM, were calculated using ANTs Atropos.25 Analyses used Matlab (v2021b,TheMathWorksInc.,Natick,USA) and SPM12.26 For CET, VOIs larger than 3cm³ were evaluated (n=7). Pearson-Correlations of Tex with K2>0, K2<0 and |K2| were calculated. |K2| was used for regional investigations of combined T1 and T2*-effects. Lastly, Tex and |K2| were compared between patients and HCs (unpaired t-tests, p<0.05).Results
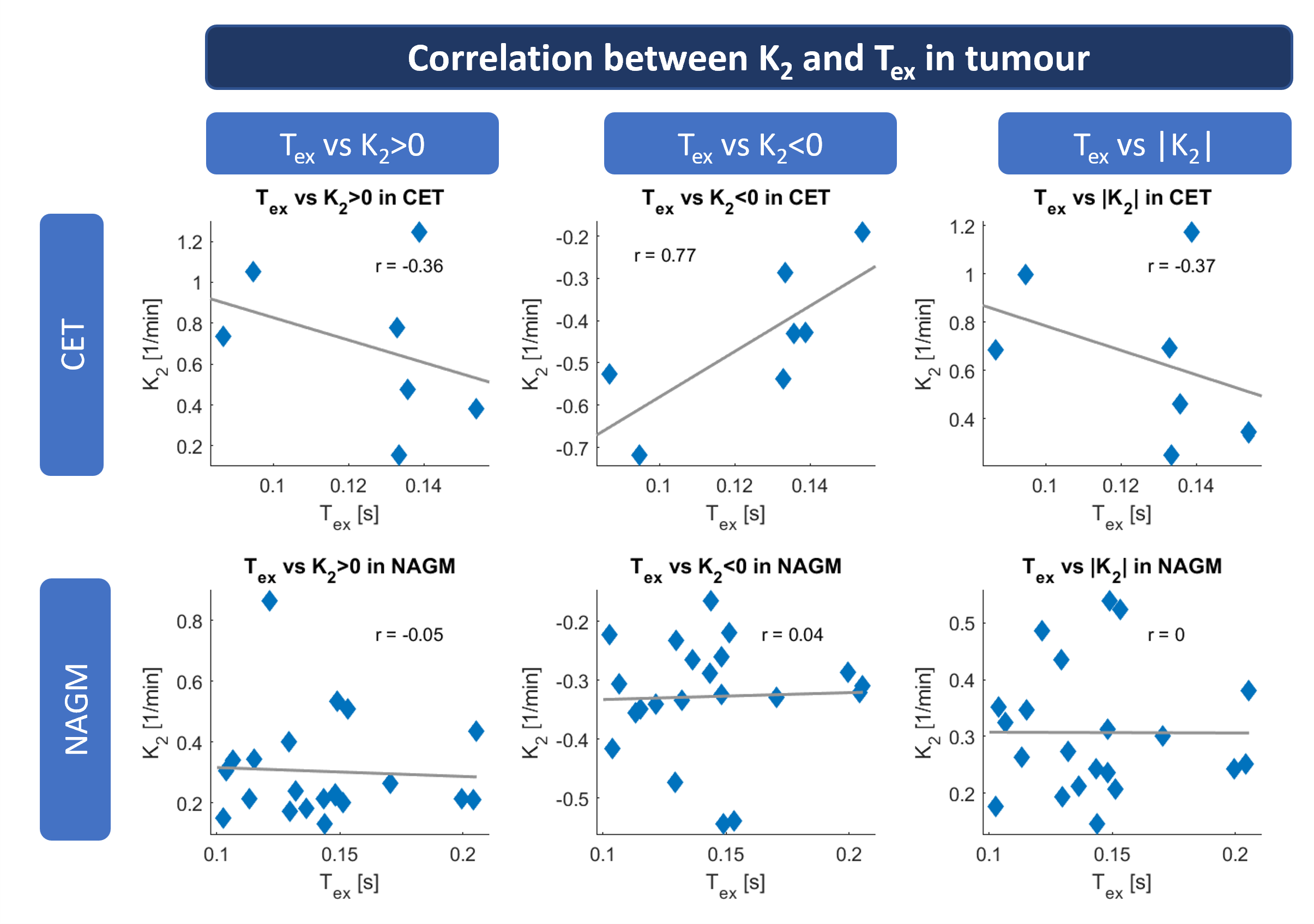
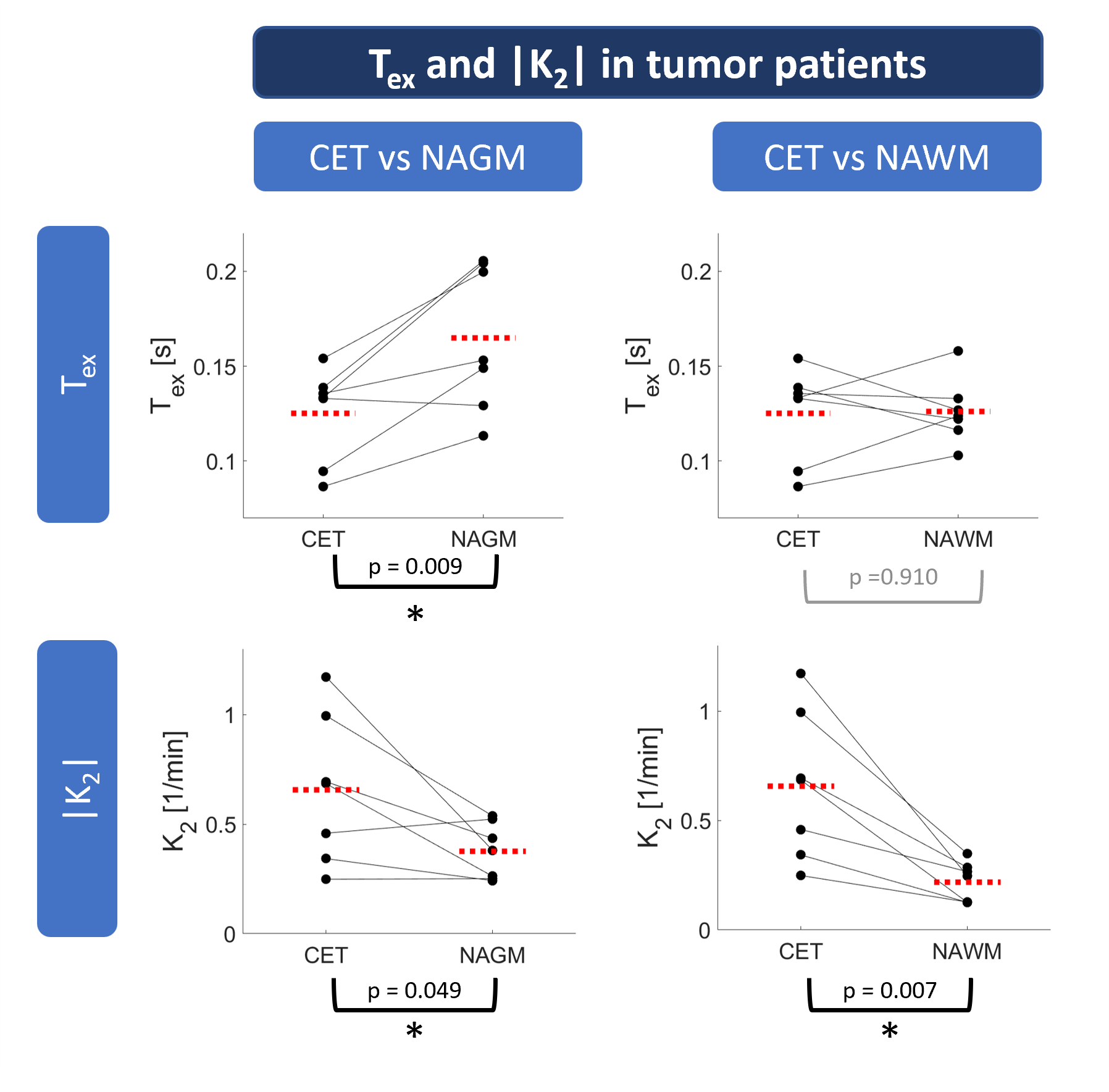
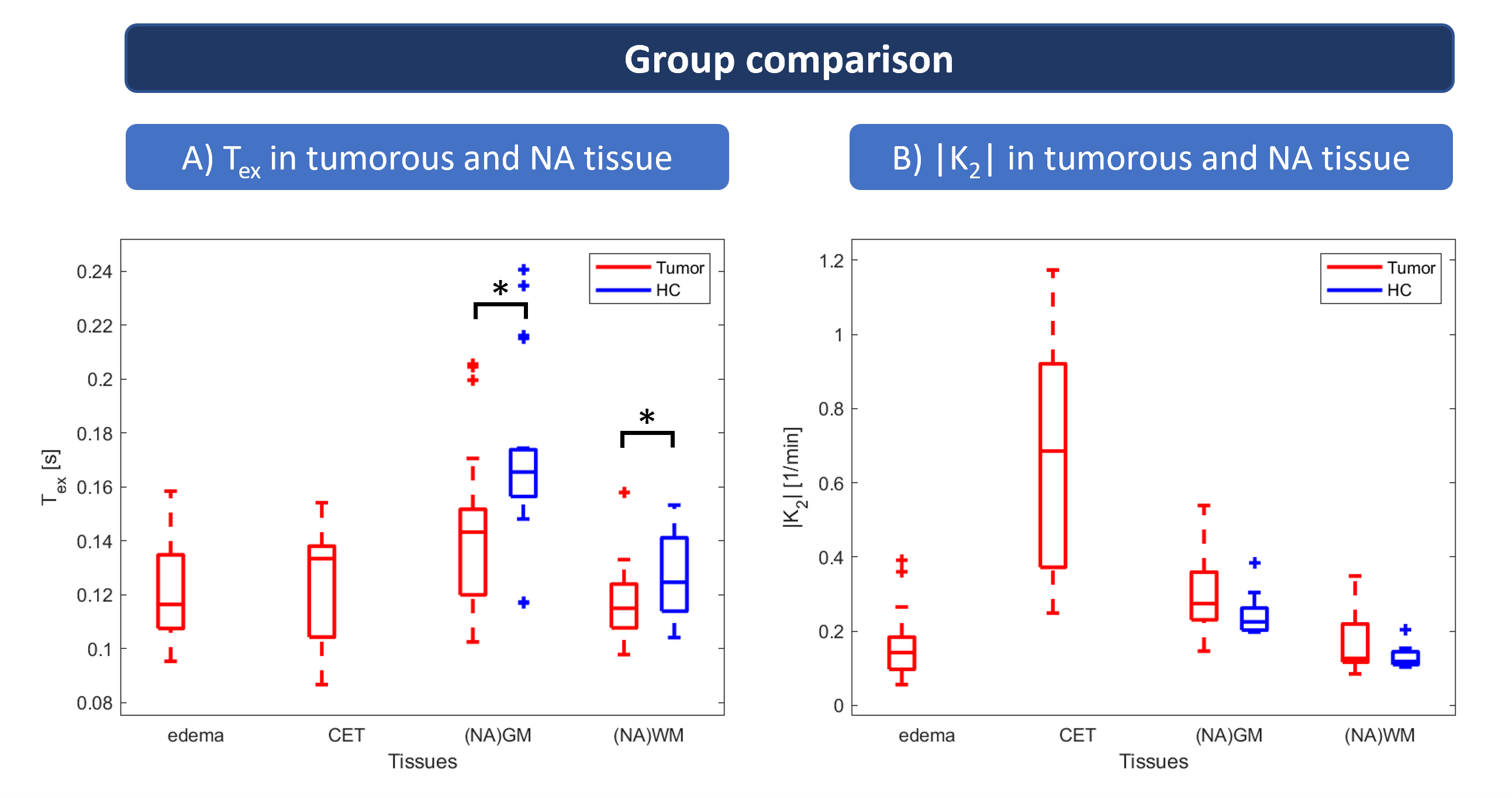
Data from a representative Glioma patient (Fig.2, 1a-e) show rim-like CA uptake (1a) and extensive edema (1b). This visually agrees with hypointense regions in Tex (1d) and increased K2 (1e), dominated by K2>0. Similar effects are seen in a metastasis patient (2a-e), however, K2-maps were dominated by K2<0 in CET (2e).On group-level, Tex correlated well with K2>0 (r=-0.36), K2<0 (r=0.77), and |K2| (r=-0.37) in CET (Fig.3,top), while correlations in NAGM were low (Fig.3, bottom). In CET, Tex was significantly reduced compared to NAGM (Fig.4,top), similar to increased |K2| in CET compared to NAGM and NAWM (Fig.4,bottom). In edema, Tex was likewise reduced, while K2 was not increased (Fig.5A). Compared to HCs, Tex was significantly reduced in (NA)GM (p=0.008) and (NA)WM (p=0.041), while |K2| was just marginally increased in patients (Fig.5B).
Discussion
As hypothesized, our results indicate that reduced Tex correlates with increased K2 in CET with impaired BBB. This agreement was found for both K2 domains (K2>0 and K<0) and |K2|. In NAGM, weak correlations of Tex with K2 reflect expectations, as very subtle CA-leakage largely reduces K2-sensitivity. Lowered Tex in CET agrees well with increased |K2| and can be interpreted as increased leakage which concords with several reports from DCE2,27 and DSC6-8 studies. Similar Tex in CET and NAWM may be due to comparably low ASL signal in NAWM, limiting Tex accuracy. Low Tex in edema may, however, indicate BBB impairments preceding CA-leakage 28,29 that are not yet detectable using |K2|. Interestingly, Tex was significantly decreased in NAGM and NAWM of patients compared to HCs, while |K2| differed just slightly between groups. This may indicate subtle BBB impairment in NA-tissue without CA-leakage, which is not detectable with K2. This agrees with expected Tex sensitivity for subtle impairments using water as an endogenous tracer.16-19 This finding might be especially relevant in tumor progression monitoring and therapy planning.30-32Conclusion
In conclusion, ASL-based Tex is sensitive to pathophysiological changes in BBB-integrity and agrees well with DSC-based K2. Moreover, decreased Tex in NAGM and NAWM points to sufficient sensitivity to subtle impairments in normal appearing tissue, which may open pathways for advanced tumor therapy management. Consequently, non-invasive Tex could also contribute to understanding of BBB dysfunction in various other pathologies such as Alzheimer’s disease.33-35Acknowledgements
We would like to acknowledge support by the Ev. Studienwerk Villigst (personal grant to GH) and by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – project number 395030489. AM and MG received funding from the European Union's Horizon 2020 Research and Innovation Programme under grant agreement No. 825664.
References
1. Jain, R.K., Di Tomaso, E., Duda, D.G., Loeffler, J.S., Sorensen, A.G. & Batchelor, T.T. Angiogenesis in brain tumours. Nature Reviews Neuroscience 8, 610-622 (2007).
2. Heye, A.K., Culling, R.D., Hernandez, M.D.V., Thrippleton, M.J. & Wardlaw, J.M. Assessment of blood-brain barrier disruption using dynamic contrast-enhanced MRI. A systematic review. Neuroimage-Clin 6, 262-274 (2014).
3. Wolburg, H., Noell, S., Fallier-Becker, P., Mack, A.F. & Wolburg-Buchholz, K. The disturbed blood–brain barrier in human glioblastoma. Molecular Aspects of Medicine 33, 579-589 (2012).
4. Boxerman, J.L., Schmainda, K.M. & Weisskoff, R.M. Relative cerebral blood volume maps corrected for contrast agent extravasation significantly correlate with glioma tumor grade, whereas uncorrected maps do not. AJNR Am J Neuroradiol 27, 859-867 (2006).
5. Bjornerud, A., Sorensen, A.G., Mouridsen, K. & Emblem, K.E. T1- and T2*-dominant extravasation correction in DSC-MRI: part I--theoretical considerations and implications for assessment of tumor hemodynamic properties. J Cereb Blood Flow Metab 31, 2041-2053 (2011).
6. Kluge, A., Lukas, M., Toth, V., Pyka, T., Zimmer, C. & Preibisch, C. Analysis of three leakage-correction methods for DSC-based measurement of relative cerebral blood volume with respect to heterogeneity in human gliomas. Magnetic resonance imaging 34, 410-421 (2016).
7. Lee, J.Y., Bjornerud, A., Park, J.E., Lee, B.E., Kim, J.H. & Kim, H.S. Permeability measurement using dynamic susceptibility contrast magnetic resonance imaging enhances differential diagnosis of primary central nervous system lymphoma from glioblastoma. Eur Radiol 29, 5539-5548 (2019).
8. Bonekamp, D., Deike, K., Wiestler, B., Wick, W., Bendszus, M., Radbruch, A. & Heiland, S. Association of overall survival in patients with newly diagnosed glioblastoma with contrast-enhanced perfusion MRI: Comparison of intraindividually matched T1 - and T2 (*) -based bolus techniques. Journal of Magnetic Resonance Imaging 42, 87-96 (2015).
9. Taoka, T., Kawai, H., Nakane, T., Hori, S., Ochi, T., Miyasaka, T., Sakamoto, M., Kichikawa, K. & Naganawa, S. Application of histogram analysis for the evaluation of vascular permeability in glioma by the K2 parameter obtained with the dynamic susceptibility contrast method: Comparisons with Ktrans obtained with the dynamic contrast enhance method and cerebral blood volume. Magnetic Resonance Imaging 34, 896-901 (2016).
10. Quarles, C.C., Gore, J.C., Xu, L. & Yankeelov, T.E. Comparison of dual-echo DSC-MRI- and DCE-MRI-derived contrast agent kinetic parameters. Magn Reson Imaging 30, 944-953 (2012).
11. Elschot, E.P., Backes, W.H., de Jong, J.J.A., Drenthen, G.S., Wong, S.M., Staals, J., Postma, A.A., Rouhl, R.P.W., van Oostenbrugge, R.J. & Jansen, J.F.A. Assessment of the clinical feasibility of detecting subtle blood-brain barrier leakage in cerebral small vessel disease using dynamic susceptibility contrast MRI. Magn Reson Imaging 102, 55-61 (2023).
12. European Medicines Agency (EMA). EMA's final opinion confirms restrictions on use of linear gadolinium agents in body scans. (2017).
13. Harvey, H.B., Gowda, V. & Cheng, G. Gadolinium deposition disease: a new risk management threat. Journal of the American College of Radiology 17, 546-550 (2020).
14. Marckmann, P., Skov, L., Rossen, K., Dupont, A., Damholt, M.B., Heaf, J.G. & Thomsen, H.S. Nephrogenic systemic fibrosis: suspected causative role of gadodiamide used for contrast-enhanced magnetic resonance imaging. Journal of the American Society of Nephrology 17, 2359-2362 (2006).
15. Semelka, R.C., Ramalho, J., Vakharia, A., AlObaidy, M., Burke, L.M., Jay, M. & Ramalho, M. Gadolinium deposition disease: initial description of a disease that has been around for a while. Magnetic resonance imaging 34, 1383-1390 (2016).
16. Mahroo, A., Buck, M.A., Huber, J., Breutigam, N.J., Mutsaerts, H., Craig, M., Chappell, M. & Gunther, M. Robust Multi-TE ASL-Based Blood-Brain Barrier Integrity Measurements. Front Neurosci 15, 719676 (2021).
17. Dickie, B.R., Parker, G.J.M. & Parkes, L.M. Measuring water exchange across the blood-brain barrier using MRI. Prog Nucl Magn Reson Spectrosc 116, 19-39 (2020).
18. Petitclerc, L., Schmid, S., Hirschler, L. & van Osch, M.J.P. Combining T2 measurements and crusher gradients into a single ASL sequence for comparison of the measurement of water transport across the blood–brain barrier. Magnetic Resonance in Medicine 85, 2649-2660 (2021).
19. Shao, X., Jann, K., Ma, S.J., Yan, L., Montagne, A., Ringman, J.M., Zlokovic, B.V. & Wang, D.J.J. Comparison Between Blood-Brain Barrier Water Exchange Rate and Permeability to Gadolinium-Based Contrast Agent in an Elderly Cohort. Frontiers in Neuroscience 14(2020).
20. Günther, M. Highly efficient accelerated acquisition of perfusion inflow series by cycled arterial spin labeling. in Proceedings of the 15th Annual Meeting of ISMRM (Berlin, 2007).
21. van Osch, M.J., Teeuwisse, W.M., Chen, Z., Suzuki, Y., Helle, M. & Schmid, S. Advances in arterial spin labelling MRI methods for measuring perfusion and collateral flow. Journal of Cerebral Blood Flow & Metabolism 38, 1461-1480 (2018).
22. Mahroo, A., Buck, M.A. & Günther, M. Increased Permeability of Blood-Brain Barrier in the Aging Human Brain – A Multi-TE ASL Study. ISMRM Perfusion Workshop - From Head to Toe, (Los Angeles, CA, United States, March 04-07, 2022).
23. Hoffmann, G., Preibisch, C., Günther, M., Mahroo, A., van Osch, M., Václavů, L., Schmitzer, L., Zimmer, C., Wiestler, B. & Kaczmarz, S. Non-invasive blood brain barrier integrity mapping in patients with high-grade glioma and metastasis by time-encoded arterial spin labelling. in Proceedings of the International Society of Magnetic Resonance in Medicine (Toronto, 2023).
24. Kofler, F., Berger, C., Waldmannstetter, D., Lipkova, J., Ezhov, I., Tetteh, G., Kirschke, J., Zimmer, C., Wiestler, B. & Menze, B.H. BraTS toolkit: translating BraTS brain tumor segmentation algorithms into clinical and scientific practice. Frontiers in neuroscience, 125 (2020).
25. Avants, B.B., Tustison, N.J., Wu, J., Cook, P.A. & Gee, J.C. An open source multivariate framework for n-tissue segmentation with evaluation on public data. Neuroinformatics 9, 381-400 (2011).
26. Wellcome Centre for Human Neuroimaging. Statistical Parametric Mapping Software (SPM 12).
27. Keil, V.C., Gielen, G.H., Pintea, B., Baumgarten, P., Datsi, A., Hittatiya, K., Simon, M. & Hattingen, E. DCE-MRI in glioma, infiltration zone and healthy brain to assess angiogenesis: a biopsy study. Clinical neuroradiology 31, 1049-1058 (2021).
28. Gumerlock, M.K., Belshe, B.D., Madsen, R. & Watts, C. Osmotic blood-brain barrier disruption and chemotherapy in the treatment of high grade malignant glioma: patient series and literature review. Journal of Neuro-Oncology 12, 33-46 (1992).
29. Lutz, K., Wiestler, B., Graf, M., Bäumer, P., Floca, R., Schlemmer, H.-P., Heiland, S., Wick, W., Bendszus, M. & Radbruch, A. Infiltrative patterns of glioblastoma: Identification of tumor progress using apparent diffusion coefficient histograms. Journal of Magnetic Resonance Imaging 39, 1096-1103 (2014).
30. Dubois, L.G., Campanati, L., Righy, C., D'Andrea-Meira, I., Spohr, T.C., Porto-Carreiro, I., Pereira, C.M., Balca-Silva, J., Kahn, S.A., DosSantos, M.F., Oliveira Mde, A., Ximenes-da-Silva, A., Lopes, M.C., Faveret, E., Gasparetto, E.L. & Moura-Neto, V. Gliomas and the vascular fragility of the blood brain barrier. Front Cell Neurosci 8, 418 (2014).
31. Agarwal, S., Sane, R., Oberoi, R., Ohlfest, J.R. & Elmquist, W.F. Delivery of molecularly targeted therapy to malignant glioma, a disease of the whole brain. Expert reviews in molecular medicine 13(2011).
32. Sarkaria, J.N., Hu, L.S., Parney, I.F., Pafundi, D.H., Brinkmann, D.H., Laack, N.N., Giannini, C., Burns, T.C., Kizilbash, S.H. & Laramy, J.K. Is the blood–brain barrier really disrupted in all glioblastomas? A critical assessment of existing clinical data. Neuro-oncology 20, 184-191 (2018).
33. van de Haar, H.J., Burgmans, S., Jansen, J.F., van Osch, M.J., van Buchem, M.A., Muller, M., Hofman, P.A., Verhey, F.R. & Backes, W.H. Blood-Brain Barrier Leakage in Patients with Early Alzheimer Disease. Radiology 281, 527-535 (2016).
34. Starr, J.M., Farrall, A.J., Armitage, P., McGurn, B. & Wardlaw, J. Blood-brain barrier permeability in Alzheimer's disease: a case-control MRI study. Psychiatry Res 171, 232-241 (2009).
35. Al-Bachari, S., Naish, J.H., Parker, G.J.M., Emsley, H.C.A. & Parkes, L.M. Blood–Brain Barrier Leakage Is Increased in Parkinson’s Disease. Frontiers in Physiology 11(2020).Figures
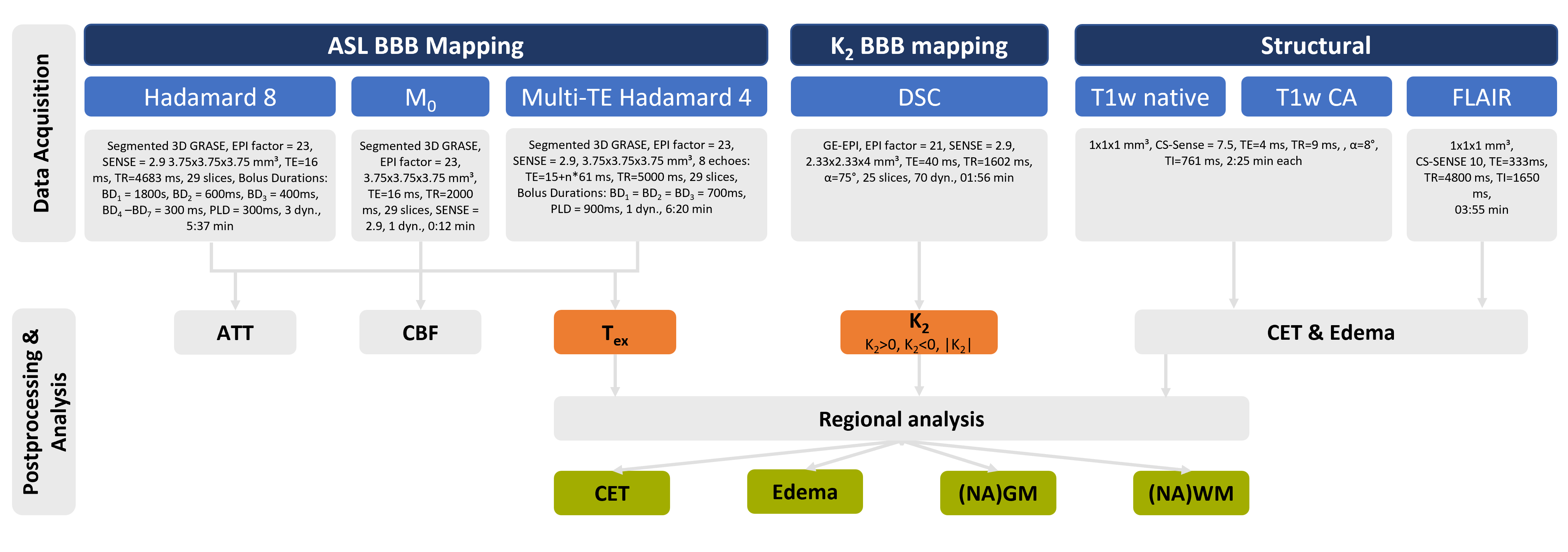
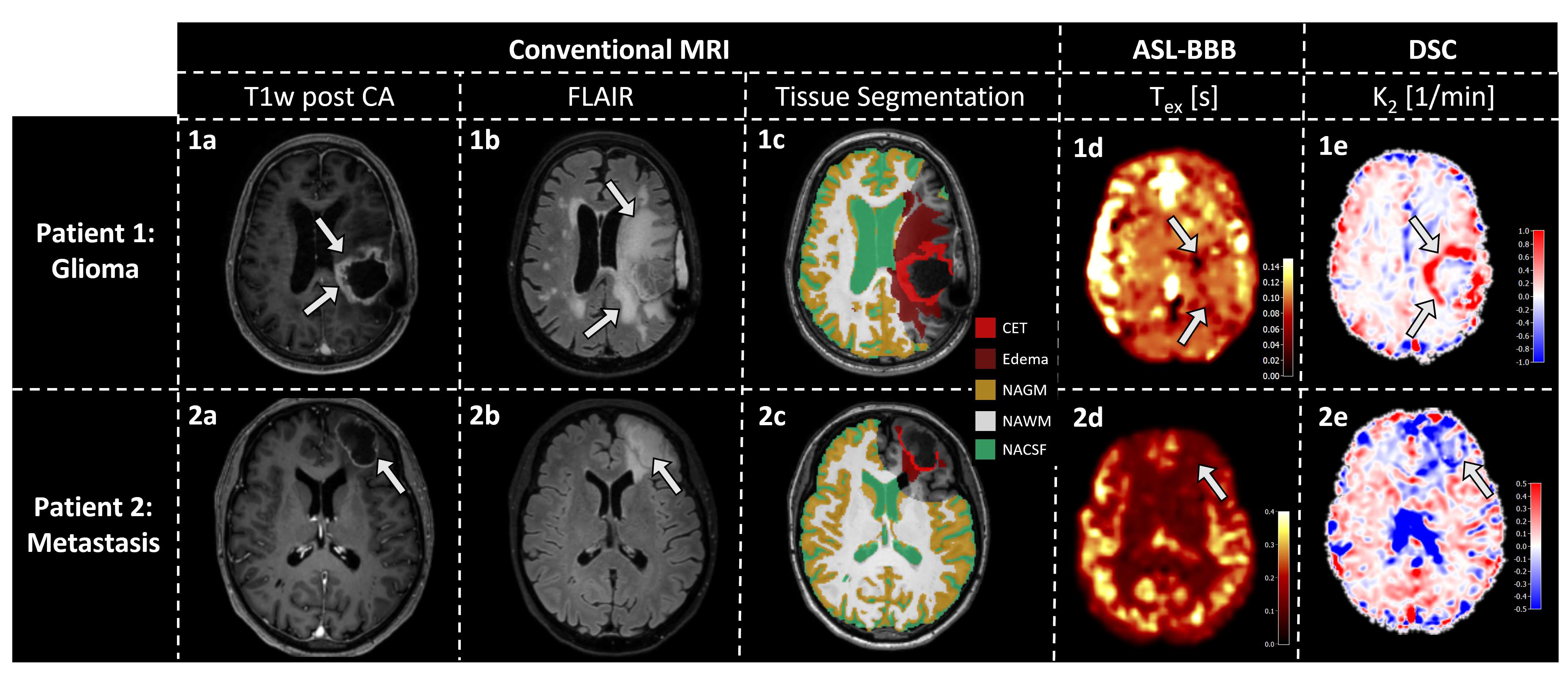
Figure 2: Exemplary data of two patients. T1w post contrast agent (CA, a), FLAIR (b), tissue masks (c), Tex (d) and K2 (e) maps are shown. The glioma patients’ rim-like CA uptake (1a) and pronounced edema (1b) are segmented into masks of contrast enhancing tissue (CET) and edema (1c). Tex (1d) is visibly reduced in the tumorous region, resembling areas of increased K2, dominated by K2>0. The metastasis patient similarly shows a rim like CA uptake (2a) with edema (2b). Here, hypointense Tex regions (2d) concord with areas where K2 < 0 (2e). Arrows indicate tumorous regions.