3820
An interleaved flip angle multi-slice acquisition method for 2D variable flip angle T1 mapping1State Key Laboratory of Extreme Photonics and Instrumentation, College of Optical Science and Engineering, Zhejiang University, Hangzhou, China
Synopsis
Keywords: Quantitative Imaging, Quantitative Imaging
Motivation: Magnetization transfer (MT) effect has been demonstrated to be a significant factor that results in the estimation bias and reduced reproducibility of single pool T1 mapping by 3D variable flip angle (VFA) method.
Goal(s): Reduce the estimation bias of 2D VFA T1 mapping method while improving its reproducibility using different protocols with a simple single-pool relaxometry model.
Approach: Interleave the variable flip angles for multi-slice 2D acquisition to balance the MT effect between acquisitions without SAR increase.
Results: Both simulations and in vivo experiments showed improved accuracy and reproducibility of 2D VFA T1 mapping with our proposed method.
Impact: It has been reported that 2D VFA T1 mapping encounters biased estimation and low reproducibility issues. Improving estimation accuracy and reducing estimation variance can help promote the clinical application of 2D VFA T1 mapping.
Introduction
As a fast T1 mapping method, variable flip angle (VFA) is widely used in basic and clinical research. While VFA with a single pool relaxometry model shows unreliable parameter estimates because of MT effects, controlled saturation magnetization transfer (CSMT)1 has been proposed for 3D VFA acquisition to alleviate this issue and is found to highly improve the reproducibility of T1 mapping across vendors2. In CSMT, multiband nonselective RF pulses are used, and different amplitudes of off-resonance RF are added to different flip angles of on-resonance RF to balance the energy between different acquisitions, thus inevitably increasing the RF power and making it easy to excess SAR limits.Here we proposed an interleaved flip angle multi-slice acquisition method (IFAMS) for 2D VFA T1 mapping to balance the MT effect between different acquisitions without increasing the RF power, and thus improve the accuracy of 2D T1 mapping and reproducibility under different protocols.
Method
Simulations based on Bloch equations of the two-pool exchange model3 which consider both exchange and relaxation processes were conducted to compare the T1 estimation difference among 2D VFA single-slice acquisition (SS), conventional multi-slice acquisition (CMS), and proposed IFAMS. Unlike CMS which one flip angle (FA) is used in one acquisition and then change the FA in another acquisition, the proposed IFAMS uses interleaved FAs of the multi-slices acquisition (e.g. 2 FAs scenario: first acquisition for odd-position slices uses 1st FA and even-position slices uses the 2nd FA, and second acquisition for odd-position slices uses 2nd FA and even-position slices uses 1st FA) to balance the MT effect between different acquisitions. The tissue parameters4 were: T1f = 860ms, T1r = 1s, T2f = 60ms, T2r = 11.4us, kf = 1.368 s-1, kr = 12 s-1, M0f = 1, M0r = 0.114. We used two flip angles (FA1=20° and FA2 = 50°) to generate signals with different contrasts. The time bandwidth product and duration time of 2D sinc RF pulses were respectively 4 and 3ms, and TR was 194ms. To explore the reproducibility across different protocols, the total number of acquisition slices varied from 1 to 30 to simulate how the slice number affect the T1 estimation. Another two combinations of flip angles (FA1=15°, FA2 = 45°; FA1=25°, FA2 = 55°) were investigated in the simulations.To validate the simulations, we performed in vivo experiments on a 3T Prisma scanner with a 20-channel head-neck-coil. A volunteer was scanned with the approval of the Institutional Review Board. The protocol of 2D GRE sequence was as follows: field of view (FOV) = 174×192 mm2, in-plane resolution = 1×1 mm2, slice thickness = 3 mm. Other parameters were the same as the simulations. In MS and IFAMS, a total of 40 slices were acquired with a concatenation of 2 which corresponds to 20 slices in simulations. Only the 19th slice located was scanned for SS. Finally, T1 mappings were obtained by using the dictionary matching based 2D VFA T1 mapping method5 which employs a single pool relaxometry model to correct both radio frequency excitation field (B1+) and slice excitation profile inhomogeneity. For comparison, the gold standard inverse recovery (IR) with TI = 100, 400, 800, 1200, 1800ms, TR = 6000ms, and a slice thickness of 4mm was performed to acquire the reference T1 mappings. White matter (WM) masks were generated using the FSL FAST tool to compare the T1 estimation results by different methods and protocols.
Results
In the simulations, compared with CMS, 2D VFA with IFAMS show more consistent estimated T1 values when varying the number of slices acquired and the FAs used (Figure 1). Figure 2 shows the T1 mappings of in vivo experiments by different methods and the whole brain T1 mappings of 2D VFA with IFAMS were shown in Figure 3. The histograms of T1 mappings after WM masking using different methods and protocols are shown in Figure 4, which validates the simulations.Discussion and Conclusion
Compared with 3D VFA method, the MT saturation of 2D VFA in one slice mainly come from off resonance excitation from other slices, and it can be seen in our simulation and in vivo experiment comparing single slice acquisition and multi-slice acquisition. To balance the MT effect in different acquisitions, we propose the IFAMS scheme for 2D VFA T1 mapping method. Both simulations and in vivo experiments results were performed, demonstrating enhanced accuracy and reproducibility of T1 mappings across different protocols when employing 2D VFA with IFAMS. Future work will encompass experiments involving a larger number of volunteers and tests across more protocols to further validate its reproducibility.Acknowledgements
This work was supported in part by the National Key Research and Development Program of China (No: 2020AAA0109502), by the National Natural Science Foundation of China (No: U1809204, 61701436), and by the Zhejiang Provincial Natural Science Foundation of China (No: LY22F010007).References
1. A.G. Teixeira RP, Malik SJ, Hajnal JV. Fast quantitative MRI using controlled saturation magnetization transfer. Magn Reson Med. 2019;81(2):907-920.
2. A. G. Teixeira RP, Neji R, Wood TC, Baburamani AA, Malik SJ, Hajnal JV. Controlled saturation magnetization transfer for reproducible multivendor variable flip angle T1 and T2 mapping. Magnetic Resonance in Medicine. 2020;84(1):221-236.
3. Murase K. Generalized equation for describing the magnetization in spoiled gradient-echo imaging. Magnetic Resonance Imaging. 2011;29(5):723-730.
4. Dortch RD, Li K, Gochberg DF, et al. Quantitative magnetization transfer imaging in human brain at 3 T via selective inversion recovery. Magnetic Resonance in Med. 2011;66(5):1346-1352.
5. Chen Y, Liu H, Ye H. Dictionary Matching Based 2D Thin Slice Generalized Slice-dithered Enhanced Resolution (gSlider) Variable Flip Angle T1 Mapping. In: Lu H, Ouyang W, Huang H, et al., eds. Image and Graphics. Lecture Notes in Computer Science. Cham: Springer Nature Switzerland; 2023:93-105.
Figures
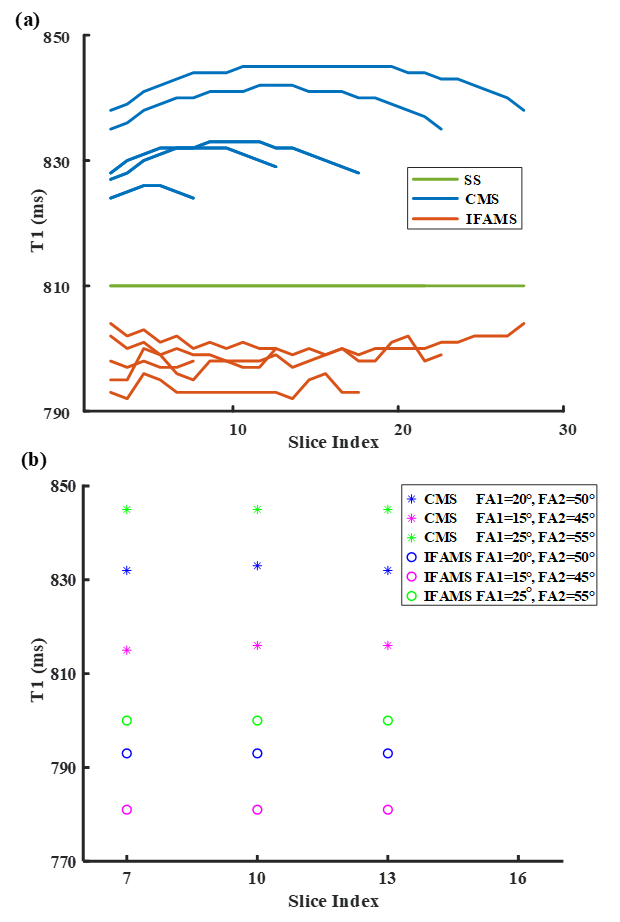
Figure 1. (a) The simulated T1 estimation values by CMS (blue), IFAMS (orange), and SS (green) method with FA1=20° and FA2=50°. Acquisition slices varied from 1 to 30 were set and only the 10th, 15th, 20th, 25th, and 30th slice were shown. (b) The simulated T1 estimation values of 7th, 10th, and 13th slice in a total 20 slices acquisition by CMS (star) and IFAMS (circle) with three different protocols.
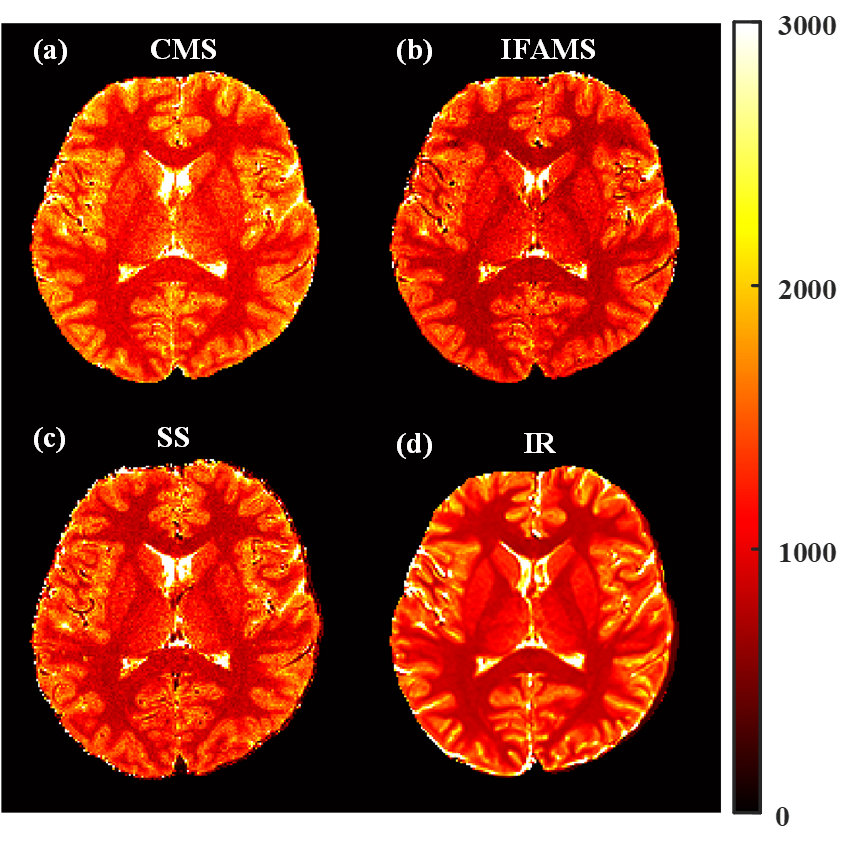
Figure 2. T1 mappings employing 2D VFA (FA1=20°, FA2=50°) with CMS (a), IFAMS (b), and SS (c). (d) T1 mappings using IR method.
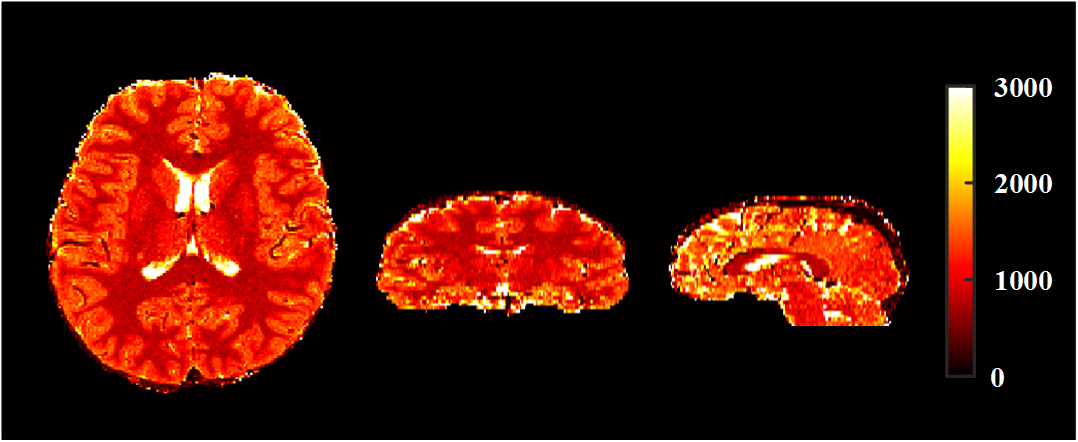
Figure 3. Whole brain T1 mappings using 2D VFA IFAMS including horizontal, coronal, and sagittal plane.
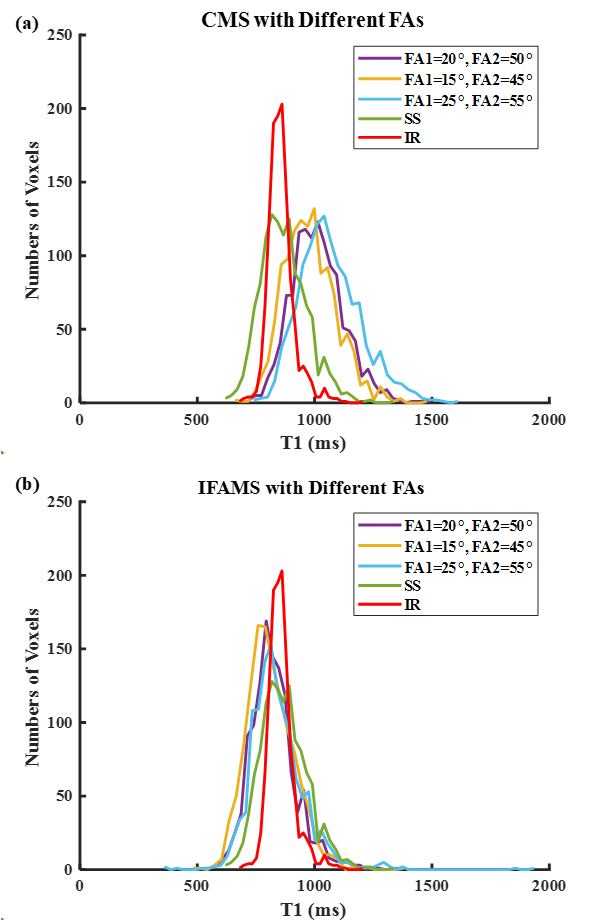
Figure 4. (a) Histograms of T1 mappings after WM masking by 2D VFA CMS with three different combinations of FAs, 2D VFA SS, and IR. (b) Histograms of T1 mappings after WM masking by 2D VFA IFAMS with three different FAs, 2D VFA SS, and IR.