3814
Combing CT coronary artery calcification score and deep learning MR late gadolinium enhancement to detect unrecognized myocardial infarction1Department of radiology, Renmin Hospital Wuhan University, Wuhan, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Cardiovascular
Motivation: Coronary artery calcification score (CACS) is currently a common and widely-accepted indication of UMI, but it itself fails to accurately reflect myocardial ischemia in patients with unrecognized myocardial infarction(UMI).
Goal(s): To establish a UMI-screening workflow for a cohort who receive a physical examination.
Approach: To explore the detection rate of myocardial infarction (MI) using CACS only, Parea only, CACS in combination with Parea using different thresholds.
Results: The AI-CACS combined with Parea had higher diagnostic performance on differentiating UMI from non-UMI groups than AI-CACS or Parea alone, especially AI-CACS combined with Parea-DL-5SD with AUC of 0.914.
Impact: Patients with UMI usually do not have typical symptoms of cardiogenic chest pain. CACS-Parea-DL-5SD can detect unrecognized myocardial infarction in the outpaitnets, and increased the diagnostic confidence of UMI, providing an important reference for UMI risk stratification and follow-up recommendations.
INTRODUCTION
The incidence of unrecognized myocardial infarction (UMI) increases every decade[1]. Patients with UMI often lack typical symptoms, making it essential to confirm myocardial infarction/ischemia using ECG and coronary computed tomography artery (CCTA) along with elevated troponin levels[2]. Highly agreeing to manual measurements, artificial intelligence-based non-gated chest CT coronary artery calcification score (AI-CACS) can reflect the extent of coronary artery calcification (CAC) [3]. But, CACS itself fails to accurately reflect myocardial ischemia in patients with UMI, and not to mention the degree and extent of ischemia by AI-CACS alone [4]. Late gadolinium enhancement (LGE) is effective for assessing cardiac function but is rarely used for UMI detection. Deep learning algorithms like Deep Neural Networks (DNN) and Convolutional Neural Networks (CNN) are applied to enhance image quality and image reconstruction[5]. A new inline deep-learning-based reconstruction (DLR) algorithm improves image quality, reduces artifacts, and eliminates interpretation differences[6]. Up to now, there is no DLR-based LGE (LGEDL) study in evaluation of patients with UMI. Therefore, this study aimed to explore the clinical value of AI-CACS combined with the percentage of myocardium enhancement area (Parea) on LGEDL (Parea-DL) in assessment of diagnostic performance on unrecognized myocardial infarction.METHODS
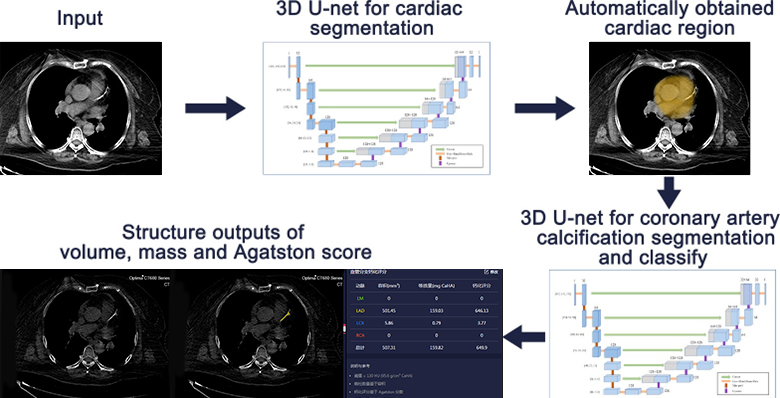
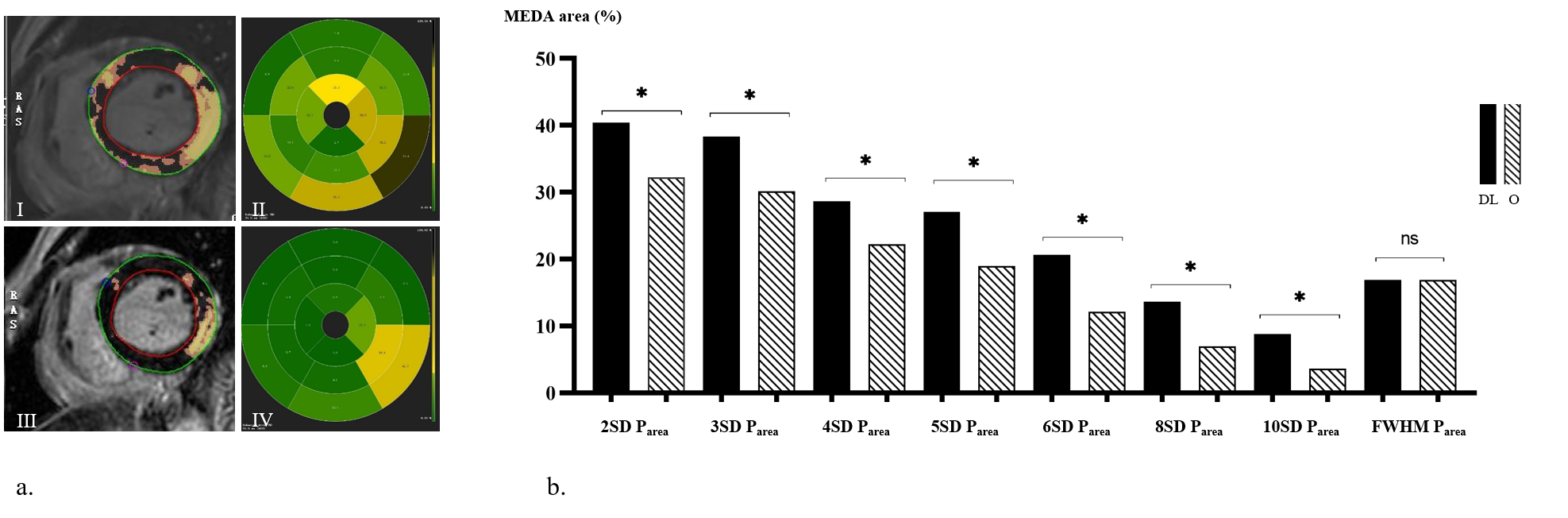
This study was approved by the hospital and prospectively included 1679 patients underwent non-gated chest CT scans for physical examinations from March 2022 to April 2023. A subset of 83 volunteers underwent cardiac magnetic resonance (CMR) including LGE (TE 2.7ms, flip angle 25°, field of view = 34 cm ×34 cm, matrix size = 260 × 174, slice thickness = 8 mm, gap = 2 cm, bandwidth = 83.33kHz, echo train length = 24, number of excitation = 1, theoretical acquisition time = 8 s × 9 heartbeats) on 3.0 T MRI scanner (Signa Architect, GE Healthcare) at our hospital from April to September 2022. Non-gated chest CT scans were performed on all subjects, and AI-CACS software was used to automatically assess coronary artery calcification (Fig. 1). CMR examinations included LGE sequences, and both conventional LGE images (LGEO) and DLR LGE images (LGEDL) were generated. The percentage of myocardium enhancement area (Parea) was assessed for cardiovascular disease diagnosis (Fig.2). Qualitative and quantitative evaluations of CMR images were conducted by radiologists, and Parea was assessed using Cvi42 software. The diagnostic accuracy of Parea-DL and Parea-O in differentiating patients with UMI was compared using clinical diagnosis as the gold standard.Statistical analysis was performed using R-project (version 4.0.4, http://www.r-project.org), and various tests were used to assess the diagnostic efficacy of AI-CACS and Parea in differentiating UMI from non-UMI, including area under the curve (AUC), accuracy, precision, sensitivity, specificity, and other measures. p<0.05 was considered statistically significant.RESULTS
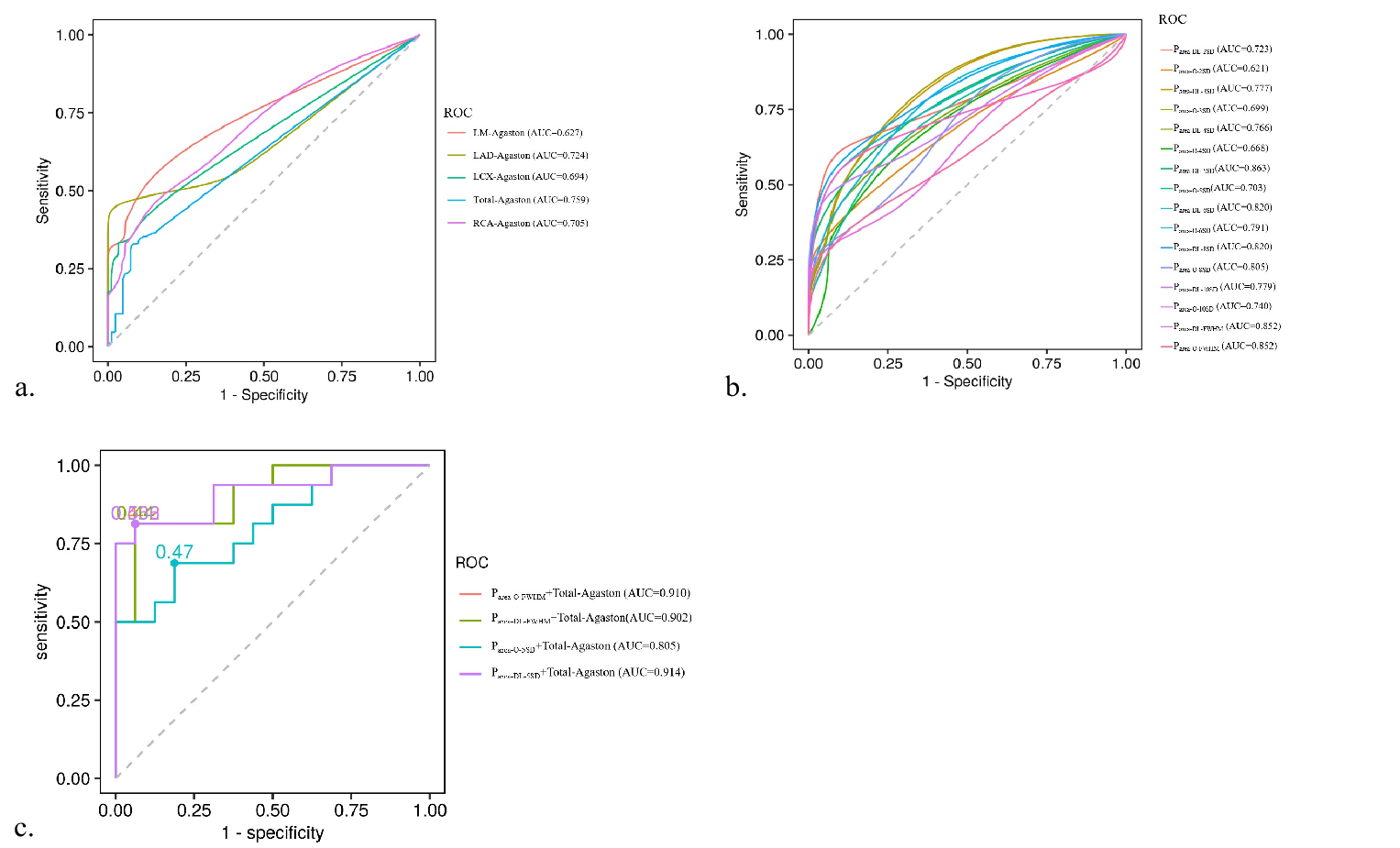
A total of 66 suspicious UMI volunteers were studied (48 males, and 18 females, mean age: 56.17 years ± 8.65). The AUC value of Total-Agaston for UMI diagnosis was 0.759 (p<0.001) with the optimal cut-off value of 109.69 (a.u.) (Fig.3). Parea-DL-5SD, Parea-O-FWHM and Parea-DL-FWHM showed the consistent diagnostic accuracy of UMI with AUC, sensitivity and specificity of 98.47%, 77.11% and 99.84%. The AI CACS combined with Parea-DL-5SD (CACS-Parea-DL-5SD) had the highest diagnostic performance on differentiating UMI from non-UMI groups with AUC of 0.914, sensitivity = 81.25%, specificity = 93.75%, and accuracy = 87.50%. Intra- and inter-rater agreement for Parea-DL showed higher than Parea-O (respectively ICC = 0.84-0.97 and 0.73-0.96, p < 0.001) (Fig.3) .DISCUSSION
Our findings suggested that CACS-Parea-DL-5SD elevated screen-out rate for unrecognized myocardial infarction (UMI) with the best AUC of 0.914 whereas 90 (5.36%) subjects with suspected UMI out of 1679 outpatients only reached AUC of 0.759. LGEDL and LGEO showed strong consistency in Parea measurements despite no significantly different in the number of detected UMI patients. Coronary artery calcification (CAC) is associated with a higher UMI risk, and the combination of CACS and myocardial enhancement area improves UMI detection, even in asymptomatic patients[7]. However, CACS may not directly reflect the severity of myocardial ischemia, as it primarily reflects coronary artery disease burden[8]. The study suggested that AI-CACS and DLR-based LGE can be used for timely UMI detection, risk stratification, and follow-up recommendations, benefiting individuals undergoing physical examinations. To optimize algorithm in avoidance of overfitting to improve accuracy of AI-CACS and LGEDL using as onsite data as input for training can be achieved in the future.CONCLUSION
AI-CACS combined with DLR-based LGE can detect unrecognized myocardial infarction in the population who receive physical examination and increase the diagnostic confidence of UMI, providing an important reference for UMI risk stratification and follow-up recommendations.Acknowledgements
None.References
[1] Sugiyama T, Kanaji Y, Hoshino M, et al. Relationship Between Unrecognized Myocardial Infarction and Underlying Coronary Plaque Characteristics on Optical Coherence Tomography. JACC Cardiovasc Imaging 2022;15(10):1830-1832.
[2] Pickhardt PJ, Summers RM, Garrett JW, et al. Opportunistic Screening: Radiology Scientific Expert Panel. Radiology 2023;307(5):e222044.
[3] Xu J, Liu J, Guo N, et al. Performance of artificial intelligence-based coronary artery calcium scoring in non-gated chest CT. EurRadiol 2021;145(12):1-11.
[4] El-Rewaidy H, Neisius U, Mancio J, et al. Deep complex convolutional network for fast reconstruction of 3D late gadolinium enhancement cardiac MRI. NMR Biomed 2020;33(7): e4312.
[5] Xue H, Rehman A, Davies RH, Moon JC, Fontana M , Kellman P. CNNT DB-LGE: free-breathing dark blood late enhancement imaging using the convolutional neural network transformer speeds acquisition by 50%. Eur Heart J Cardiovasc Imaging. 2022;23: ii11-ii12.
[6] Nikki van der Velde,H. CarlijneHassing,Brendan J. Bakker, et al. Improvement of late gadolinium enhancement image quality using a deep learning–based reconstruction algorithm and its influence on myocardial scar quantification. Eur Radiol 2021;31(6):3846–3855.
[7] Boccalini S, Teulade M, Paquet E, et al. Silent myocardial infarction fatty scars detected by coronary calcium score CT scan in diabetic patients without history of coronary heart disease. Eur Radiol 2023,2. doi: 10.1007/s00330-023-09940-2.
[8] Rijlaarsdam-Hermsen D, Lo-Kioeng-Shioe M, van Domburg RT, Jaap W Deckers, Dirkjan Kuijpers, Paul R M van Dijkman. Stress-Only Adenosine CMR Improves Diagnostic Yield in Stable Symptomatic Patients with Coronary Artery Calcium. JACC Cardiovasc Imaging 2020;13(5):1152-1160.
Figures