3813
Fully Automated Deep Learning 3D Segmentation of the Aorta from Contrast Enhanced Magnetic Resonance Angiography Images1Department of Radiology, Northwestern University, Chicago, IL, United States
Synopsis
Keywords: AI/ML Software, Machine Learning/Artificial Intelligence, Contrast enhanced MRA, MRA, Magnetic Resonance Angiography
Motivation: Contrast-enhanced MRA (CE-MRA) of the thoracic aorta is an essential to assess and monitor aortic complications, and to quantify aortic dimensions. However, aortic dimensions’ measurement is cumbersome. Thus, automating aortic 3D-segmentation from CE-MRA is important to improve analysis workflow efficiency.
Goal(s): We aimed to, accurately and precisely, automate thoracic aorta 3D-segmentation from CE-MRA scans using deep-learning.
Approach: Using 125 CE-MRA scans we trained and tested a convolutional neural network to automatically segment the thoracic aortic.
Results: Automated-segmentations was faster to output and had excellent agreement with manual-segmentations in metrics like aortic diameters and volume, dice scores, Hausdorff distance and average symmetrical surface distance.
Impact: To our knowledge, this is the first study that implemented a fully-automated 3D-segmentation of contrast-enhanced MRA images. Such automation could possibly facilitate the clinical workflow when combined with future applications aiming at automating dimensions’ calculation at standardized locations.
Introduction
Contrast enhanced magnetic resonance angiography (CE-MRA) of the thoracic aorta is a reliable and reproducible imaging technique that allows the evaluation of aortic anatomy, structure, and dimensions. Aortic morphology and dimensions enable physicians to assess and monitor aortic complications such as dilation and aneurysm without the need of ionizing radiation1,2. However, quantification of aortic dimensions requires manual measurements at multiple anatomical levels which is cumbersome and time consuming, especially with variations in contrast intensities. Thus, automating the process of obtaining aortic measurements from raw CE-MRA images is of clinical importance to facilitate workflow and reduce analysis/reporting time. The purpose of this study was to employ deep learning in order to obtain a fully automated 3D-segmentation of the thoracic aorta followed by identification of anatomic landmarks and reporting aorta dimensions at multiple levels.To date, most deep-learning based aorta segmentations were implemented on computed tomography angiography (CTA)3-6. There are few reports on automated aorta 3D-segmentation in non-contrast enhanced MRA and time resolved 2D phase-contrast MRI but none for 3D CE-MRA7-9. In this study, we implemented a convolutional neural network (CNN) for the segmentation of the aorta from CE-MRA images.
Methods
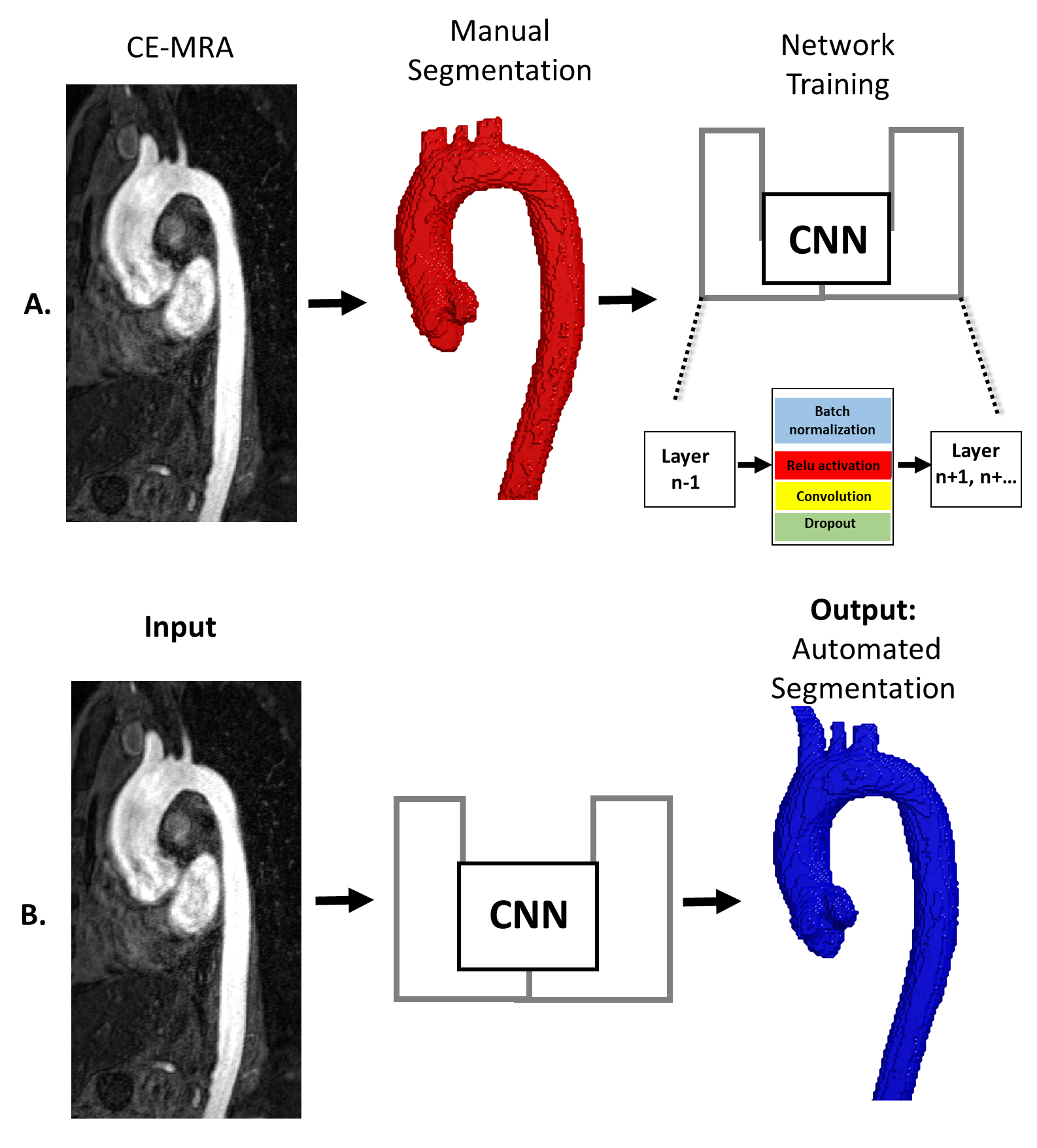
We retrospectively identified 125 patients with 3D CE-MRA scans of the thoracic aorta acquired at Northwestern Memorial Hospital (2011-2020). 3D CE-MRA scan parameters were: flip angle= 25-40, TE= 0.89-1.23ms, and spatial resolution= 0.63-1.3 x 0.63-1.3 x 1-2 mm3. The aorta was manually segmented for all scans using a dedicated software (MIMICS). As shown in Figure 1A, this 3D-segmentation served as ground-truth for CNN training and testing. The training data included 92 scans (27F/65M, 49.1 ± 16.6 years) and the testing data consisted of 33 cases (8F/25M, 49.1 ± 15.8 years).The CNN was based on a 3D-UNet consisting of DenseNet blocks (Figure 1A). Each block constituted of a series of 3D-convolutions, batch normalization, rectified linear unit activation, and a dropout layer. These functions were applied “n” number of times with increasing frequency at deeper layers of the CNN. After each layer, previous feature maps were concatenated and used as input for subsequent layers. Post-contrast 3D CE-MRA images were used as a single input (Figure 1B).
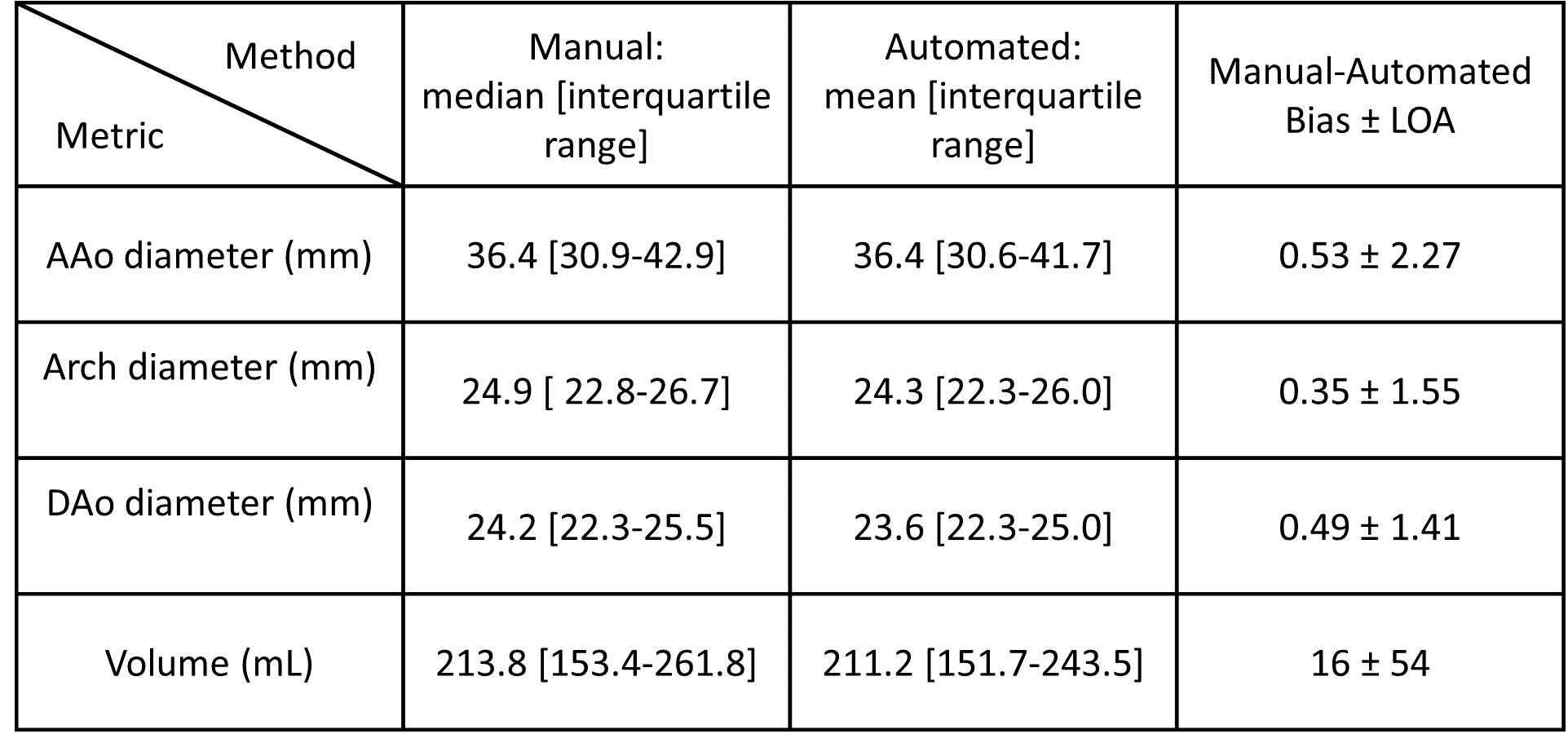
To compare ground truth versus CNN-derived aortic 3D-segmentations, Dice score (DS), Hausdorff distance (HD), and average symmetrical surface distance (ASSD) were calculated. Planes were placed orthogonal to automatically-generated centerline and used to calculate the largest aortic diameter at the ascending aorta (AAo), arch, and descending aorta (DAo). Aortic volume from 3D-segmentation was also calculated. All values are reported as mean/median ± standard deviation [interquartile range] depending on normality.
Results
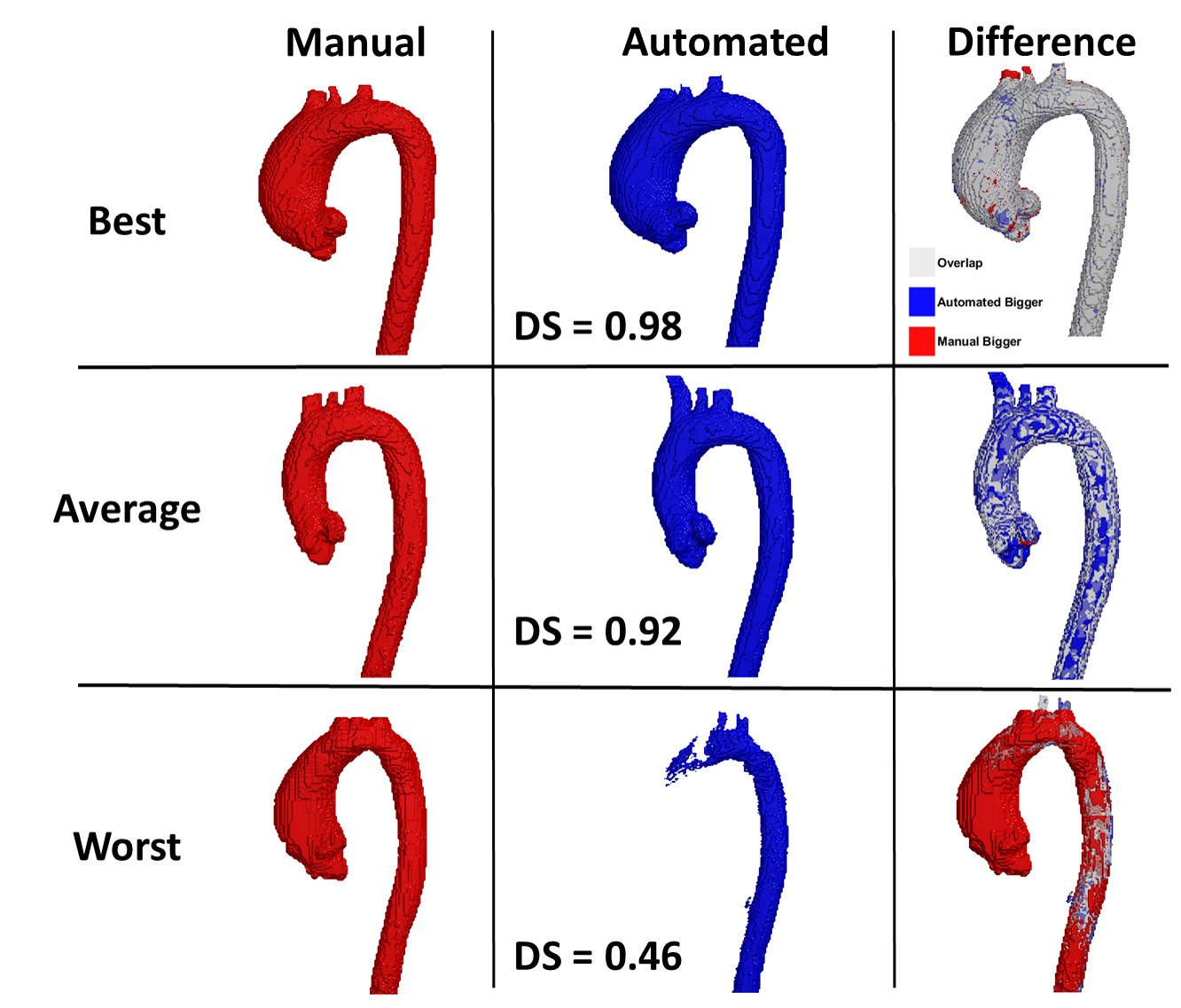
The CNN required 302 minutes to train and 1.52 ± 0.15 s to segment the aorta compared to 10-20 minutes manually. Examples of best, average, and worst aorta 3D-segmentation agreement are shown in Figure 2. The worst case was the only failed case where the AAo and arch were missing which prevented calculation of aortic dimension. This case was excluded from the diameter analysis but not from volume and performance assessment.The CNN’s performance was as follows: DS = 0.95 [0.91-0.97], HD = 4.0 mm [1.8-7.5], and ASSD = 0.22 mm [0.09-0.56]. Diameter and volume metrics showed excellent agreement between manual and CNN-derived segmentations (AAo= 1.0%; Arch= 2.0%; DAo= 1.8%; volume = 6.4%).
Discussion
A CNN was developed for fast and fully automated 3D-segmentation of the thoracic aorta from 3D CE-MRA input data. Our results demonstrate manual-level segmentation performance and excellent agreement across the mentioned aortic metrics. The only failure case shown in Figure 2C could be attributed to variations in aortic contrast with respect to the surrounding structures in the patient’s scan. This highlights the possible importance of including pre-bolus sequences or even non-contrast 3D MRA in the training datasets. Future studies should also include inter-observer assessment of CE-MRA manual segmentation to assess human vs CNN performance for aortic 3D segmentation accuracy.Our network’s performance was on par with CT-angiography based studies (DS=0.95 and DS = 0.88-0.96, respectively)3-4. When compared to automation of non-enhanced MRA data, we achieved better agreement (DS=0.85 vs. DS = 0.95)7. Studies on 2D phase-contrast MRI achieved similar dice scores of around 0.958-9.
To our knowledge, this is the first study that implemented automated aortic 3D-segmentation of CE-MRA scans. Future efforts will be directed to implement a second automated step that would localize standardized anatomic landmarks, according to the American Heart Association guidelines, and extract dimensions that physicians currently obtain manually. Such automation could possibly aid physicians to decrease reading and reporting durations.
Acknowledgements
No acknowledgement found.References
1. Aguet, J., Gill, N., Tassos, V. P., Chavhan, G. B., & Lam, C. Z. (2022). Contrast-enhanced body magnetic resonance angiography: how we do it. Pediatric Radiology, 52(2), 262-270.
2. Zhang, H., Maki, J. H., & Prince, M. R. (2007). 3D contrast‐enhanced MR angiography. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 25(1), 13-25.
3. Cao L, Shi R, Ge Y, et al. Fully automatic segmentation of type B aortic dissection from CTA images enabled by deep learning. Eur J Radiol. 2019;121:108713.
4. Kurkure U, Avila-Montes OC, Kakadiaris IA. Automated segmentation of thoracic aorta in non-contrast CT images. In: 2008 5th IEEE International Symposium on Biomedical Imaging: From Nano to Macro. IEEE; 2008:29-32.
5. Mohammadi S, Mohammadi M, Dehlaghi V, et al. Automatic Segmentation, Detection, and Diagnosis of Abdominal Aortic Aneurysm (AAA) Using Convolutional Neural Networks and Hough Circles Algorithm. Cardiovasc Eng Technol. 2019;10: 490–499.
6. Zheng Y, John M, Liao R, et al. Automatic aorta segmentation and valve landmark detection in C-arm CT: application to aortic valve implantation. In: International Conference on Medical Image Computing And-Assisted Intervention. Springer; 2010:476-483.
7. Hepp, T., Fischer, M., Winkelmann, M. T., Baldenhofer, S., Kuestner, T., Nikolaou, K., ... & Gatidis, S. (2020). Fully automated segmentation and shape analysis of the thoracic aorta in non–contrast-enhanced magnetic resonance images of the German National Cohort Study. Journal of Thoracic Imaging, 35(6), 389-398.
8. Herment, A., Kachenoura, N., Lefort, M., Bensalah, M., Dogui, A., Frouin, F., ... & De Cesare, A. (2010). Automated segmentation of the aorta from phase contrast MR images: validation against expert tracing in healthy volunteers and in patients with a dilated aorta. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 31(4), 881-888.
9. Codari, M., Scarabello, M., Secchi, F., Sforza, C., Baselli, G., & Sardanelli, F. (2018). Fully automated contour detection of the ascending aorta in cardiac 2D phase-contrast MRI. Magnetic Resonance Imaging, 47, 77-82.
Figures