3805
Classification of Benign and Malignant Parotid Gland Tumors using Deep Learning and 2.5D MRI1The First Affiliated Hospital of Jinan University, Guangzhou, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Machine Learning/Artificial Intelligence
Motivation: Preoperative distinguishment of the benign parotid gland tumors from the malignant determines the surgical scope; however, identifying tumor nature with only T1-weighted and fat-suppressed T2-weighted images is challenging.
Goal(s): Inserting three adjacent slices of the tumor into the RGB channels of a 2D image as 2.5D images coupled with transfer learning was utilized.
Approach: Using 2D and 2.5D images as input, a ResNet-101 model, pre-trained on ImageNet, was employed for transfer learning to facilitate the prediction.
Results: Deep learning models discerned malignant parotid gland tumors from the benign, especially 2.5D model showed superior performance to 2D model.
Impact: The transfer learning and 2.5D-MRI based classification model offered new insights to differentiate the malignant parotid gland tumors from the benign ones, especially when sample quantities are limited.
Introduction and Purpose
Parotid gland tumors account for about 2-3% of head and neck tumors[1]. The treatments for benign and malignant tumors vary; clinically, conservative treatment or simple tumorectomy is generally recommended for benign cases[2]. For malignant tumors, the primary approach is a complete radical surgical resection of the primary tumor, ensuring sufficiently available margins. Preoperative prediction of the tumor's benign or malignant nature holds significant implications for the patients with high-risk for postoperative radiation therapy. The efficacy of the diagnostic gold standard, Fine Needle Aspiration Biopsy, is hampered by the histological similarities between benign and malignant tumors[3], and the biopsy procedure has potential in malignant tumor spreading [4]. Despite magnetic resonance imaging (MRI) remains the optimal imaging modality, differentiating MRI manifestations of benign and malignant tumors poses a challenge to precise diagnosis. The Convolutional Neural Networks based on transfer learning have shown potential in precise prediction of other types of tumors. Due to the rarity of parotid gland tumors, the deep learning research based on MRI images is rare. This study adopts the emerging 2.5D image processing technique and transfer learning approach, aiming to construct a deep learning prediction model using limited samples.Materials and Methods
MRI datasets of 92 patients (63 benign and 29 malignant cases) with initially diagnosed as parotid gland tumors and untreated at the First Affiliated Hospital of Jinan University between January 2015 and January 2023 were retrospectively collected by 3.0T magnetic resonance scanner (Signa Premier, GE healthcare, Waukesha, WI). .The datasets including T1-Weighted Imaging (T1WI) and Fat-Suppressed T2-Weighted Imaging (T2WI-FS) for each patient were segregated into training and validation cohorts at an 8:2 ratio. All tumors were demarcated by adding 15 pixels around the lesion's maximum diameter as the segmentation scope and then segmented. Those tumor segments were further bifurcated into 2D groups (434 images in training set; 120 images in validation set) and 2.5D groups (290 images in training set; 79 images in validation set). The planar images in 2D group were inputted via slicing 3-dimensional (3D) lesion along the z-axis, while in 2.5D group, 2.5D images were formed by inserting three adjacent slices of the tumor into the RGB channels of a 2D image, thereby creating a pseudo 2D image with information from three different planes. This arrangement allows for the expression of a certain degree of 3D spatial information within a 2D image format. Parameter fine-tuning was executed on a pre-trained ResNet101 model using the ImageNet dataset as source inputs, facilitating transfer learning for classification endeavor in this study. The final classification model was chosen based on the Area Under the Curve (AUC) and Loss values. Gradient-weighted Class Activation Mapping (Grad-CAM) heatmaps alongside feature maps were employed for visualizing model predictions.Results
All the evaluation metrics for the deep models are presented in Table 1. The 2.5D-based deep learning T1WI model had the best predictive performance with AUC of 0.95 and 0.89 and accuracies of 0.87 and 0.77 respectively for the training and validation sets (Figure 2). The training loss (Train Loss) and validation loss (Val Loss) for each group of deep learning models was inclined to stabilize across different training epochs (Epoch), and the small difference between the training and validation sets indicated good fitting performance (Figure 3). The feature maps and Grad-CAM heatmaps visualized the decision-making process of the deep learning models (Figure 1).Discussion and Conclusions
The deep learning 2.5D-T1WI model exhibited excellent performance in the classification of parotid gland tumors. As illustrated by the Grad-CAM heatmap and feature maps, the model were built using hierarchical features of the tumor and surrounding areas. In the learning process from the lower to the upper layers, the features gradually became more complex; in the end, the final prediction analysis was based on the features from the top layer.Compared to traditional radiological and radiomic analyses[5,6], deep learning end-to-end models reduced human interference and elevated diagnostic accuracy and objectivity via automatedly extracting image features. Under limited sample size, utilizing 2.5D image strategy and transfer learning for training deep learning models yielded good predictive performance for low-incidence tumors.
Even though a small sample size with solely on T1WI and T2WI images from only one center may restrict robustness and generalization, our study initially proved deep learning models based on routine pre-operative MRI could effectively differentiate the benign parotid gland tumors from the malignant ones, providing valuable insights for clinical decision-making.
Acknowledgements
Funding: This project was supported by the Science and Technology Projects in Guangzhou, China (2023A03J0609), Guangdong Basic and Applied Basic Research Foundation (2022A1515110630).
References
[1] Bradley P J, McGurk M. Incidence of salivary gland neoplasms in a defined UK population[J]. British Journal of Oral and Maxillofacial Surgery, 2013, 51(5): 399-403.
[2] Park Y M, Kang M S, Kim D H, et al. Surgical extent and role of adjuvant radiotherapy of surgically resectable, low-grade parotid cancer[J]. Oral Oncology, 2020, 107: 104780.
[3] Feinstein A J, Alonso J, Yang S, et al. Diagnostic Accuracy of Fine‐Needle Aspiration for Parotid and Submandibular Gland Lesions[J]. Otolaryngology–Head and Neck Surgery, 2016, 155(3): 431-436.
[4] Bjørndal K, Krogdahl A, Therkildsen M H, et al. Salivary gland carcinoma in Denmark 1990-2005: a national study of incidence, site and histology. Results of the Danish Head and Neck Cancer Group (DAHANCA)[J]. Oral Oncology, 2011, 47(7): 677-682.
[5] Maraghelli D, Pietragalla M, Cordopatri C, et al. Magnetic resonance imaging of salivary gland tumours: Key findings for imaging characterisation[J]. European Journal of Radiology, 2021, 139: 109716.
[6] Zheng Y mei, Li J, Liu S, et al. MRI-Based radiomics nomogram for differentiation of benign and malignant lesions of the parotid gland[J]. European Radiology, 2021, 31(6): 4042-4052.
Figures
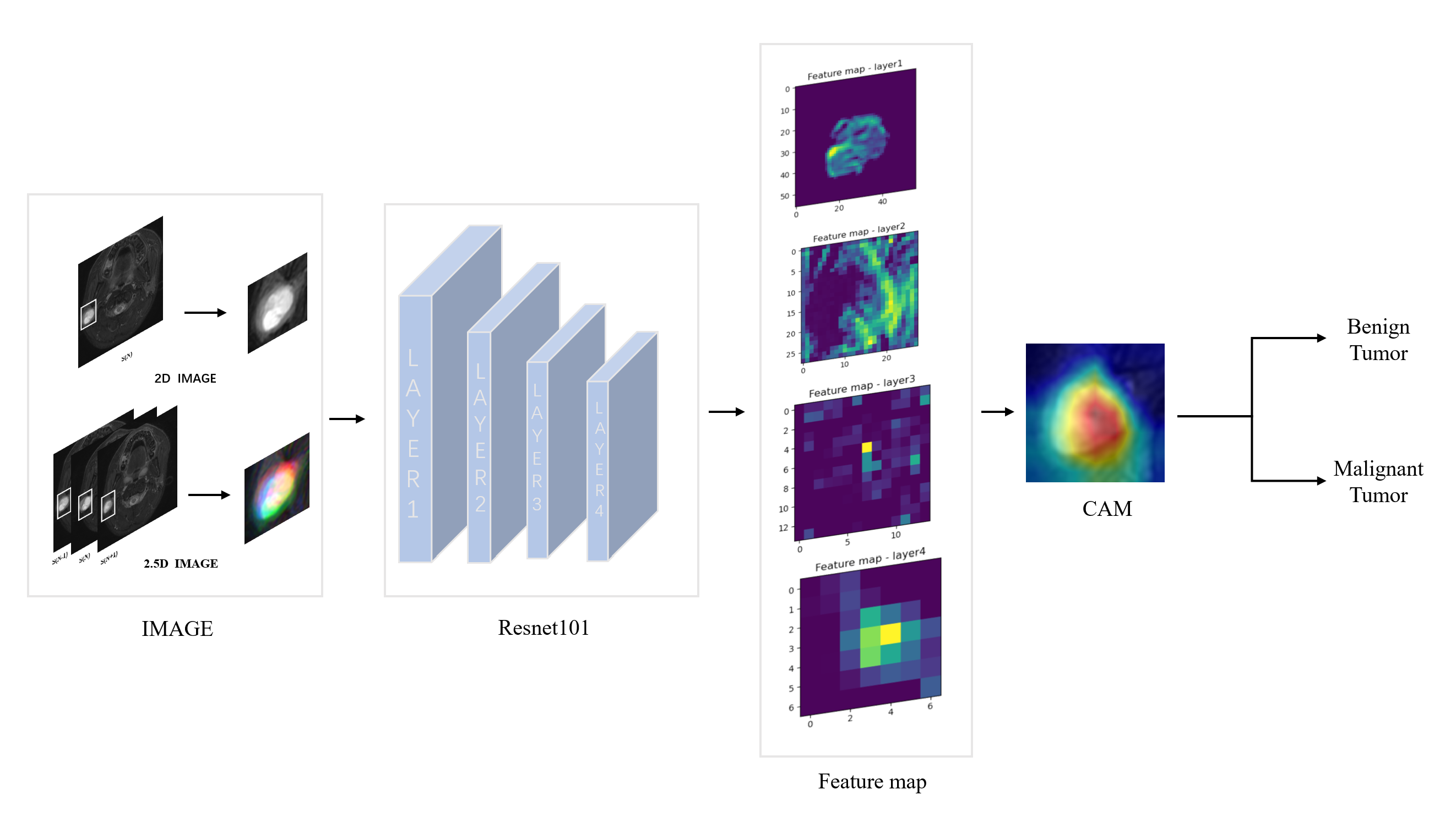
Figure1: Experimental Workflow Diagram for Deep Model Construction. A 2D image encapsulates the axial slice of the lesion, while a 2.5D image is formulated by integrating three contiguous tumor slices into the RGB channels of a 2D image, thus embodying information across three tumor planes. The deep learning model ResNet-101 leverages pre-trained weights acquired from the extensive dataset, ImageNet. Feature Maps illustrate the visualized features procured from diverse layers of the input image. Grad-CAM heatmap elucidates the lesion regions instrumental in model predictions.
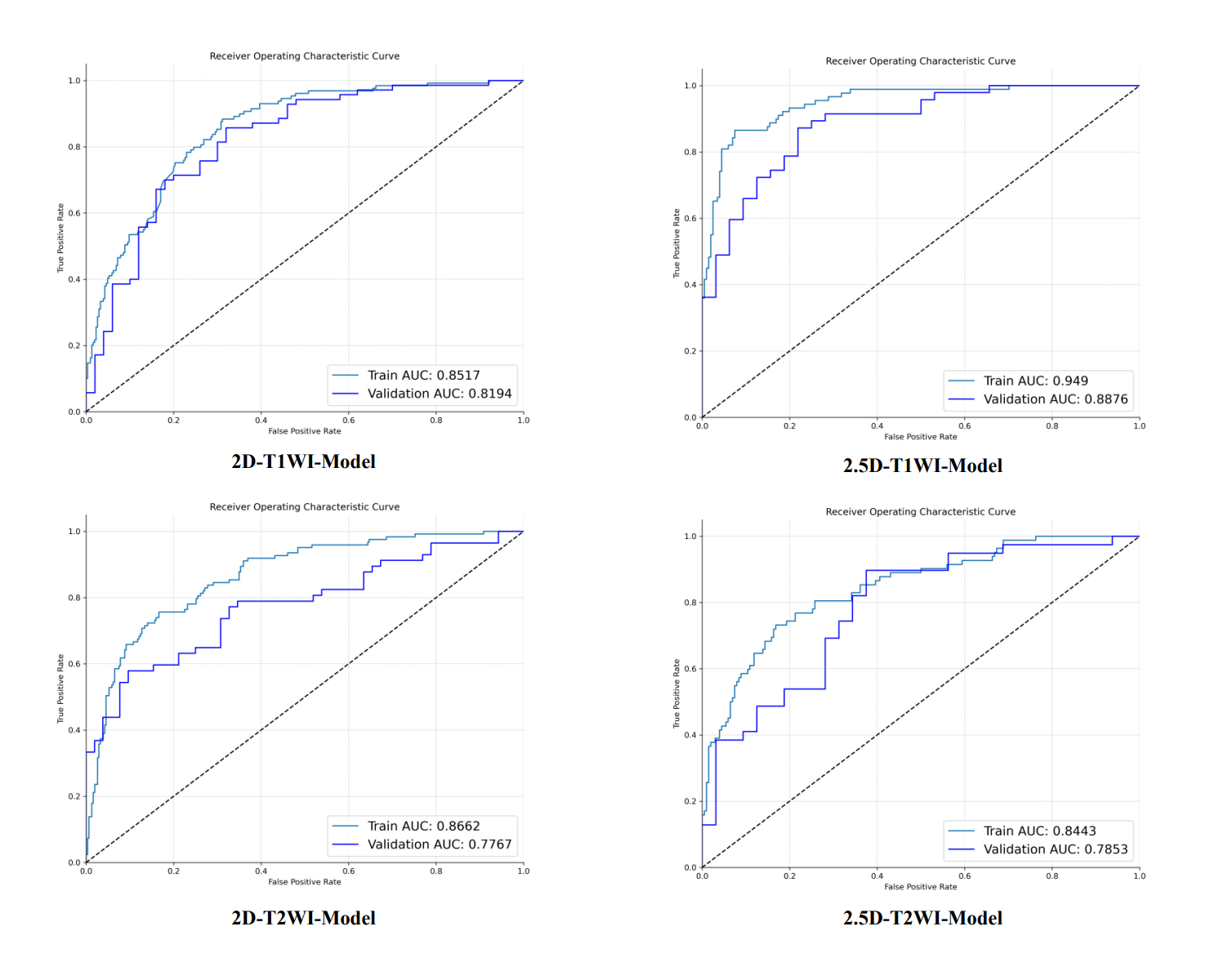
Figure 2: ROC curves of different model groups in the training and validation sets along with corresponding AUC values, where the x-axis represents the false positive rate (FPR) and the y-axis represents the true positive rate (TPR).
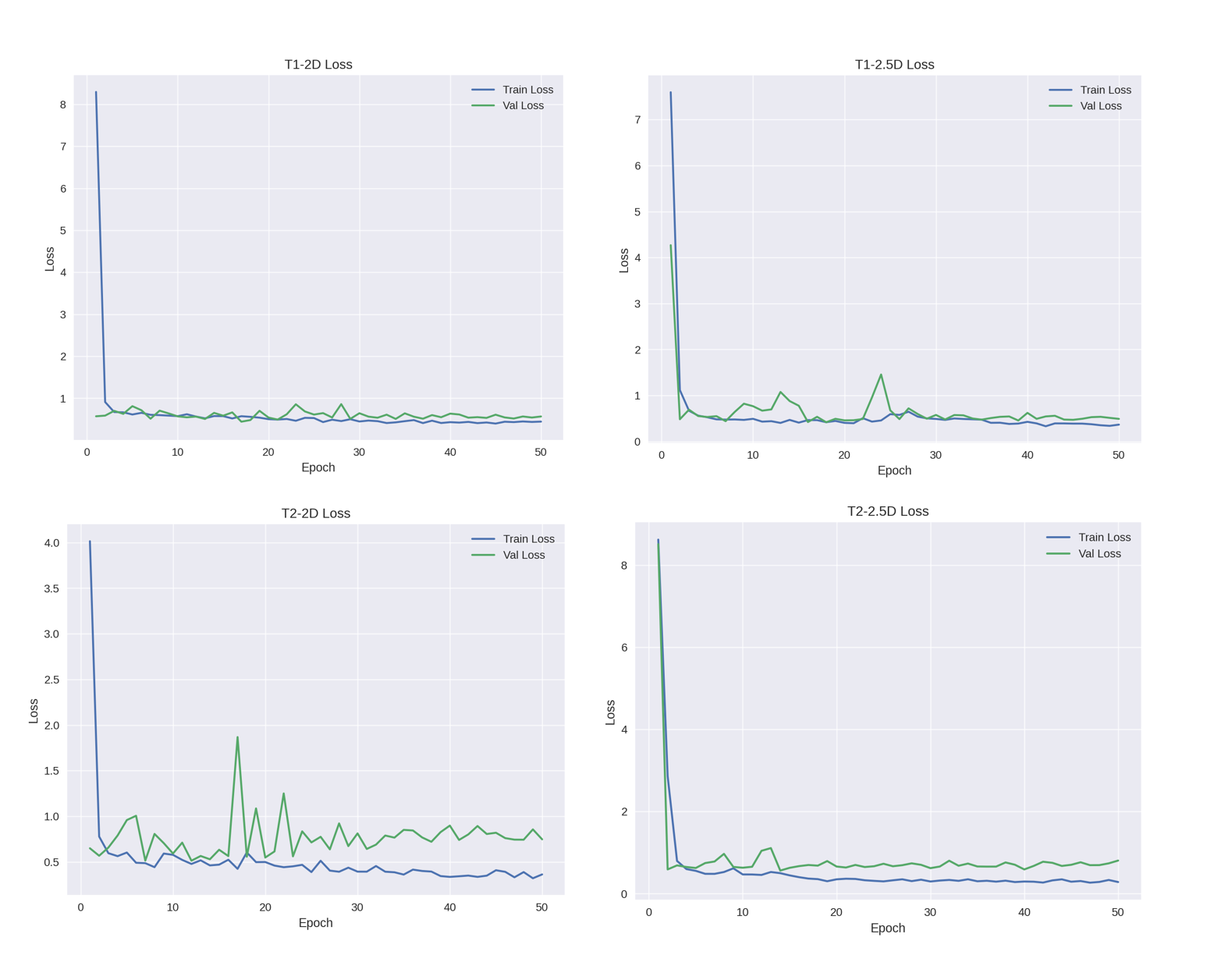
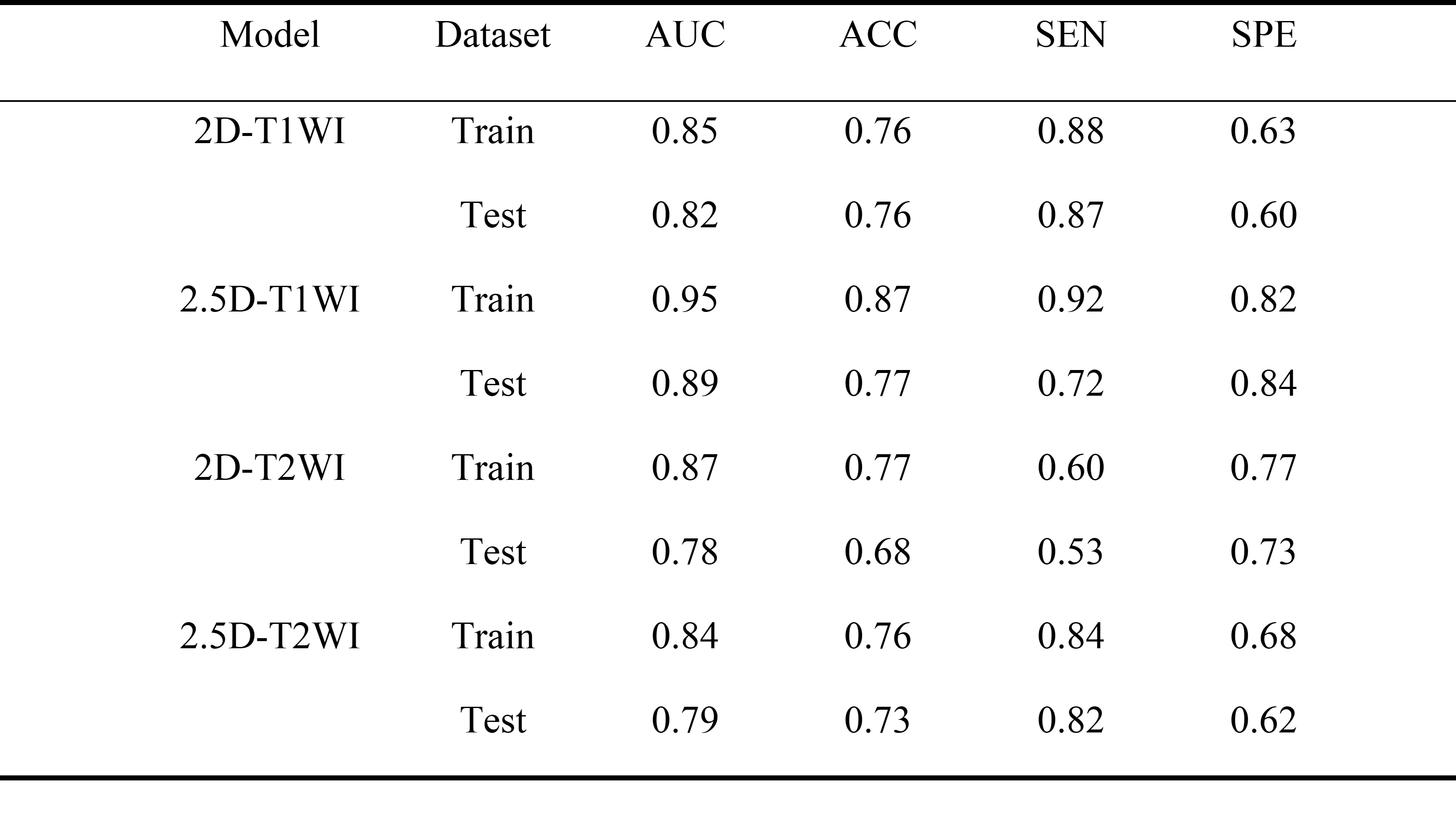
Table 1: Classification efficacy of the bulit deep learning models for 2D and 2.5D groups in the training and testing sets.