3792
AI-enhanced prognostication in cardiac resynchronization therapy using displacement encoding with stimulated echoes (DENSE) MRI1University of Virginia, Charlottesville, VA, United States
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence
Motivation: The need to address the challenge of a high nonresponse rate (approximately 40%) in CRT patients.
Goal(s): By leveraging advanced computational methods, this research seeks to redefine risk stratification and long-term survival prediction.
Approach:
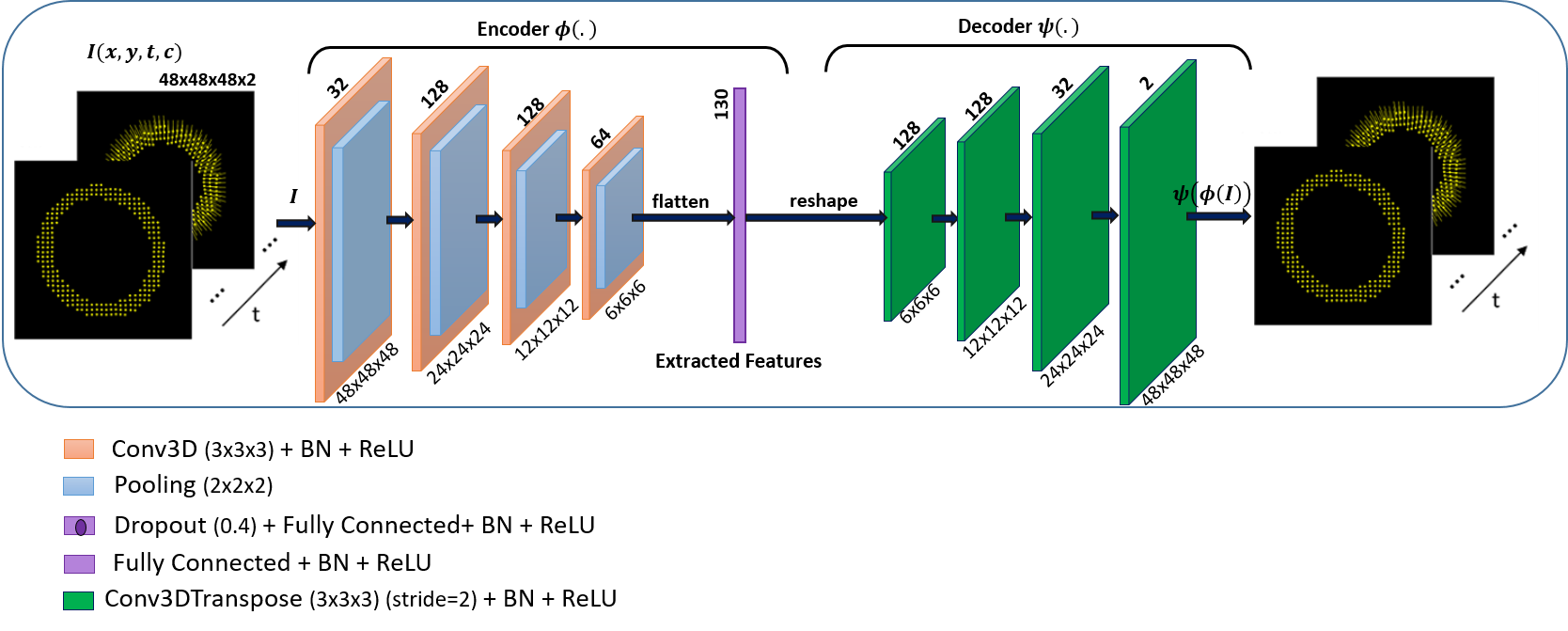
- 3D-CAE model is designed to compress displacement trajectories into a low-dimensional latent code while preserving sufficient information for trajectory reconstruction.
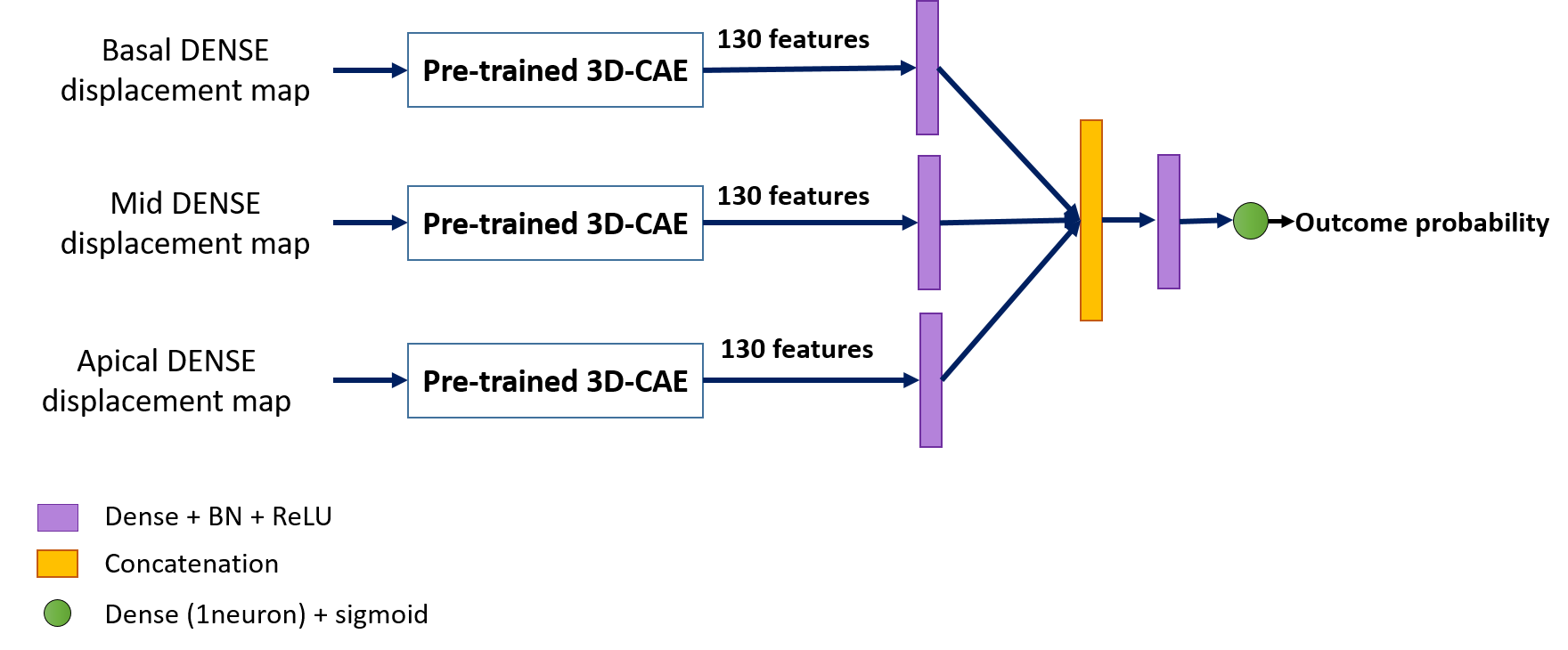
- The survival network utilizes latent features from three specific slices for predicting 4-year survival of patients post-CRT.
Results:
- 3D-CAE model effectively learned to extract latent features and reconstructed displacements with EPE of 0.0914.
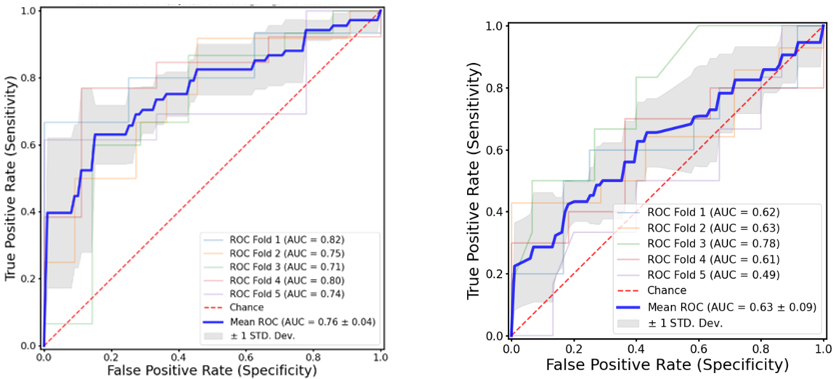
- The survival network had the average AUC value for the ROC curves of 0.76 ± 0.04
Impact: This study used important features in myocardial displacement fields. It gives better AUC in comparison with human-derived descriptors of cardiac motion. Also, there are other parameters that can be added to this model to get a promising 4-year survival prediction.
Background
Cardiac Resynchronization Therapy (CRT) improves cardiac function and prolongs survival of heart failure patients with dyssynchrony. However, a persistent challenge lies in the approximately 40% nonresponse rate. This study explores the potential of deep learning (DL) to extract latent features from myocardial displacement fields and train a classifier for the prediction of 4-year survival post-CRT 1-4. In contrast to conventional human-derived descriptors of cardiac motion, the hypothesis posits that DL-based approaches can offer superior prognostic capabilities. By leveraging advanced computational methods, this research seeks to redefine risk stratification and long-term survival prediction, providing a promising avenue for optimizing cardiac care strategies.Methods
In this study, two different models were developed. First, a 3D Convolutional Autoencoder (3D-CAE) was created to compress displacement trajectories into a low-dimensional latent code, preserving sufficient information for reconstructing the trajectories. Second, a survival network was designed to utilize latent features from three slices: the base, mid, and apex, for predicting 4-year survival post-CRT. The 3D-CAE model was trained on short-axis (SA) cine DENSE MRI data collected from 162 heart-disease patients and 136 healthy volunteers. All DENSE displacement trajectories were standardized to a 48x48 matrix in the x-y plane and spanned 48 cardiac phases through time. The autoencoder's input consisted of DENSE displacement trajectories, and the output yielded reconstructed trajectories by utilizing the extracted latent features. The network structure is shown in in Figure 1, and the mean squared error (MSE) was defined as the model's loss function. The model underwent testing on a dataset of 70 subjects, and the end-point-error (EPE) was computed to compare the input and reconstructed trajectories. This model was saved, and its encoded output was employed as a feature extraction module to provide input for the survival network. For the Survival network, data from 112 out of 130 heart failure/CRT patients were used. CMR imaging was performed prior to CRT implantation, which included short-axis DENSE imaging. Eighteen data sets were excluded because they lacked the necessary three short-axis DENSE slices, which are a prerequisite for this model. Each slice was processed through the pre-trained 3D-CAE network, with the encoder's output[FE1] serving as the input for the survival model. The Survival network incorporated 'dense + batch normalization + ReLU' layers and employed a combination of the information from the three slices at the final sigmoid layer. The network architecture is depicted in Figure 2, and the loss function employed was binary cross-entropy. The model underwent training and validation using a 5-fold cross-validation (CV) approach. Receiver operating characteristic (ROC) curves were generated for each fold within the CV, and the areas under the ROC curves (AUCs) were calculated to assess the model's performance. [FE1]Should this be “latent code” instead of “output”?Results
Figure 3A shows the ROC curves for the survival model. The average AUC value for the ROC curves was 0.76 ± 0.04. Figure 3B shows the ROC and AUCs for 5-fold validation using a logistic regression model based on the DENSE circumferential uniformity ratio estimate with singular value decomposition (CURE-SVD1 ). The AUC for the survival model was significantly higher than 0.63± 0.09 obtained by CURE-SVD. To assess the 3D-CAE network, the mean EPE of 0.0914 demonstrates very good reconstructed trajectories using 130 features.Conclusion
The 3D-CAE model trained using DENSE displacement trajectories extracted latent features (generated a compressed representation of displacement trajectories) and a survival model was subsequently trained using these latent features and known survival outcomes. These models joined together can outperform conventional models using human-derived predictor variables like CURE-SVD for 4-year survival prediction after CRT.Acknowledgements
This work was supported by R01 HL147104.References
[1] Bilchick, Kenneth C., et al. "CMR DENSE and the Seattle heart failure model inform survival and arrhythmia risk after CRT." JACC: Cardiovascular Imaging 13.4 (2020): 924-936.
[2] Gao, Xu, et al. "Cardiac magnetic resonance assessment of response to cardiac resynchronization therapy and programming strategies." JACC: Cardiovascular Imaging 14.12 (2021): 2369-2383.
[3] Bivona, Derek J., et al. "Machine learning for multidimensional response and survival after cardiac resynchronization therapy using features from cardiac magnetic resonance." Heart Rhythm O2 3.5 (2022): 542-552.
[4] Ramachandran, Raghav, et al. "Singular value decomposition applied to cardiac strain from MR imaging for selection of optimal cardiac resynchronization therapy candidates." Radiology 275.2 (2015): 413-420.
Figures