3791
Estimating right heart catheterization results from Phase-Resolved Functional Lung (PREFUL) MRI using Deep Learning1Institute of Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 2Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), German Center for Lung Research (DZL), Hannover, Germany, 3Department of Respiratory Medicine and Infectious Diseases, Hannover Medical School, Hannover, Germany
Synopsis
Keywords: Diagnosis/Prediction, Hypertension
Motivation: Right heart catheterization (RHC) is the invasive gold standard to measure several cardiopulmonary parameters. PREFUL is a non-invasive method to quantify hemodynamics during the cardiac cycle from MRI in free breathing and without contrast agents.
Goal(s): Provide an MRI-based method for non-invasive estimation of mean pulmonary arterial pressure (mPAP), pulmonary arterial wedge pressure (PAWP) and mixed venous oxygen saturation (SvO2) currently determined by RHC.
Approach: Multiple deep neural networks were trained to estimate mPAP, PAWP and SvO2 from cardiac cycles of three lung slices, provided by PREFUL.
Results: The estimations of mPAP, PAWP and SvO2 showed strong correlation with RHC.
Impact: Estimation of mPAP, PAWP and SvO2 is possible via PREFUL MRI. The presented approach is more automatized than echocardiography and may support the diagnosis of cardiopulmonary diseases such as pulmonary hypertension where RHC is not yet available.
Introduction
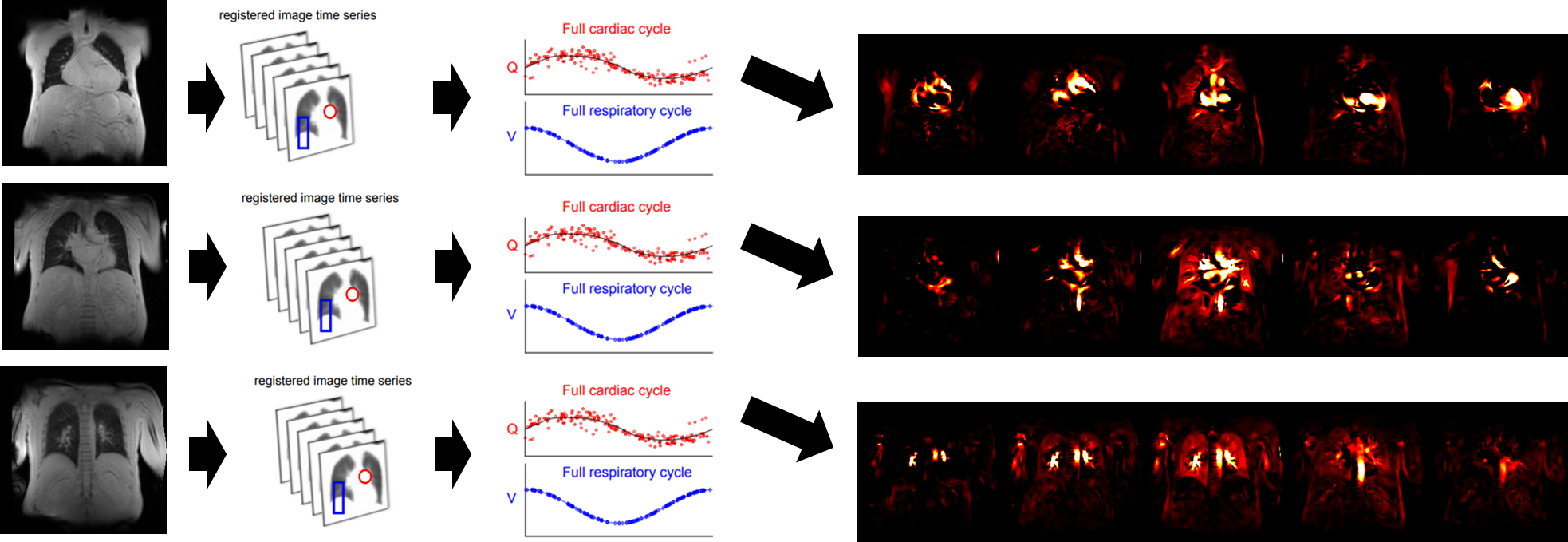
Assessment of hemodynamics, especially pulmonary arterial wedge pressure (PAWP), mixed venous oxygen saturation (SvO2) and especially mean pulmonary arterial pressure (mPAP) are important parameter to diagnose cardiopulmonary diseases such as pulmonary hypertension (PH). The clinical standard to determine these values is right heart catheterization (RHC). Echocardiography presents a non-invasive method, but tends to overestimate the pulmonary arterial pressure.1From the field of MRI, Phase-Resolved Functional Lung (PREFUL) Imaging2,3 may be installed as a non-invasive method to measure mPAP and further parameters. PREFUL enables an assessment of ventilation (represented by respiratory cycle) and perfusion (represented by cardiac cycle) of the lung and surrounding vasculature from proton MRI. As PREFUL requires neither breathing stops nor contrast media, it is a very patient-friendly method.
We introduce a Deep Learning-based approach to determine PAWP, SvO2 and mPAP from PREFUL provided cardiac cycles, which is non-invasive and more automatized than echocardiography.
Method
93 (f=48) patients with suspected PH underwent RHC and PREFUL MRI with maximum 7 days difference.PREFUL MRI was performed at 1.5T (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany) using a 2D spoiled gradient echo sequence (FoV=500x500mm slice thickness=15mm, matrix size=128x128 (256x256 interpolated), TE=0.82ms, TR=3ms, flip angle= 5°).
The fully automatized PREFUL-post-processing2,3 shown in Figure 1 visualizes the cardiac cycle represented by 15 images with matrix size 256x256.
We hypothesize that the cardiac cycle of the central coronal slice at the level of the trachea combined with the cardiac cycles of its first neighbor slice in ventral and dorsal direction contains information currently measured by RHC. Concretely, we have investigated the feasibility to estimate mPAP, PAWP and SvO2 from the cardiac cycles of three coronal lung slices.
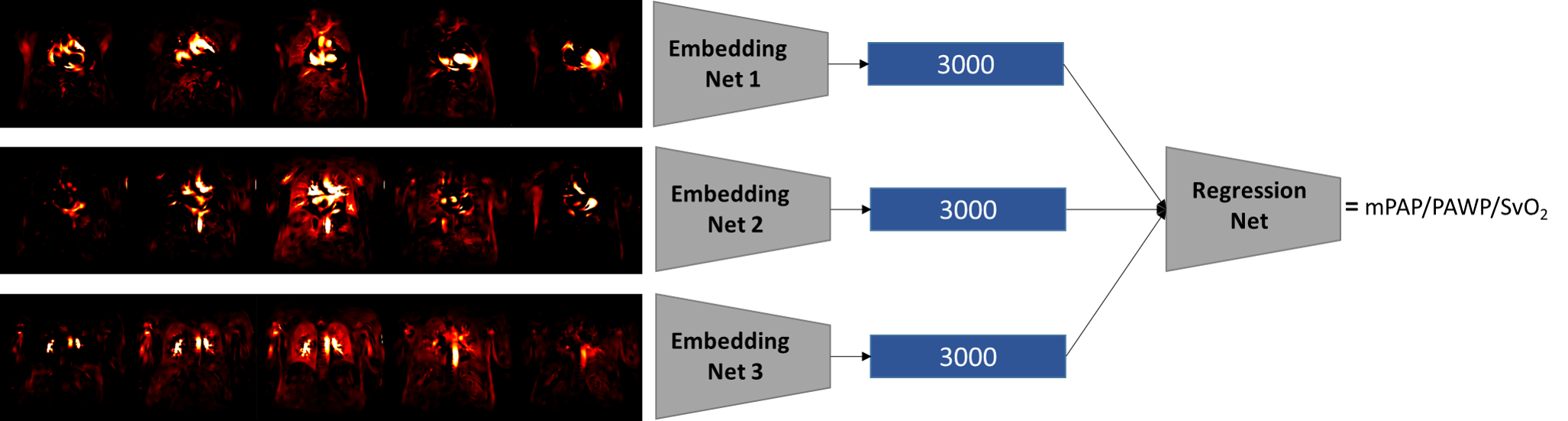
For each parameter, an artificial neural network (ANN) was trained to estimate this parameter from the cardiac cycles. The ANN consists of 4 subnetworks: Each cardiac cycle is transformed to a feature vector consisting of 3000 components. Thereby, the transformation of each lung slice is learned by a dedicated ANN. Finally, an additional ANN maps the concatenation of the resulting features to the target value. We have evaluated the architecture shown in Figure 2 with mPAP, PAWP and SvO2 as target value. All subnetworks had Densenet-264 topology (4) and were trained simultaneously with mean squared error on the ground truth given by RHC as loss function.
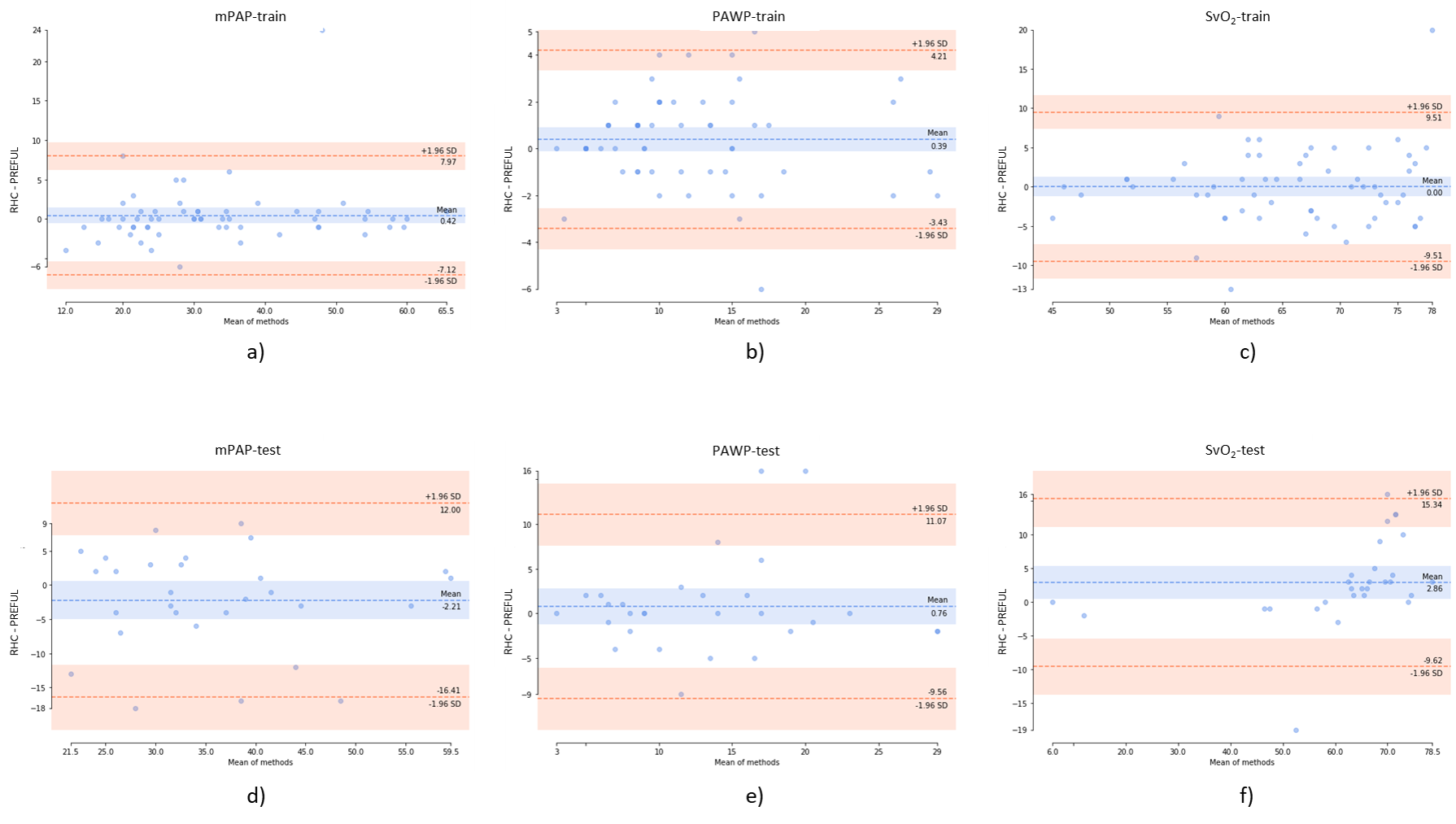
The bias of PREFUL MRI-based estimation compared to the RHC was measured using Wilcoxon-test, Pearson’s correlation and Bland-Altman plots.
Results
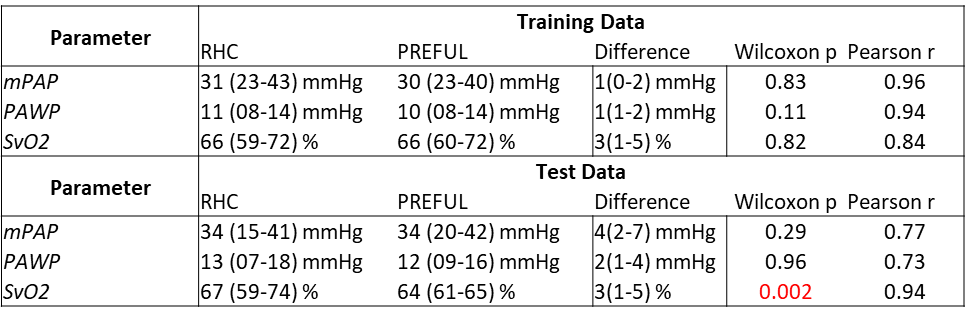
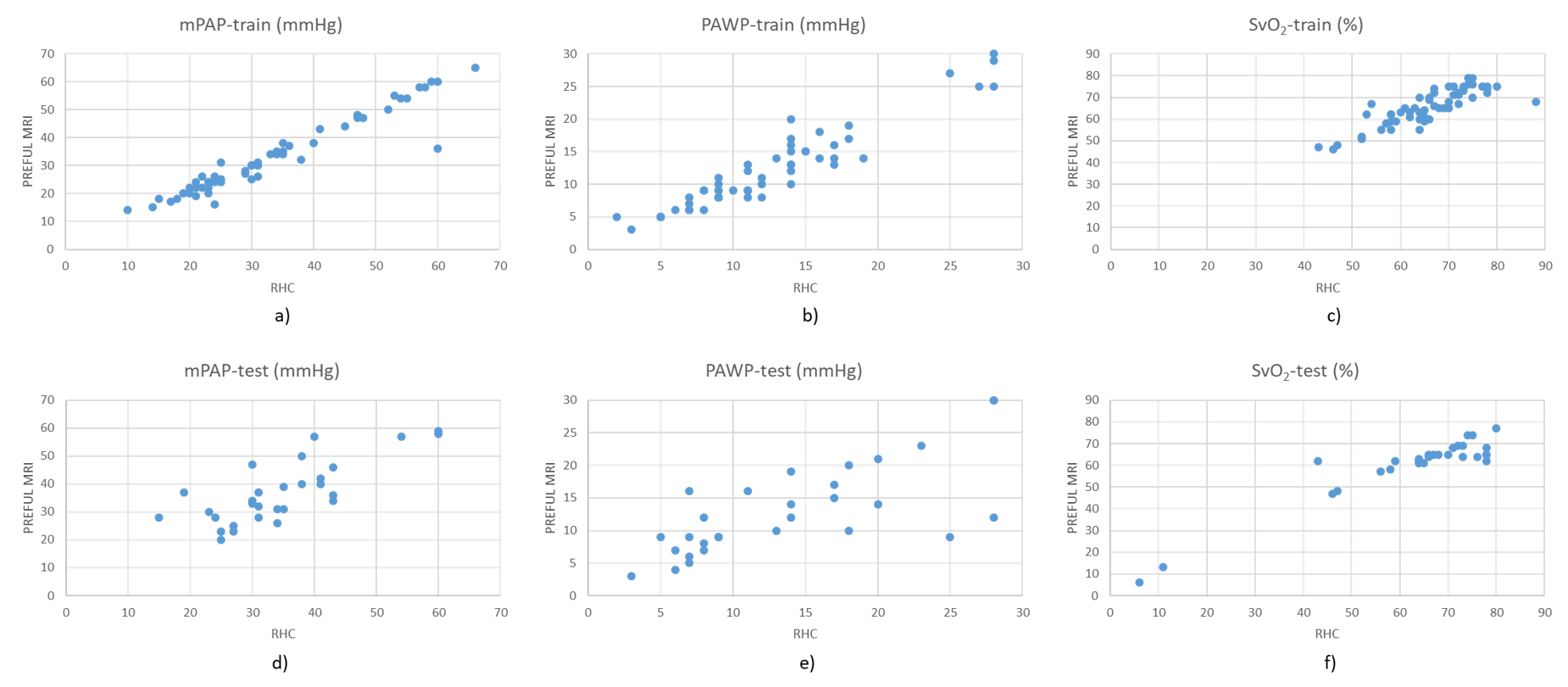
As documented in Table 1, the MRI-based estimation of mPAP and PAWP was feasible without a significant difference to RHC. For SvO2 also a strong correlation of PREFUL based estimation with RHC measurements was observed for both data sets, with a small significant systematic bias towards lower PREFUL-derived values.The almost perfect correlation of estimated mPAP, PAWP and a strong correlation of SVO2 with RHC for the training dataset is illustrated in Figure 3a-b. The corresponding test data (Figure 3d-e) showed increased variance.
The Bland-Altman plots (see Figure 4) confirmed the increased scattering of test data.
Discussion
First experiments with a small dataset demonstrated a promising precision of our approach, however, a difference to RHC remains. Therefore PREFUL-based estimation of RHC parameters may be considered as an early monitor in the future when RHC is not yet available. An mPAP >20 mmHg defines pulmonary hypertension5, an MRI-based estimation of 23 mmHg and a RHC result of 26 mmHg would probably have the same consequences for further diagnostic and treatment. On the other hand, an MRI-based estimation of 17 mmHg and an RHC results of 22 mmHg would be problematic. Therefore, RHC should not yet be replaced by the described method. Instead, the MRI-approach needs to be improved using advanced Deep Learning methods such as transformers, which, however, require larger amounts of training data.Conclusion
Deep Learning-based estimation of mPAP and PAWP showed no significant difference to the ground truth provided by RHC. For unseen test data SvO2 had the strongest correlation, but also a significant bias. Overall, the estimation of RHC parameters from PREFUL cardiac cycles seems feasible and should be further explored.Acknowledgements
No acknowledgement found.References
- Johns CS, Rajaram S, Capener DA, Oram C, Elliot C, Condliffe R, Kiely DG, Wild JM, Swift AJ. Non-invasive methods for estimating mPAP in COPD using cardiovascular magnetic resonance imaging. Eur Radiol. 2018 Apr;28(4):1438-1448. doi: 10.1007/s00330-017-5143-y. Epub 2017 Nov 16. PMID: 29147768; PMCID: PMC5834560.
- Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Schönfeld C, Rotärmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018 Apr;79(4):2306-2314. doi: 10.1002/mrm.26893. Epub 2017 Aug 30. PMID: 28856715.
- Voskrebenzev A, Gutberlet M, Kaireit TF, Wacker F, Vogel-Claussen J. Low-pass imaging of dynamic acquisitions (LIDA) with a group-oriented registration (GOREG) for proton MR imaging of lung ventilation. Magn Reson Med. 2017 Oct;78(4):1496-1505. doi: 10.1002/mrm.26526. Epub 2016 Nov 18. PMID: 27859552.
- Huang, G, Liu Z, Van Der Maaten L, Weinberger, K. Q. Densely connected convolutional networks. Proceedings of the IEEE conference on computer vision and pattern recognition. 2017.
- Humbert M, Kovacs G, Hoeper MM, Rosenkranz S et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG). European heart journal. 2022 Oct; 43(38):3618–3731. doi: 10.1093/eurheartj/ehac237
Figures