3789
High-resolution 3D aortic segmentations from standard 2D CMR localisers: an AI application to clinical care and population studies1University College London, London, United Kingdom, 2Barts Health NHS Trust, London, United Kingdom, 3Royal Free Hospital, London, United Kingdom
Synopsis
Keywords: Diagnosis/Prediction, Segmentation
Motivation: Undiagnosed aortic aneurysms can be fatal. We aim to use machine learning to measure the aorta from standard CMR localisers, allowing screening and characterisation of aneurysms without the need for additional sequences.
Goal(s): We aim to generate accurate 3D segmentations (1-1.5mm slice thickness) from standard 2D trans-axial SSFP localisers stacks (10-12mm slice thickness).
Approach: We trained an AI model using high-resolution segmentations alongside simulated low-resolution images (2D localisers). This enables the model to predict high-resolution segmentations from unseen, low-resolution images by generalising from the learned patterns.
Results: Our model shows promising performance in generating high-resolution segmentations from various unseen low-resolution validation dataset.
Impact: With our model, the dilated aorta can be identified from routine CMR scans without the need for extra sequences. Additionally, 3D aorta morphology information can be obtained from previous clinical CMR studies or population studies without additional cost.
Introduction
The identification and measurement of aortic aneurysm is an important clinical problem. While specialised high-resolution CMR sequences, 3D whole-heart sequences, allow detailed aortic assessment, they require additional sequences and are therefore time-consuming, preventing their use in routine cardiac scans and in population studies.In this work, we aimed to achieve accurate 3D measurement of aortic size in routine clinical CMR studies to allow screening and monitoring of aneurysms without the need for additional sequences. The trans-axial SSFP localisers are routinely acquired as a part of CMR study, but with a typical slice spacing of 8-12mm, they usually have low through-plane resolution. Using deep learning, we propose to create high-resolution 3D segmentations of the aorta from these low-resolution images. For evaluation, we compare the model-predicted 3D segmentations to the high-resolution segmentations from 3D whole-heart sequences acquired concurrently on the same patients. We also investigate the model test-retest reproducibility, as well as assess the quality of model-predicted high-resolution segmentation on external population data.
Methods
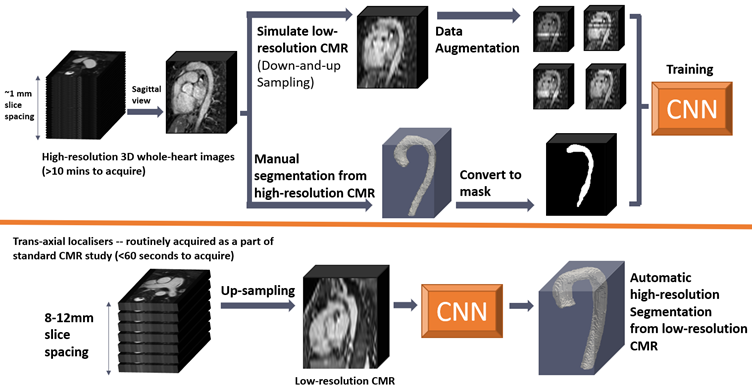
Our approach is illustrated in Figure 1. In summary,A. We acquire high-resolution 3D whole-heart images (1-2mm slice spacing; SSFP) of the heart and thoracic aorta. These SSFP images are acquired from two sources: 30 from successive consented patients from a clinical service (Royal Free Hospital, London – 1.6mm slice spacing) and 41 subjects from the MM-WHS grand challenge1 (1-2 mm slice spacing).
B. High-resolution segmentations of the aorta were manually created from the 3D whole-heart data by a clinician using Horos v4.0 (Plug-ins built in, Horosproject.org sponsored by Nimble Co LLC d/b/a Purview, Maryland, USA).
C. Simulate low-resolution trans-axial localisers: To create paired training data, we down-sampled the high-resolution 3D whole-heart images by linear interpolation, augmented them by changing the contrast of randomly selected slices (to mimic the inconsistency of contrast in 2D slices), and subsequently up-sampled them with cubic spline interpolation of several different parameters to resemble the resolution of 2D localisers of slice spacing 8-12 mm.
D. Train a neural network: Using the simulated low-resolution image (from step C) and paired with their manual high-resolution segmentations (from step B) to train a model that is capable of taking in new, unseen, low-resolution 2D slices and returns predicted high-resolution 3D aortic segmentations.
Validation
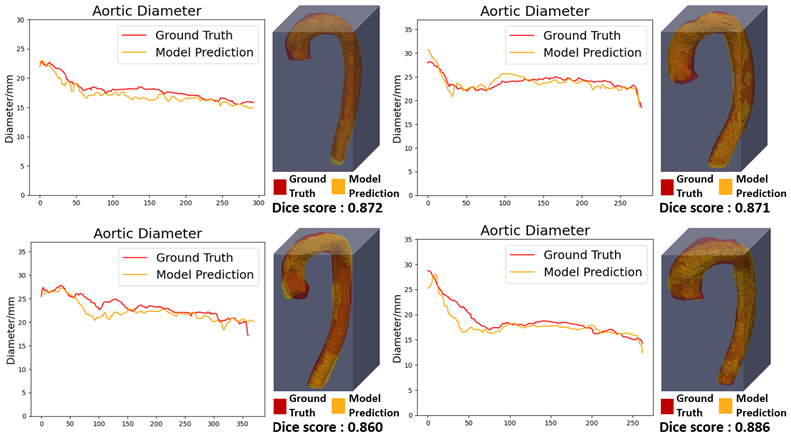
We validate the method in three ways:Quantitative validation: Both 2D localiser (10mm slice spacing) and 3D whole-heart (1-2 mm slice spacing) SSFP images were acquired concurrently on the same subject for 10 cases. The model-predicted segmentations from 2D localiser were evaluated against manual segmentations from the 3D whole-heart images using the DICE score, maximum diameter measurement, as well as a 3D visual comparison.
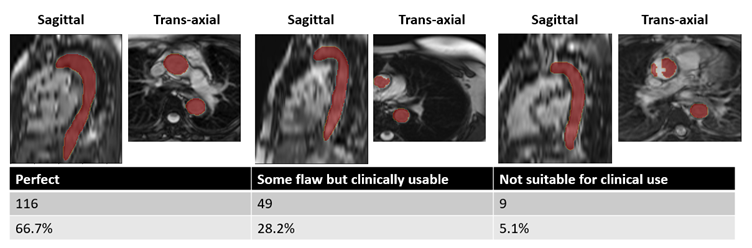
Qualitative validation of segmentation quality: the ML algorithm was run on low-resolution images from 180 subjects from the UK Biobank (12mm slice spacing), and rated by a clinician as one of (i) perfect, (ii) some flaws but clinically usable and (iii) not suitable for clinical use.
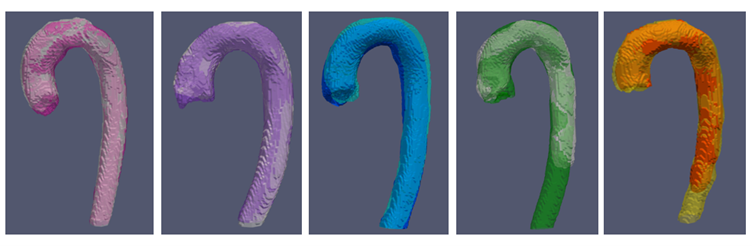
Test-retest performance: 5 subjects underwent cardiac MRI twice within the same day at Barts Heart Centre, with the predicted aortic segmentation results shown in 3D visualization. This will form the basis for a test-retest study.
Results
Quantitative analysis: Some examples of the predicted segmentations are shown in Figure 2. The high-resolution predictions were compared with high-resolution manual segmentations (considered as ground truth) and gave a mean DICE score 0.85 across all subjects. The diameters automatically measured from these 3D aortic models agreed well and 4 examples were shown in Figure 2.Qualitative analysis: Of the 180 UK Biobank segmentations, 6 were acquired without the aortic arch included in the image and thus eliminated. And of the rest 174 segmentations, 165 (95%) were deemed 'usable for clinical use' (116 very good; 49 some flaws, but clinically usable), only 9 (5%) subjects deemed 'clinically unusable' (See figure 3).
Test-retest performance: Visualisation of the test-retest pairs are shown in figure 4.
Discussion
The model shows a good overall performance. And it is applicable to several unseen validation dataset (UK Biobank, Barts), implying a great robustness to generalise well to 2D localisers of various thickness. The process of generating 3D aortic segmentation is fully automated, finished within seconds, and offers extra information for clinically use without requiring extra acquisition time/effort.Conclusion
We have described a method of producing high-resolution aortic segmentations from standard CMR planning images. We have shown the method to be accurate and reproducible, allowing routine screening of aortic aneurysm in clinical care and for establishing normal ranges of variation in large-scale population studies.Acknowledgements
No acknowledgement found.References
1. Xiahai Zhuang: Multivariate mixture model for myocardial segmentation combining multi-source images. IEEE Transactions on Pattern Analysis and Machine Intelligence 41(12): 2933-2946, 2019.Figures