3784
Machine learning based characterisation of glioma shows best performance with post-contrast T1 and diffusion imaging1Department of Medical Physics and Biomedical Engineering, University College London, London, United Kingdom, 2Department of Biomedicine and Prevention, University of Rome Tor Vergata, Rome, Italy, 3Department of Surgery and Cancer, Imperial College London, London, United Kingdom, 4Precision Imaging Beacon, Medical School, University of Nottingham, Nottingham, United Kingdom, 5Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, United Kingdom, 6Radiology Department, Queen’s Medical Centre, Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom, 7Department of Brain Rehabilitation and Repair, Institute of Neurology, University College London, London, United Kingdom, 8Lysholm Department of Neuroradiology, National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, United Kingdom, 9Department of Computer Science, University College London, London, United Kingdom
Synopsis
Keywords: Diagnosis/Prediction, Tumor, Neuro-oncology
Motivation: Accurate glioma classification currently relies on tissue diagnosis, which has associated surgical risks. Machine learning based classification of MR images may enable non-invasive glioma characterisation.
Goal(s): Our aim was to assess which imaging modalities provided optimal training data to increase accuracy of machine learning based glioma characterisation.
Approach: A pyRadiomics based pipeline predicted tumour grade and IDH-mutation status with XGBoost on a glioblastoma-rich dataset. 10 structural and advanced MR acquisitions were used as model input and a systematic search for the most informative MR modalities was performed.
Results: The classifier performed best when the model was trained on post-contrast T1 and diffusion imaging.
Impact: We found post-contrast T1 and diffusion imaging to be the most informative MR modalities for machine learning based glioma characterisation. This result will benefit scientists in making well-informed choices on how to train their machine learning models for glioma classification.
Introduction
Gliomas are the most common type of malignant brain tumours. Tumour grading and genotyping is essential for guiding treatment and to predict prognosis. Accurate glioma classification relies on tissue diagnosis, which has associated surgical risks, takes time and is not feasible in all patients. XGBoost is one of many machine learning algorithms currently available to perform classification tasks from MR images, potentially enabeling non-invasive glioma characterisation. Choosing the optimal MR modality and best region of interest for feature extraction to maximize model performance remains an empirical question. A recently published dataset [1] contains glioma segmentations for structural and advanced MR acquisitions (Diffusion, SWI, ASL), presenting an opportunity for a systematic search of ideal model inputs. Our aim was to assess which tumour regions and which imaging modalities provided the best accuracy for untreated glioma characterisation.Methods
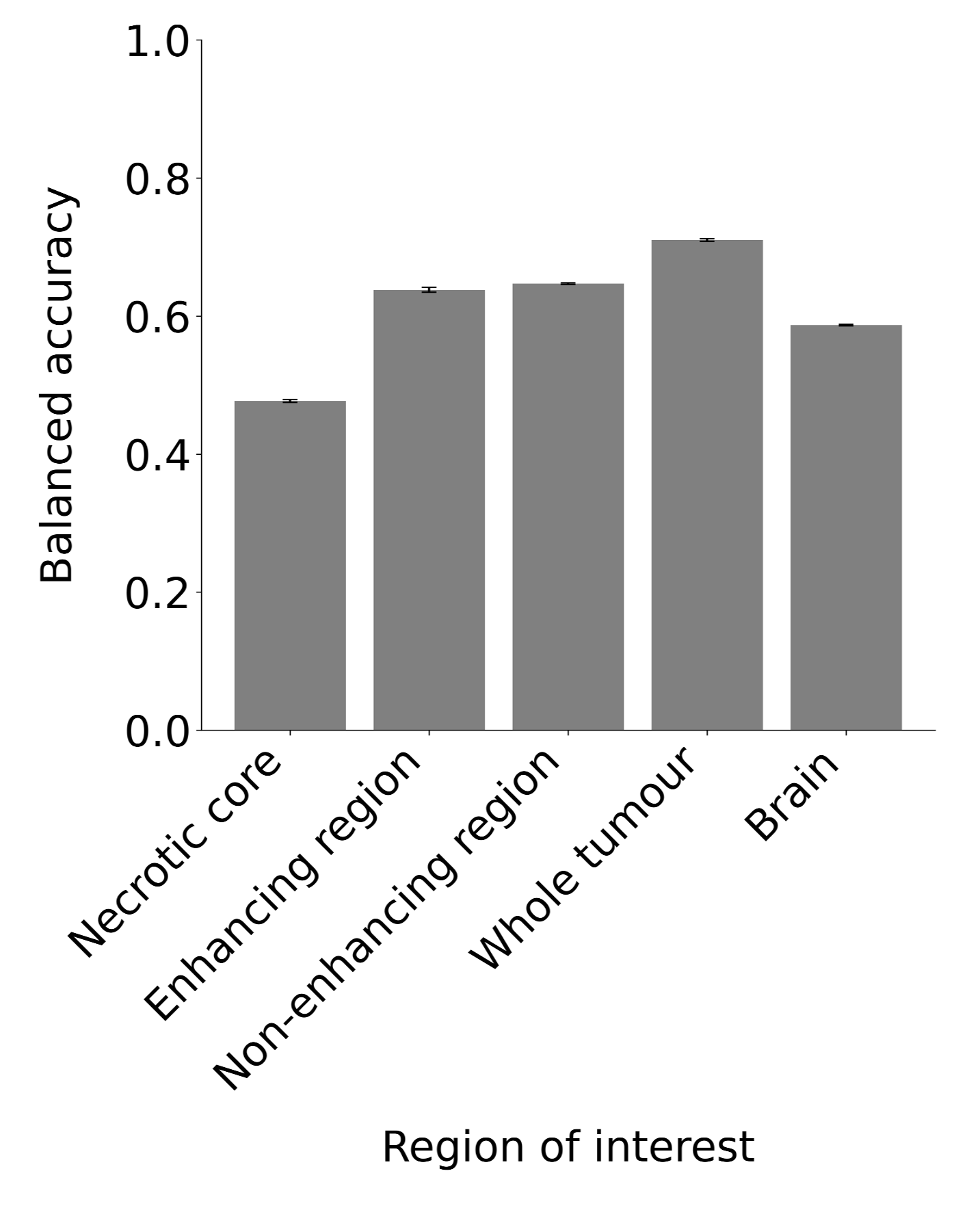
The cleaned dataset comprised of 493 glioma patients, of which 56 (11%) were diagnosed with WHO grade 2, 43 (9%) with WHO grade 3, and 394 (80%) with WHO grade 4. The IDH mutation was present in 103 patients (21%). The dataset was divided into 80% for training, and 10% for each validation and testing, while stratifying the groups along the dimensions 1) IDH status, and 2) WHO Grade. A pyRadiomics based pipeline was set up on a high-performance computing cluster to extract 18 first-order features from 10 structural and advanced MR acquisitions (pre-contrast T1, T2, post- contrast T1, FLAIR, SWI, ASL, DWI, ADC, DTI fractional anisotropy and mean diffusivity). XGBoost classifiers were trained on all extracted first-order features, along with basic clinical information (sex and age) to predict WHO grade (grade 2, 3 or 4) and isocitrate dehydrogenase (IDH) mutation status (wildtype or mutant) with all possible combinations of the 10 modalities as input. First-order features have been separately extracted from the necrotic core, the enhancing region, the non-enhancing region, the whole tumour, and the whole brain, whereby the whole tumour is defined as necrotic core + enhancing region + non-enhancing region.Results
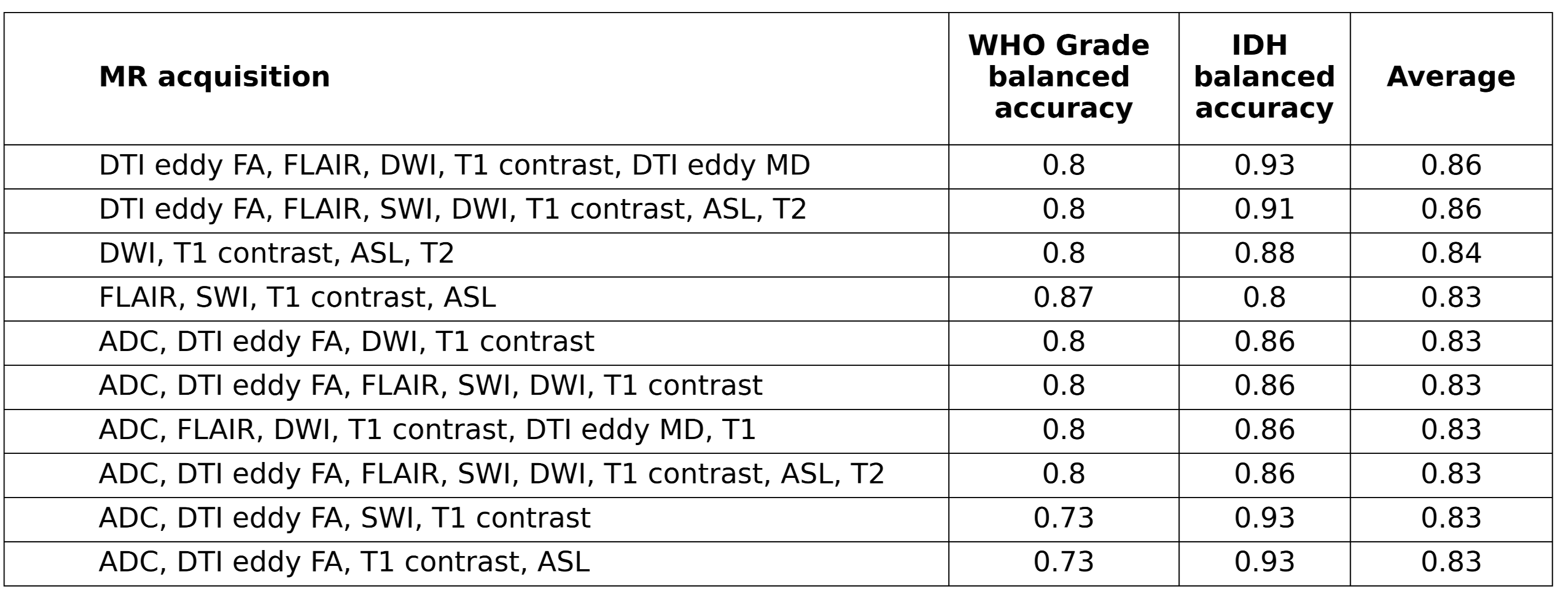
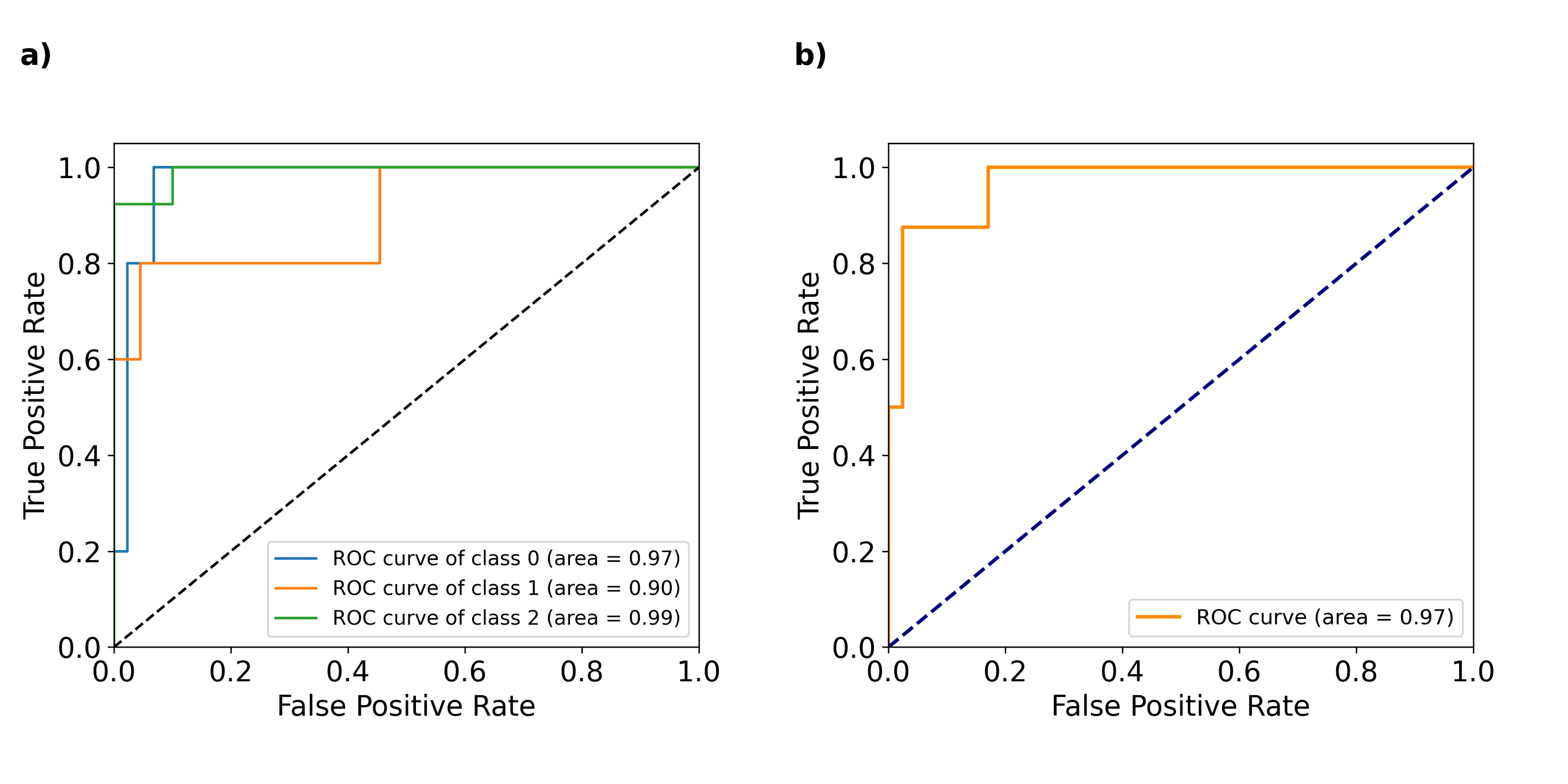
The XGBoost classifier performed best when features were extracted from the whole tumour (Fig. 1). The modalities that were used for the best performing models are post-contrast T1 (used in 10 / top 10 models), DWI (used in 8 / top 10 models), DTI fractional anisotropy, FLAIR, SWI, and ADC (all used in 6 / top 10 models). The best performing model was trained on first-order features from DTI FA, FLAIR, DWI, post-contrast T1 and DTI MD, and achieved a balanced accuracy of 0.8 for WHO grade prediction and of 0.93 for IDH status prediction (Table 1). The area under the receiver operating characteristic curve (AUC ROC) is 0.98 for differentiating WHO grade 2 gliomas against the other two grades, 0.90 to predict grade 3 tumours and 0.99 for grade 4 gliomas (Fig. 2, panel a). For the classification of the IDH mutation status the AUC ROC is 0.96 (Fig. 2, panel b).Discussion
Our study demonstrates how the XGBoost algorithm can effectively predict the WHO grade and IDH mutation status in gliomas using first-order features extracted from MR images. The most informative data appeared to come from post-contrast T1 and diffusion imaging, with features extracted from the whole tumour yielding the highest accuracy. The significant number of models that were trained, however, comes with the risk of overfitting the model on the validation set. Also, while our validation scores are promising, further research should investigate how these models perform on completely unseen data. Additionally, future studies might want to explore how accuracy can be improved by the incorporation of more clinical and genetic data into the model.Conclusion
Our study suggests that XGBoost can provide meaningful insights for glioma characterisation, especially when trained on post-contrast T1 and diffusion imaging from the whole tumour. However, future work is required to assess the model’s performance on unseen data.Acknowledgements
No acknowledgement found.References
[1] E. Calabrese et al., ‘The University of California San Francisco Preoperative Diffuse Glioma MRI (UCSF- PDGM)’. The Cancer Imaging Archive, 2022. doi: 10.7937/TCIA.BDGF-8V37.Figures