3783
Utilizing 2D UNet with Synthetic Attention for Enhanced Classification of IDH Mutations Based on Anatomical MRI in Gliomas1Institute of Biomedical Engineering, Bogazici University, Istanbul, Turkey
Synopsis
Keywords: AI/ML Software, Brain, Deep Learning, Attention
Motivation: There is a need to preoperatively assess the isocitrate dehydrogenase (IDH) mutational status in gliomas, which highly affects the treatment planning and patient prognosis.
Goal(s): To develop a robust deep learning pipeline for noninvasively assessing the IDH mutational status of gliomas based on anatomical MRI
Approach: Post-contrast T1-weighted, T2-weighted, and fluid-attenuated inversion recovery (FLAIR) MRI of 501 adult diffuse gliomas (103 IDH-mutant, 308 IDH-wildtype) of the UCSF-PGDM dataset were evaluated with a 2D UNet architecture using synthetic attention.
Results: The model utilizing all three anatomical modalities achieved an accuracy of 93.31% (sensitivity=93.33%, specificity=93.24%).
Impact: IDH mutational status in gliomas was identified with over 93% accuracy utilizing a 2D UNet architecture with synthetic attention for the evaluation of whole tumor slices of three standard anatomical MRI modalities.
Background and Purpose
Intrinsic molecular characteristics like isocitrate dehydrogenase (IDH) mutation are increasingly becoming pivotal in understanding the biology of gliomas. The World Health Organization (WHO) 2021 central nervous system tumor classification identified three distinct adult-type diffuse glioma subgroups as, glioblastoma, IDH-wildtype; astrocytoma, IDH-mutant; and oligodendroglioma, IDH-mutant and 1p/19q codeleted1. IDH mutation is known to have an effect on the treatment response and overall survival of gliomas2-4. Identification of the IDH mutation using T1-weighted (T1c), T2-weighted (T2w), and fluid-attenuated inversion recovery (FLAIR) MRI modalities has emerged as a preoperative, non-invasive approach5-7. Especially, T2-FLAIR mismatch sign has been identified as a sensitive marker of IDH-mutant, 1p/19q non-codeleted low-grade astrocytoma8. The purpose of this study is to develop a 2D UNet architecture with synthetic attention to identify IDH mutation in gliomas based on three standard anatomical MRI modalities.Methods
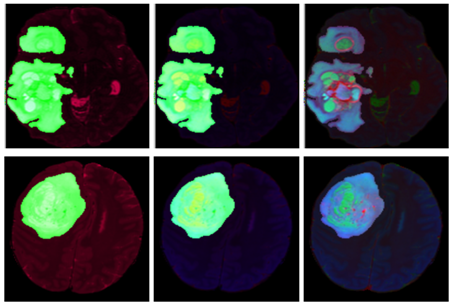
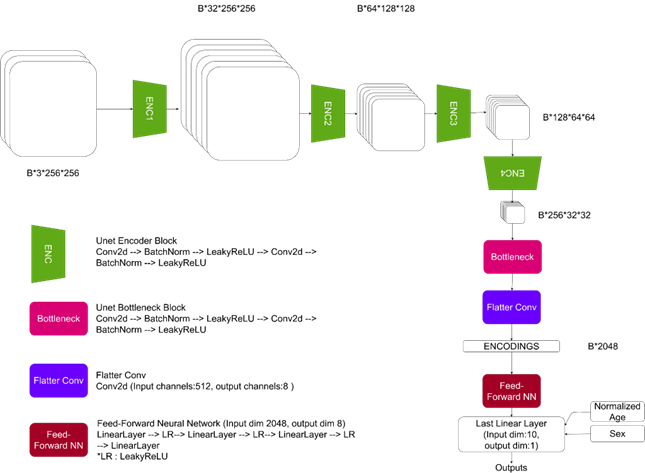
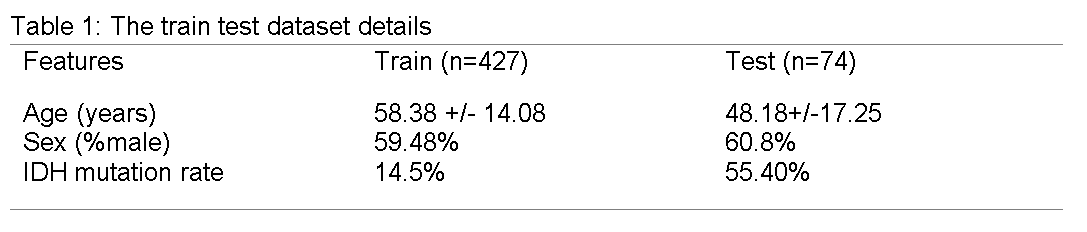
The patient cohort included presurgical MRI data of 501 gliomas (age range: 17-94 years, mean age: 56.87±15.02 years, 299M/202F, 103 IDH-mutant, 398 IDH-wildtype) that are a part of The University of California San Francisco Preoperative Diffuse Glioma MRI (UCSF-PDGM) dataset9. The IDH mutational status was assessed by histopathological analysis. MRI data were acquired at a clinical 3T MR scanner (Discovery 750, GE Healthcare, Waukesha, WI) with a brain tumor imaging protocol including post-contrast T1-weighted (T1c) inversion-recovery spoiled gradient echo (IR-SPGR) (TR/TE= 6/2.3 ms, TI= 450 ms, flip angle=12º, matrix=256×256, FOV=25.6 cm), T2-weighted (T2w) 3D fast spin echo (FSE) (TR/TE= 200/100 ms, matrix=256×256, FOV=25.6 cm) and fluid-attenuated inversion recovery (FLAIR) MRI (TR/TE= 5700/115 ms, TI= 1650 ms, matrix=256×256, FOV=25.6 cm). The details of image processing for the UCSF-PDGM dataset are provided in its reference9.For each patient, one tumor region mask was created by combining the enhancing tumor, edema and necrosis segmentation masks provided within the UCSF-PDGM dataset. A synthetic attention mechanism was added to create soft-filtered MR images by attenuating the signal intensities outside the tumor region through multiplication with a factor of 0.3. This study employed three different data fusion approaches to evaluate the IDH mutational status based on all the tumor slices (Figure 1). The first model placed the soft-filtered T1c, soft-filtered FLAIR, and soft-filtered T2w MRI at the RGB channels for each slice. On the other hand, the second model placed the tumor mask, soft-filtered T2w MRI, and soft-filtered FLAIR, while the third model placed the T2w MRI, tumor mask, and soft-filtered T2w MRI at the RGB channels. The deep learning pipeline consisted of an encoding component using a 2D UNet encoder, followed by a feed-forward neural network to evaluate the resultant encodings (Figure 2). The preprocessing steps included z-score normalization and the cropping of the black regions to focus on the brain. Normalization was applied to each channel separately. Furthermore, training and testing sets were partitioned on a per-subject basis, to prevent data leakage. The data splitting details are shown in Table 1. Normalized age -divided by 100- and sex information -m:1, f:0- were also added to the last linear layer of the model to enhance its performance.Results
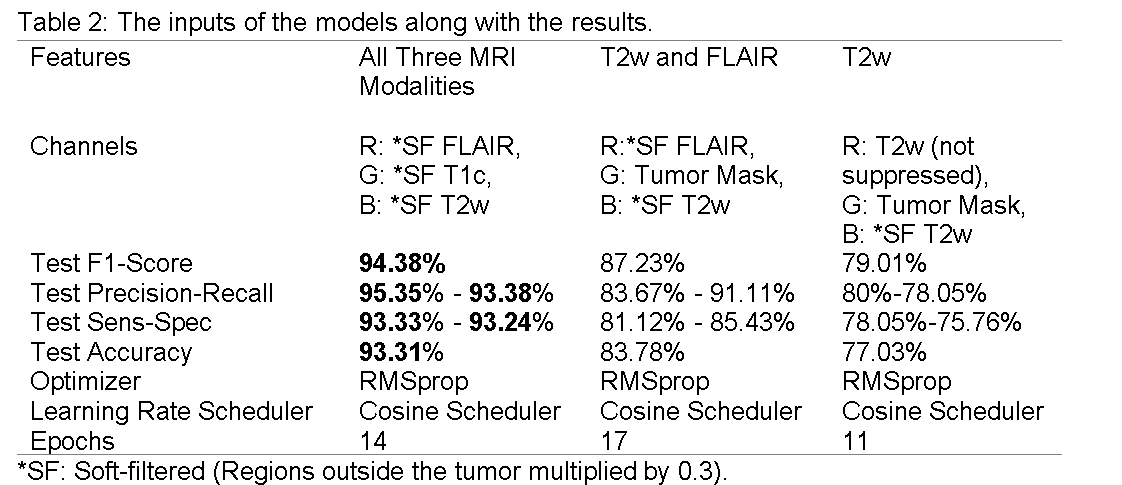
The first model based on all three MRI modalities achieved an accuracy of 93.31% (sensitivity=93.33%, specificity=93.24%, F1-score=94.38%, precision=95.45%, recall=93.33%) on the test set (Table 2). The second model that utilized both T2w and FLAIR MRI achieved an accuracy of 83% (sensitivity=81.12%, specificity= 85.43%, F1-score=87.23%, precision=83.67%, recall=91.11%). On the other hand, the last model utilizing only T2w MRI achieved a lower accuracy of 77.03% (sensitivity=75.76%, specificity=78.05%, F1-score=79.01%, precision=80%, recall=78.05%).Discussion and Conclusion
This study developed a 2D UNet-based deep learning model supported by synthetic attention to identify IDH mutation in gliomas based on commonly acquired anatomical MRI data. The best-performing model inherently took into account the T2-FLAIR mismatch effect along with the contrast enhancement. Future studies will incorporate rCBV maps to enhance the performance of our deep learning model for identifying IDH mutations in gliomas.Acknowledgements
This study was supported by TUBITAK 1003 grant 216S432.References
1. Louis, D.N., et al., The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol, 2021. 23(8): p. 1231-1251.
2. Labussiere, M., et al., Combined analysis of TERT, EGFR, and IDH status defines distinct prognostic glioblastoma classes. Neurology, 2014. 83(13): p. 1200-6.
3. Eckel-Passow, J.E., et al., Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. N Engl J Med, 2015. 372(26): p. 2499-508.
4. Killela, P.J., et al., Mutations in IDH1, IDH2, and in the TERT promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget, 2014. 5(6): p. 1515-25.
5. Sahil, N., et al., Classification of brain tumor isocitrate dehydrogenase status using MRI and deep learning. Journal of Medical Imaging, 2019. 6(4): p. 046003.
6. Chang, K., et al., Residual Convolutional Neural Network for the Determination of IDH Status in Low- and High-Grade Gliomas from MR Imaging. Clinical Cancer Research, 2018. 24(5): p. 1073-1081.
7. Pasquini, L., et al. Deep Learning Can Differentiate IDH-Mutant from IDH-Wild GBM. Journal of Personalized Medicine, 2021. 11, DOI: 10.3390/jpm11040290.
8. Foltyn, M., et al., T2/FLAIR-mismatch sign for noninvasive detection of IDH-mutant 1p/19q non-codeleted gliomas: validity and pathophysiology. Neuro-Oncology Advances, 2020. 2(1): p. vdaa004.
9. Calabrese, E., et al., The University of California San Francisco Preoperative Diffuse Glioma MRI Dataset. Radiology: Artificial Intelligence, 2022. 4(6): p. e220058.
Figures