3781
Deep learning radiomics nomograms predict IDH genotype in glioma patients: a multicenter study1Lanzhou University Second Hospital, Lanzhou, China, 2Philips Healthcare, Xi’an, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics, glioma, deep learning radiomics nomograms
Motivation: It is unclear whether deep learning radiomics nomograms (DLRN) can noninvasively predict isocitrate dehydrogenase (IDH) genotypes in glioma patients.
Goal To explore the feasibility of DLRN in predicting IDH genotype.
Goal(s): To explore the feasibility of DLRN in predicting IDH genotype.
Approach: T2WI-based DLRN was developed and validated in two centers (Center I, n=342 and Center II, n=60) to predict IDH genotype and evaluate its association with prognosis in glioma patients.
Results: The proposed model had an area under the curve(AUC)of 0.98 in an externally validated cohort, and DLRN scores were significantly associated with the overall survival of glioma patients.
Impact: The proposed DLRN can accurately predict IDH genotypes and provide a useful tool for targeted therapy of patients with IDH mutations.
Introduction
Isocitrate dehydrogenase (IDH) is the most crucial driver gene in adult diffuse gliomas, and its mutational status is the most important biomarker for the clinical management and prognosis of glioma patients. Previous studies have demonstrated that among glioma patients with preoperative Karnofsky performance score(KPS)>80 and age >45 years, the influence of the extent of surgical resection on patient prognosis is contingent upon different molecular subtypes.1,2 Therefore, it is crucial to accurately predict the IDH genotype for patient prognosis and clinically targeted therapy. However, assessing IDH mutation status using conventional MRI images remains challenging. In recent years, the deep learning radiomics model has been one of the more advanced quantitative classification models. However, there are few reports on the feasibility of predicting IDH genotype in glioma patients3,4. Therefore, our study aims to explore the capability of DLRN in predicting glioma IDH genotype and to further analyze the relationship between DLRN and prognosis of glioma patients.Methods
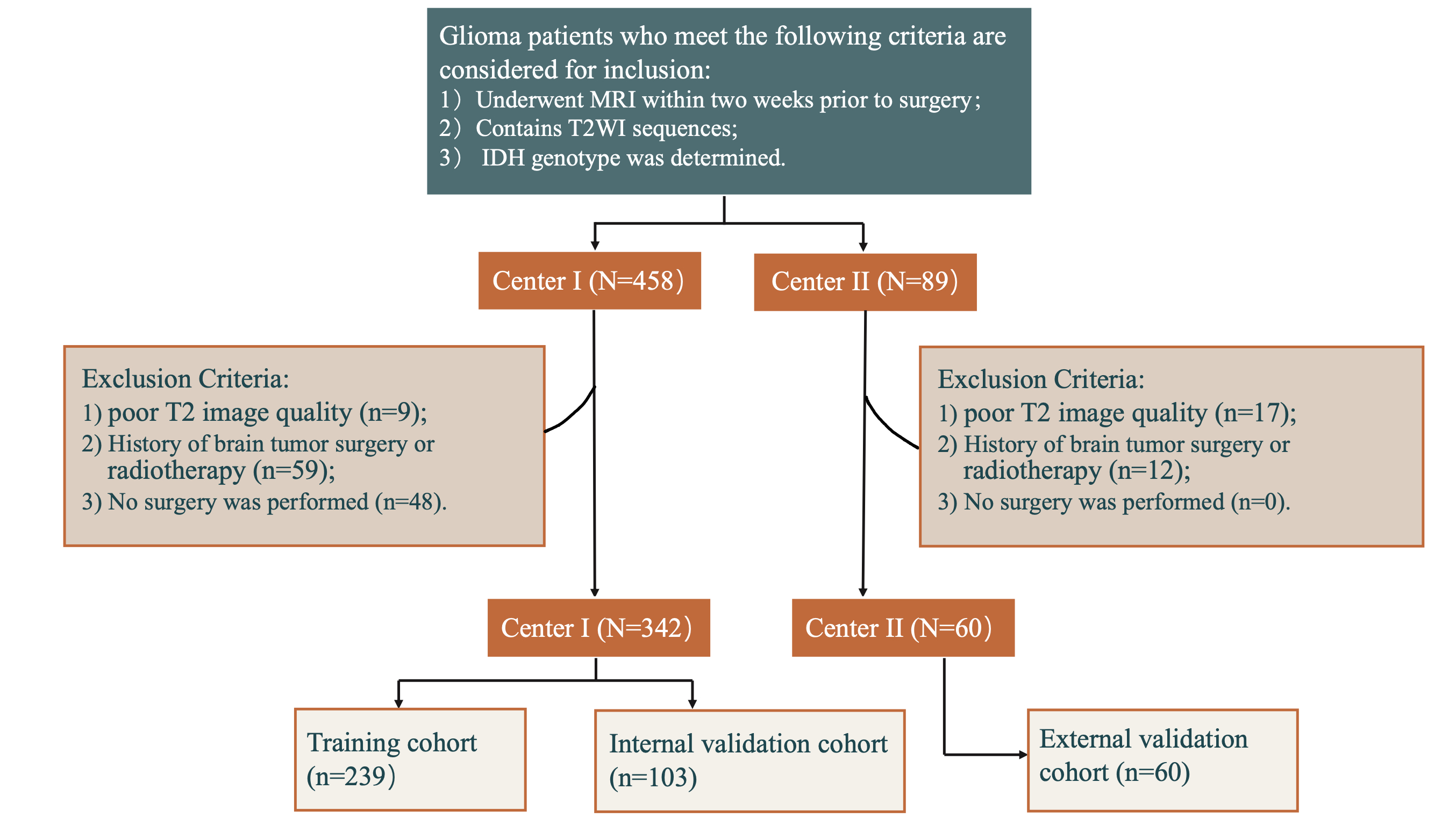
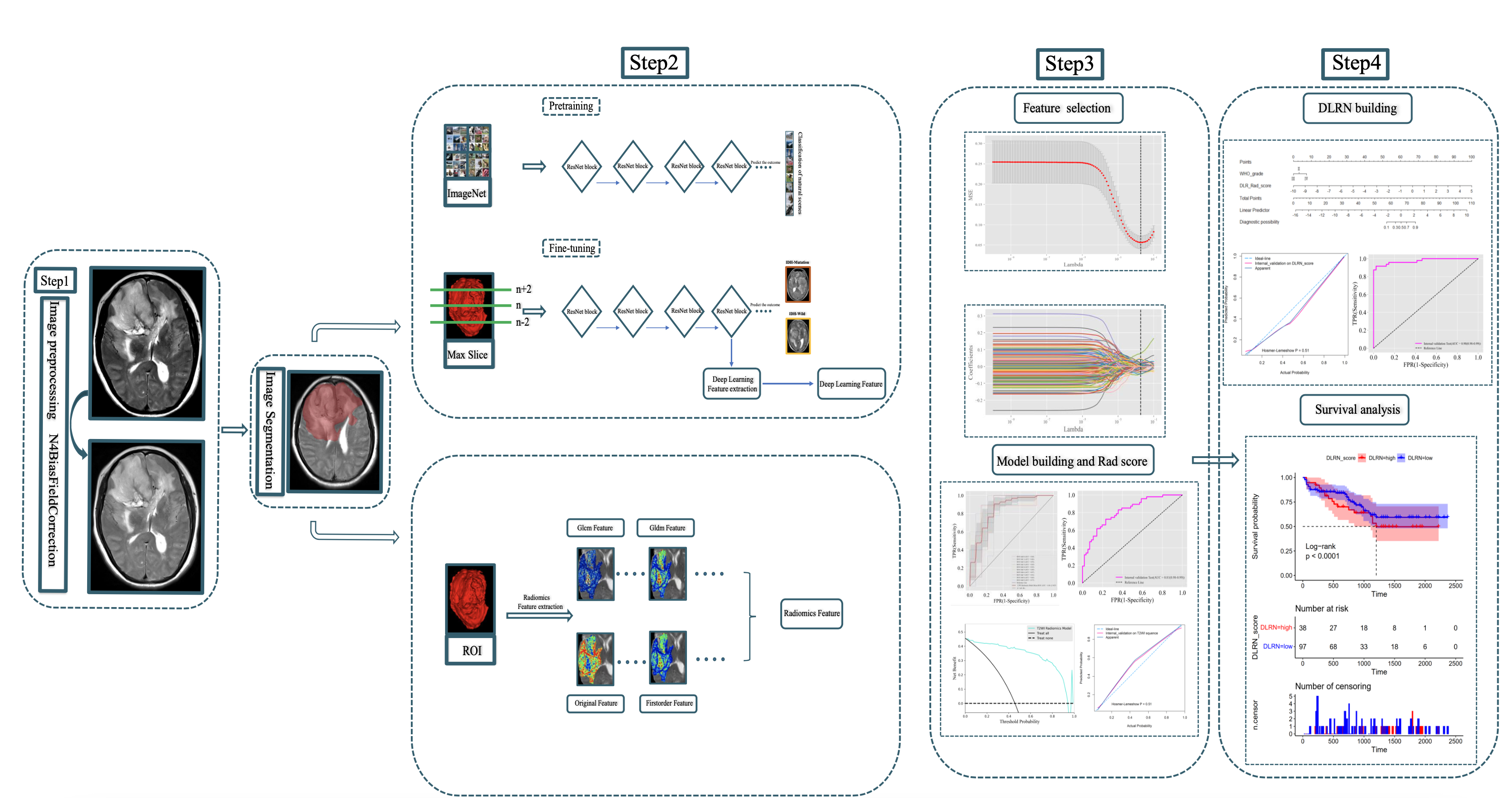
This study retrospectively analyzed 402 glioma patients from two independent centers from June 2019 to June 2023, with Center I (n=342) randomly divided at 7:3 into a training cohort (n=239) and an internal validation cohort (n=103) and Center II (n=60) as an external validation cohort. Figure 1 is a flowchart of patient enrollment.All DICOM images were resampled to 1×1×1mm3 voxel size after N4 bias field correction. After normalizing the signal intensity, all images were uniformly saved as NIfTI format. The segmentation of the tumor, which included the tumor core and the peritumoral edema area, was done by a radiologist with five years of experience and subsequently validated and determined by two senior radiologists.
Pyradiomics software was used to extract radiomics features based on T2WI images, and 107 features were extracted for each patient. In addition, we fine-tuned the ResNet101 pre-trained model based on the ImageNet dataset. We extracted the deep learning features (DLF) of the last convolutional layer after retaining the optimal weight parameters. A total of 512 DLF were extracted. The flowchart of feature extraction is shown in Figure 2.
Based on the datasets of radiomics features (RF) and DLF, we used the LASSO method to screen the features and subsequently used the support vector machine algorithm to construct the radiomics model based on 6 RF features and the DLF model based on 60 DLF, respectively. Then, we fused DLF and RF, and screened features using hierarchical clustering, followed by the support vector machine algorithm to construct and compute deep learning radiomics scores. Finally, we used multivariate Logistics regression to build the DLRN model. The diagnostic efficacy of the model was assessed using AUC. Furthermore, we analyzed the relationship between DLRN score and overall survival (OS) in selected follow-up patients using KaplaneMeier curves. All statistical analyses were done by Python 3.7 and R v4.2, and P<0.05 was considered a statistically significant difference.
Results
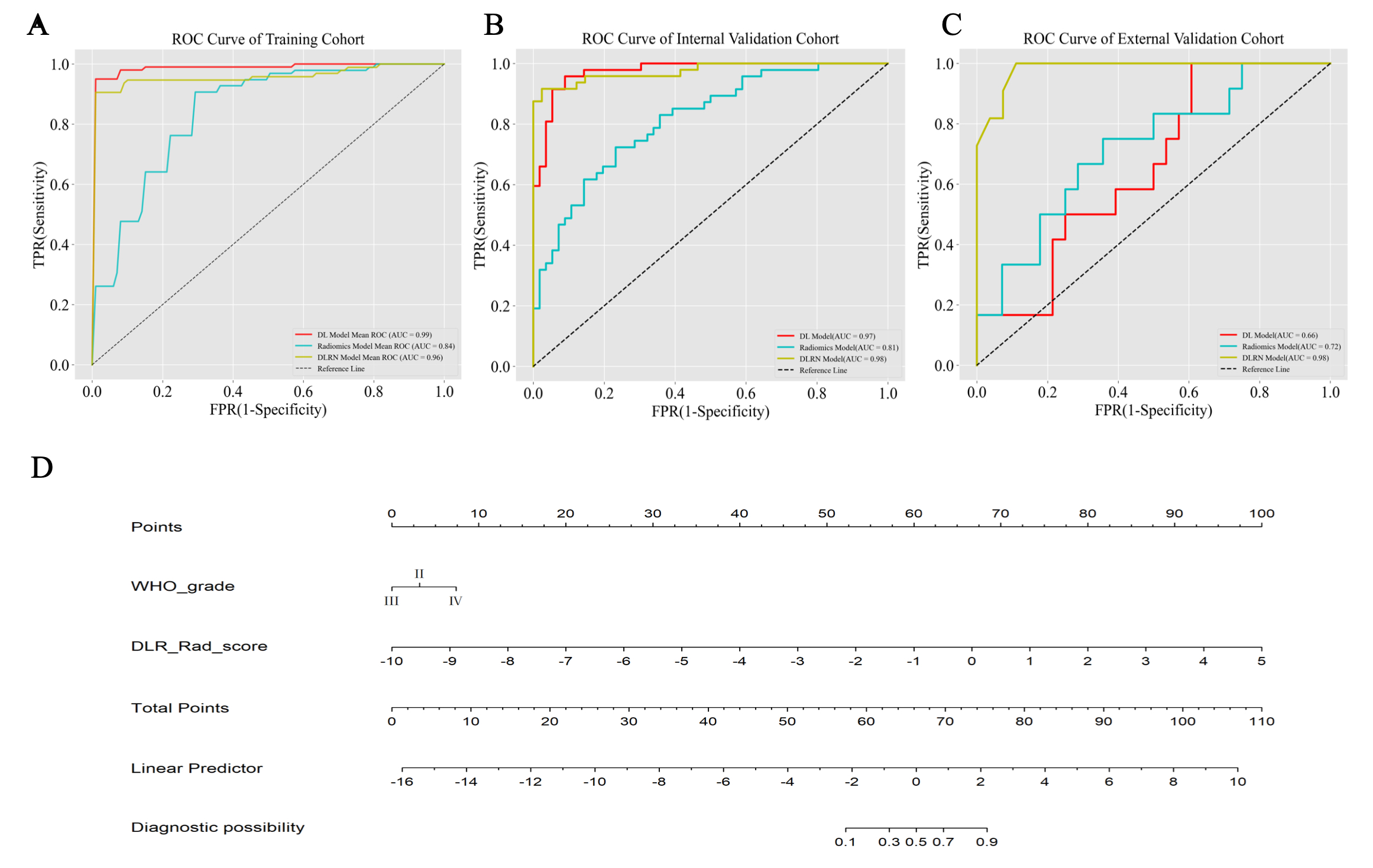
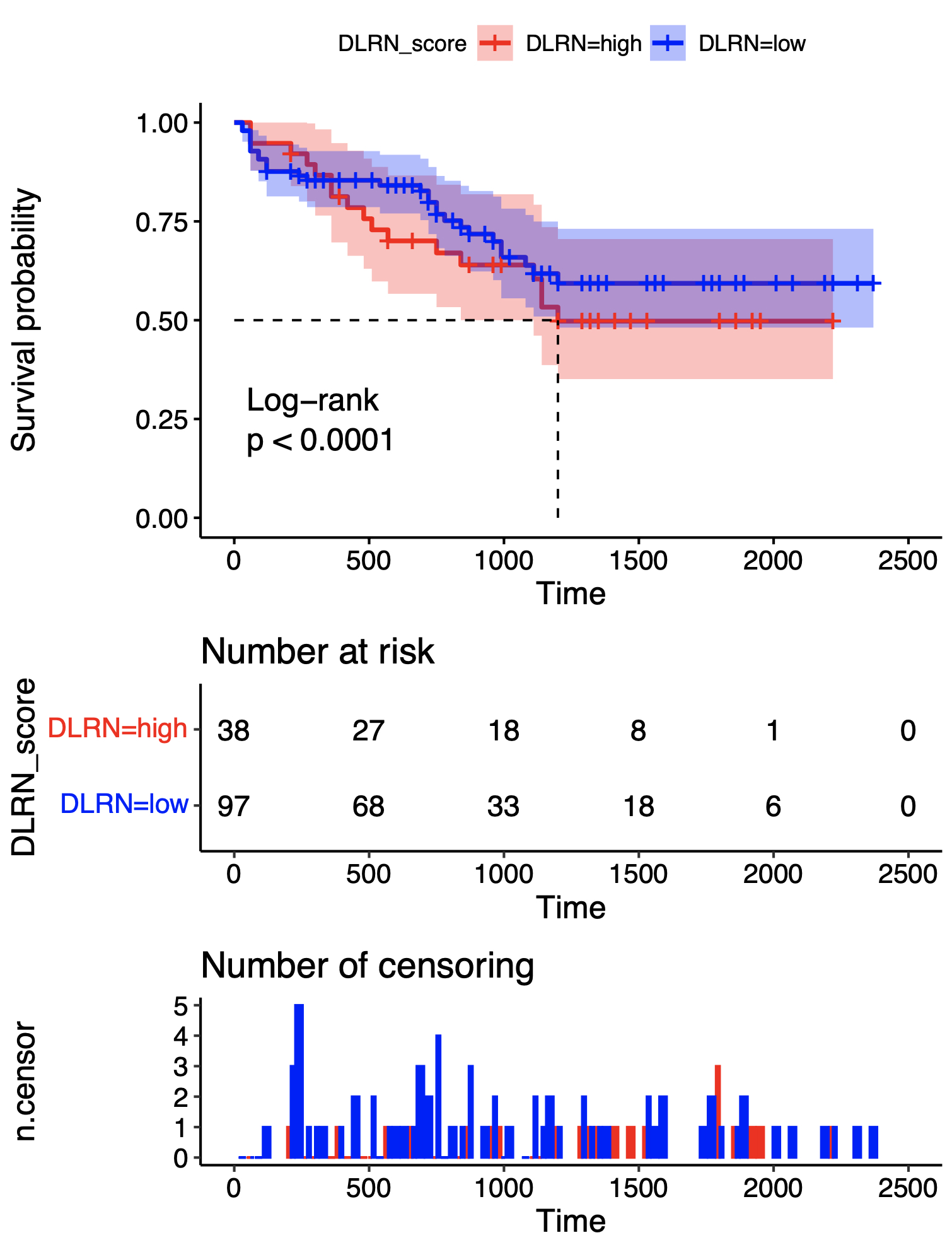
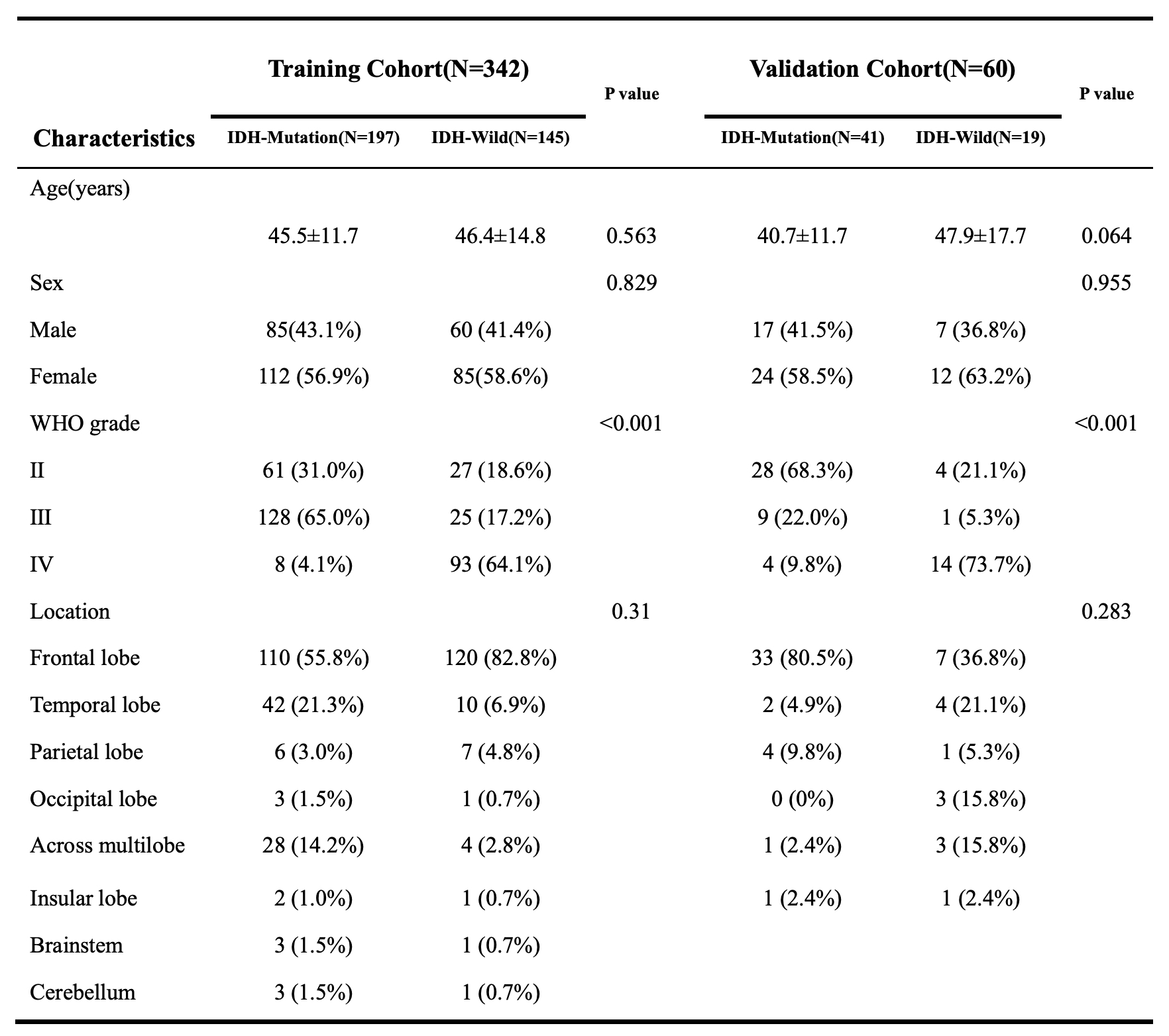
The clinical data of the patients is shown in Table 1. The AUCs of the RF, DLF, and DLRN models in the external validation cohort were 0.66 (95% CI:0.63-0.69), 0.72 (95% CI:0.70-0.75), and 0.98 (95% CI:0.95-0.99), respectively (Fig. 3). Moreover, our results showed that patients with higher DLRN scores had lower OS (Log-Rank p<0.0001)(Fig. 4).Discussion
In this study, we used a fine-tuned ResNet101 model to extract the DLF. Although the radiomics model based on the DLF did not achieve the best diagnostic efficacy, it performed well in predicting IDH genotypes. Besides, we initially screened features and constructed RF and DLF radiomics models using the LASSO method, but the results showed that this method suffers from feature redundancy and multicollinearity problems. Therefore, we used a hierarchical clustering approach in constructing the DLRN, and the results confirmed that this approach was more effective in predicting IDH genotypes.In order to balance the contribution of RF and DLF to the prediction model, Calabrese E et al. averaged the prediction probabilities of the two, and the combined model showed better performance in most situations when compared to the RF and DLF models 5. In contrast, we combined the RF and DLF and built the final classification model using multivariate Logistic analysis. The results show our model remained robust in a multicenter independent external validation cohort. Moreover, we found that DLRN score was inversely associated with overall survival in patients with glioma.
Conclusion
Our study confirms that DLRN can effectively predict glioma IDH genotypes, which not only provides a non-invasive method for preoperative prediction of IDH mutation status but also provides additional options for patients with inconclusive or inoperable pathology.Acknowledgements
No acknowledgement found.References
1. Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary [J]. Neuro-Oncology, 2021,23(8): 1231-1251.
2. Hou Z, Zhang K, Liu X, et al. Molecular subtype impacts surgical resection in low-grade gliomas: A Chinese Glioma Genome Atlas database analysis [J]. Cancer Lett, 2021,522: 14-21.
3. Zhang H, Zhang H, Zhang Y, et al. Deep Learning Radiomics for the Assessment of Telomerase Reverse Transcriptase Promoter Mutation Status in Patients With Glioblastoma Using Multiparametric MRI [J]. J Magn Reson Imaging, 2023.
4. Ning Z, Luo J, Xiao Q, et al. Multi-modal magnetic resonance imaging-based grading analysis for gliomas by integrating radiomics and deep features [J]. Ann Transl Med, 2021,9(4): 298.
5. Calabrese E, Rudie JD, Rauschecker AM, et al. Combining radiomics and deep convolutional neural network features from preoperative MRI for predicting clinically relevant genetic biomarkers in glioblastoma [J]. Neurooncol Adv, 2022,4(1): vdac060.
Figures