3779
A Subregion-based RadioFusionOmics Model Discriminates between Grade 4 Astrocytoma and Glioblastoma on Multisequence MRI1Department of Radiology, the Second Affiliated Hospital, Guangzhou, China, 2School of Biomedical Engineering, Southern Medical University, Guangzhou, China, 3Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics
Motivation: Investigated the underlying impact of subregional analysis on model performance: comparison of two volumes of interests (VOI) definition strategies.
Goal(s): To explore a subregion-based RadioFusionOmics (RFO) model for discrimination between adult-type grade 4 astrocytoma and glioblastoma.
Approach: Subregional radiomics analysis using the K-means clustering demonstrated discriminative performance comparable to that of manual segmentation. Edematous subregion is a possible intratumoral heterogeneity phenotype that differentiates grade 4 astrocytoma from glioblastoma.
Results: The RFO model that was trained using fused features achieved the AUC of 0.868 (VOI3) and 0.884 (H34) in the primary cohort (p=0.059), and 0.824 (VOI3) and 0.838 (H34) in the testing cohort (p=0.023).
Impact: Fusion of features from edematous subregions of multiple MRI sequences by the RFO model identified IDH genotypes of adult type grade 4 gliomas in line with current WHO CNS 5 criteria.
Introduction
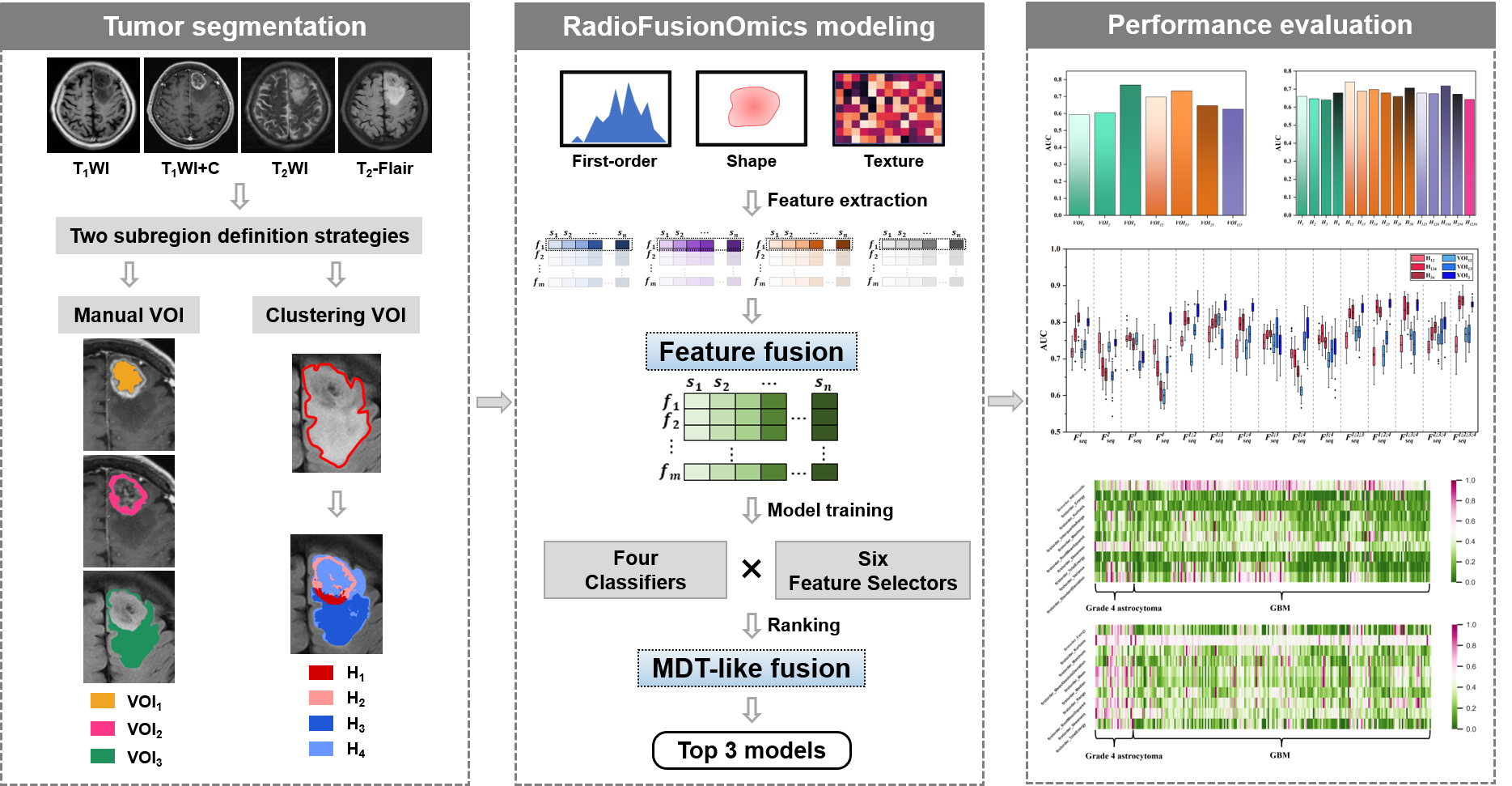
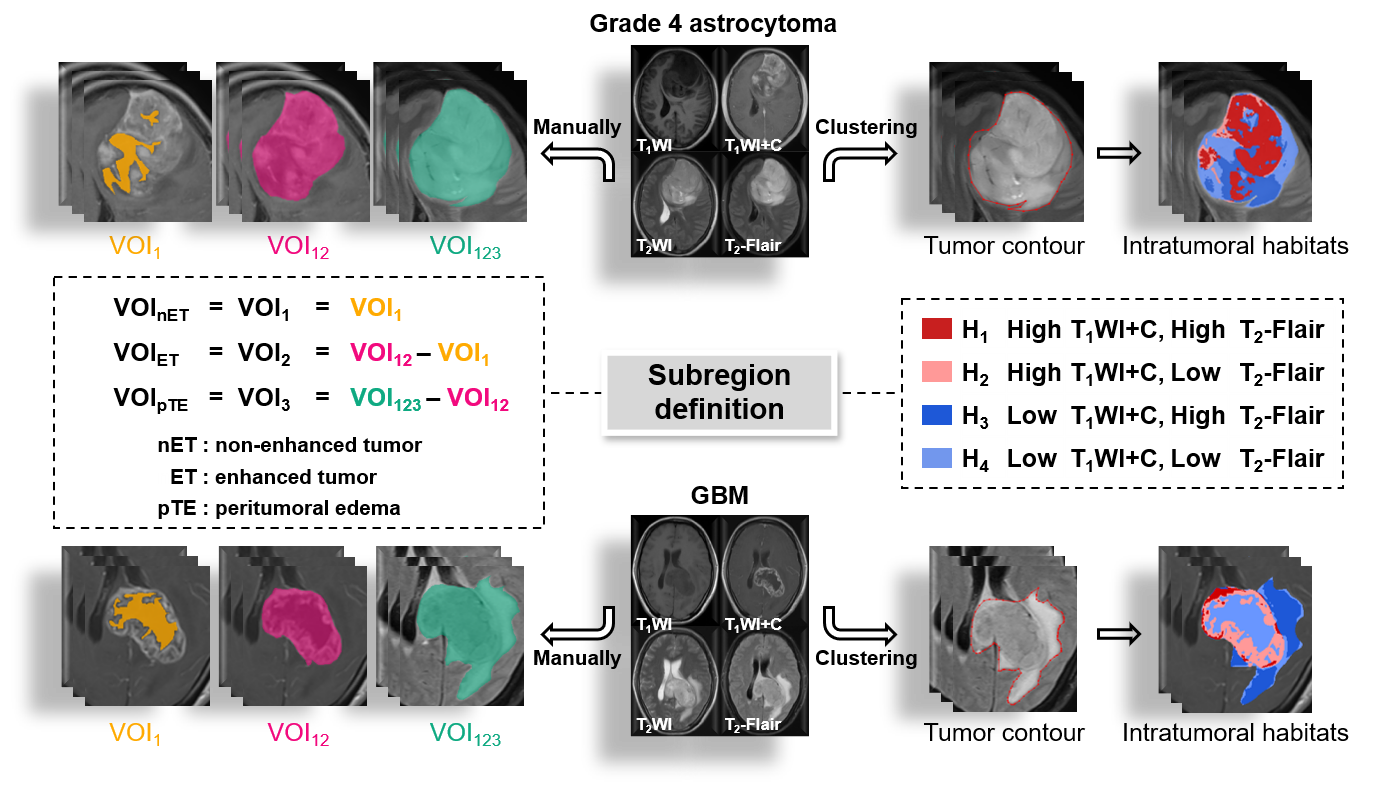
Glioblastoma (GBM) is the most aggressive and malignant adult brain tumor that has a poor prognosis1. Exploring a novel radiomics model for noninvasive discrimination between grade 4 astrocytoma and GBM provides an important reference for doctors to choose treatment options, which is of great significance to clinical practice. Besides, a lot of localized imaging information associated with tumor aggressiveness and treatment-resistance can be obtained via subregional radiomics analysis of the entire tumor, whose first step is manual or automatic segmentation of the tumor into several subregions, e.g., necrosis, enhancing core and peritumoral edema, as per MRI signal intensity by neuroradiologists or using deep learning segmentation methods2-5. Thus, the two specific goals of this study were: (i) to develop a subregion-based RFO model —which is designed for grade 4 gliomas — for the prediction of IDH genotype, and (ii) to determine the impact of the two subregion definition strategies — manual and clustering — on model performance.Methods
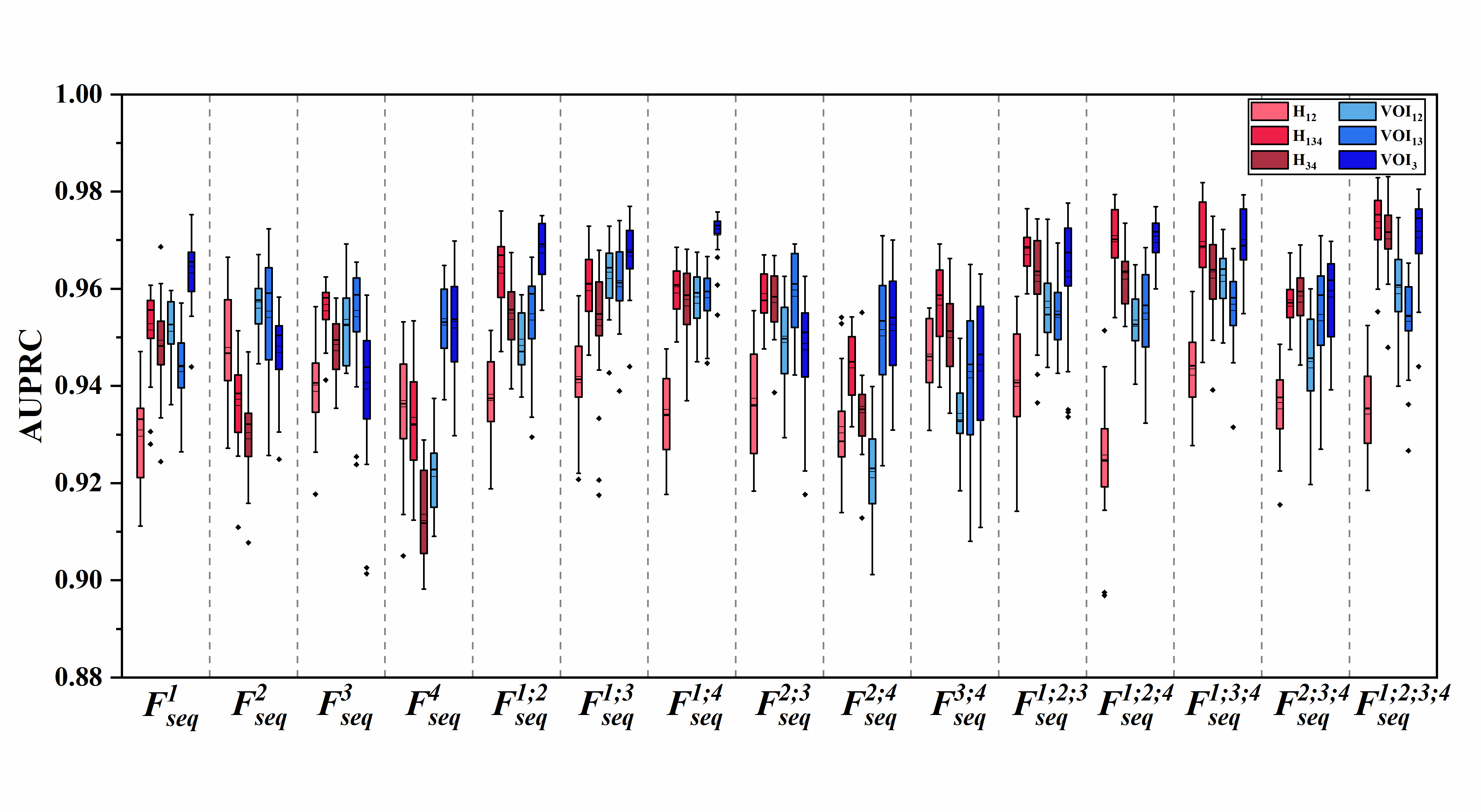
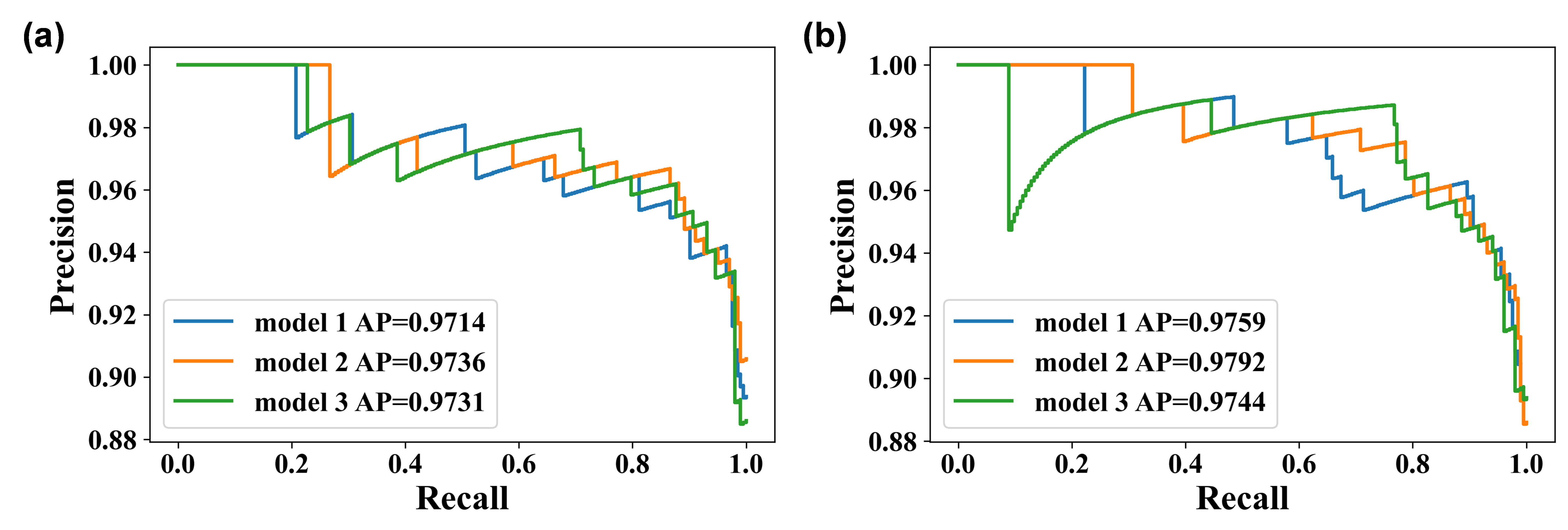
329 patients (40 grade 4 astrocytomas and 289 glioblastomas) with histologic diagnosis was retrospectively collected from our local institution and The Cancer Imaging Archive (TCIA). The volumes of interests (VOIs) were obtained from four multiparametric MRI sequences (T1WI, T1WI+C, T2WI, T2-FLAIR) using 1) manual segmentation of the non-enhanced tumor (nET), enhanced tumor (ET), and peritumoral edema (pTE), and 2) K-means clustering of four subregions (H1, H2, H3 and H4). The optimal VOI and best MRI sequence combination were determined. The performance of the RFO model was evaluated using the area under the precision-recall curve (AUPRC) and the best signatures were identified.Results
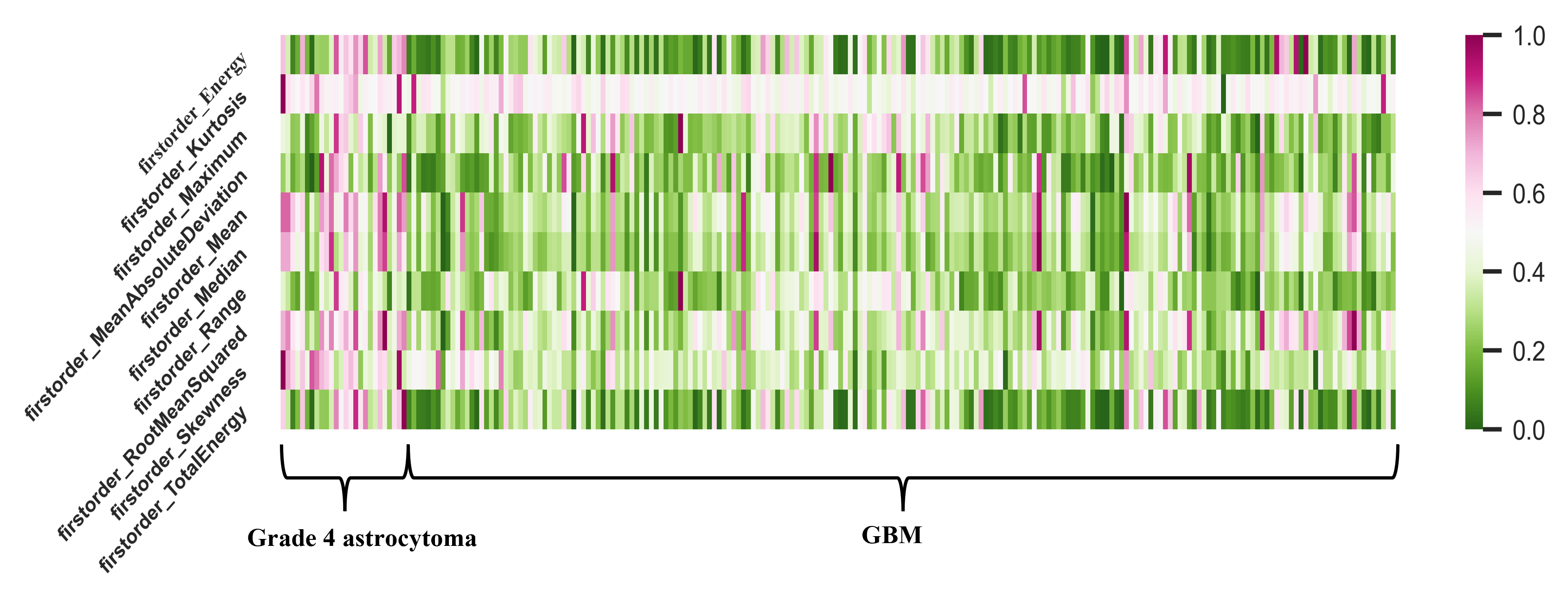
The two best VOIs were manual VOI3 (putative peritumoral edema) and clustering H34 (low T1WI+C, high T2-FLAIR (H3) combined with low T1WI+C and low T2- FLAIR (H4)). Features fused from four MRI sequences ( ) outperformed those from either a single sequence or other sequence combinations. The RFO model that was trained using fused features achieved the AUPRC of 0.972 (VOI3) and 0.976 (H34) in the primary cohort (p=0.905), and 0.971 (VOI3) and 0.974 (H34) in the testing cohort (p=0.402).Discussion
Subregion identification is a critical step in defining anatomically (or radiographically) meaningful localized zones for characterization of a glioma lesion6,7. In this study, we compared the two aforementioned subregion definition strategies and the best performance was seen in clustering subregion H34 with all four sequences T1WI, T2WI, T2-FLAIR and T1WI+C fused in the RFO model. This suggests that voxel-based clustering subregions might also define heterogeneity-related intratumoral territories when reliable radiomics signatures are extracted. The two optimal VOIs, manual VOI3 and clustering H34, were composed of tumor peripheral edematous regions. This indicates that the edema area contains informative spatial diversity signatures associated with either molecular alterations or aggressive tumor behavior, both of which contribute to differentiating grade 4 astrocytoma from GBM. This corroborates tumor heterogeneity phenotypes manifesting in surrounding edematous regions8,9. Furthermore, both tumor edema and subregions with low T1WI+C and high/low T2-FLAIR are crucial for distinguishing the underlying genetic changes between grade 4 astrocytoma and GBM.Conclusion
In conclusion, subregions defined by clustering achieved discriminative accuracy comparable to manual delineation. Fusion of features from edematous subregions of multiple MRI sequences by the RFO model identified IDH genotypes of adult type grade 4 gliomas in line with current WHO CNS 5 criteria.Acknowledgements
No acknowledgement found.References
1 Singh K, Batich KA, Wen PY et al (2021) Designing Clinical Trials for Combination Immunotherapy: A Frame-work for Glioblastoma. Clinical Cancer Research 28:585-593 2 Rudie JD, Rauschecker AM, Bryan RN, Davatzikos C, Mohan S (2019) Emerging Applications of Artificial Intelli-gence in Neuro-Oncology. Radiology 290:607-618 3 Liu D, Chen J, Ge H et al (2023) Radiogenomics to characterize the immune-related prognostic signature associat-ed with biological functions in glioblastoma. European Radiology 33:209-220 4 Li ZC, Bai H, Sun Q et al (2018) Multiregional radiomics profiling from multiparametric MRI: Identifying an im-aging predictor of IDH1 mutation status in glioblastoma. Cancer Med 7:5999-6009 5 Tan Y, Zhang ST, Wei JW et al (2019) A radiomics nomogram may improve the prediction of IDH genotype for astrocytoma before surgery. European Radiology 29:3325-3337 6 O'Connor JPB, Rose CJ, Waterton JC, Carano RAD, Parker GJM, Jackson A (2015) Imaging Intratumor Heteroge-neity: Role in Therapy Response, Resistance, and Clinical Outcome. Clinical Cancer Research 21:249-257 7 Cui Y, Tha KK, Terasaka S et al (2016) Prognostic Imaging Biomarkers in Glioblastoma: Development and Inde-pendent Validation on the Basis of Multiregion and Quantitative Analysis of MR Images. Radiology 278:546-553 8 Li Z, Bai H, Sun Q et al (2018) Multiregional radiomics profiling from multiparametric MRI: Identifying an imag-ing predictor of IDH1 mutation status in glioblastoma. Cancer Medicine 7:5999-6009 9 Dong F, Li Q, Jiang B et al (2020) Differentiation of supratentorial single brain metastasis and glioblastoma by using peri-enhancing oedema region–derived radiomic features and multiple classifiers. European Radiology 30:3015-3022Figures