3776
Predicting the IDH1 Mutation Status of Gliomas based on Multi-modality MRI Radiomics Combined with VASARI Features1Clinical medicine school of Ningxia Medical University, Yinchuan, China, 2Medical Imaging Center of Ningxia Hui Autonomous Region People's Hospital, Yinchuan, China, 3Department of Radiology ,the First Hospital Affiliated to Hainan Medical College, Haikou, China, 4GE Healthcare MR Research, Beijing, China, 5Department of Radiology, General Hospital of Ningxia Medical University, Yinchuan, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics, Gliomas
Motivation: The IDH1 mutant state is an independent risk factor of affecting the treatment and prognosis of glioma. Predicting the IDH1 status accurately pre-operator is crucial for making personalized treatment decisions for glioma patients.
Goal(s): This study aims to propose a non-invasive and convenient model based on MRI to predict the IDH1 status of gliomas before operation accurately.
Approach: Building three machine learning models based on multi-sequence MRI radiomics features, VASARI features, and combined features to predict the IDH1 status.
Results: These three models can predict the IDH1 status effectively and accurately, the combined model has the best diagnostic performance.
Impact: Models based on conventional MRI sequences and VASARI features provide the clinical value for evaluation of molecular typing in gliomas. It is expected to become a practical tool for the non-invasive characterization of gliomas to help the individualized treatment planning.
Introduction
Glioma, the most prevalent malignant primary brain tumor in adults, exhibits high heterogeneity and diverse molecular subtypes, necessitating distinct treatment strategies and yielding varying clinical prognoses1. Isocitrate dehydrogenase 1 (IDH1) status has been associated with improved prognosis and treatment response in gliomas2. Consequently, determining IDH1 status is critical for predicting survival rates and guiding treatment decisions. Significant efforts have been devoted to developing non-invasive image-based diagnostic methods for IDH1 status assessment. Radiomics, a high-throughput approach for extracting quantitative features from medical images, enables the quantitative representation of tumor heterogeneity3. The Visually Accessible Rembrandt Images (VASARI) feature set, specifically designed for gliomas, provides a quantitative or semi-quantitative description of imaging features based on conventional MRI images4. This study aims to employ machine learning models based on pre-operative MR image radiomics features and VASARI features to predict the IDH1 mutation status of gliomas.Methods
This retrospective study included 452 patients (193 female, 48.7±1.1 years; 259 male, 50.0±1.2 years) who met the following inclusion criteria: (i) pathologically confirmed glioma, (ii) known IDH1 status, (iii) preoperative MRI inclusive of CE-T1WI, T2WI, T1WI, T2flair, and (iv) age ≥ 18 years. All MR examinations were performed on a 3.0T MR scanner (SIGNATM Architect; GE Healthcare, Milwaukee, WI, USA) with a 48-channel head coil. The scan protocol and detailed parameters were listed in Table 1. The patients were randomly divided into training and validation sets at a ratio of 3:2. The study comprised three models. Firstly, 22 VASARI features were extracted and analyzed by two physicians. Univariate and multivariate logistic regression (LR) were performed to select independent predictors for IDH status to construct the VASARI model. Secondly, radiomic features were extracted from the VOI of CE-T1WI, T2WI, and T2flair, and the optimal radiomic features were selected to calculate the Radiomics score. The Classifier eXtreme Gradient Boosting (XGBoost) was used to contrast the radiomics model. Finally, filtered VASARI features and Rad-score were included in multivariate LR to contrast the combined model. The efficacy of the models was evaluated and compared using receiver operating characteristic (ROC) curves and DeLong test, while decision curve analysis (DCA) and calibration curves were plotted to evaluate their clinical value and calibration degree.Results
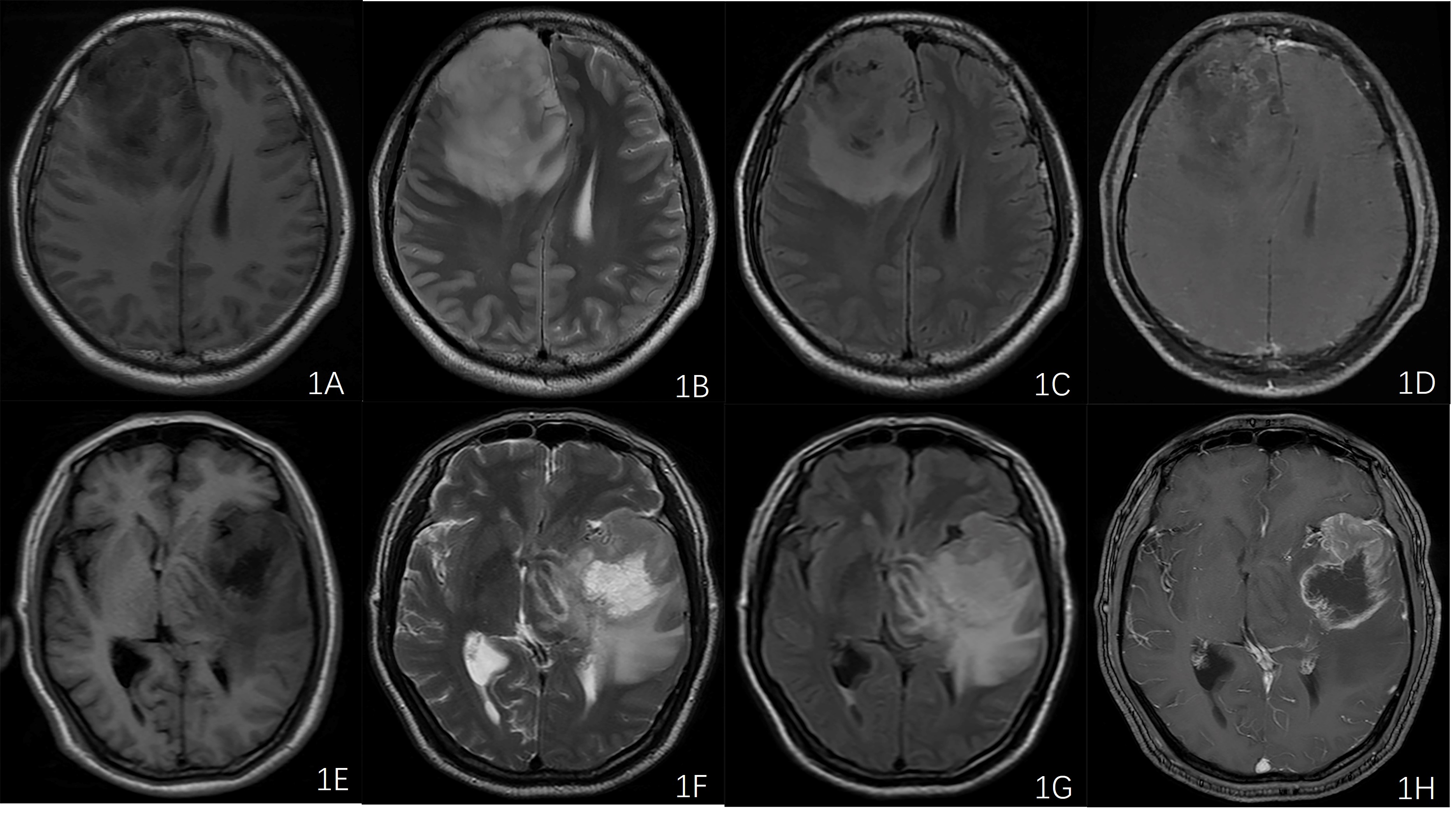
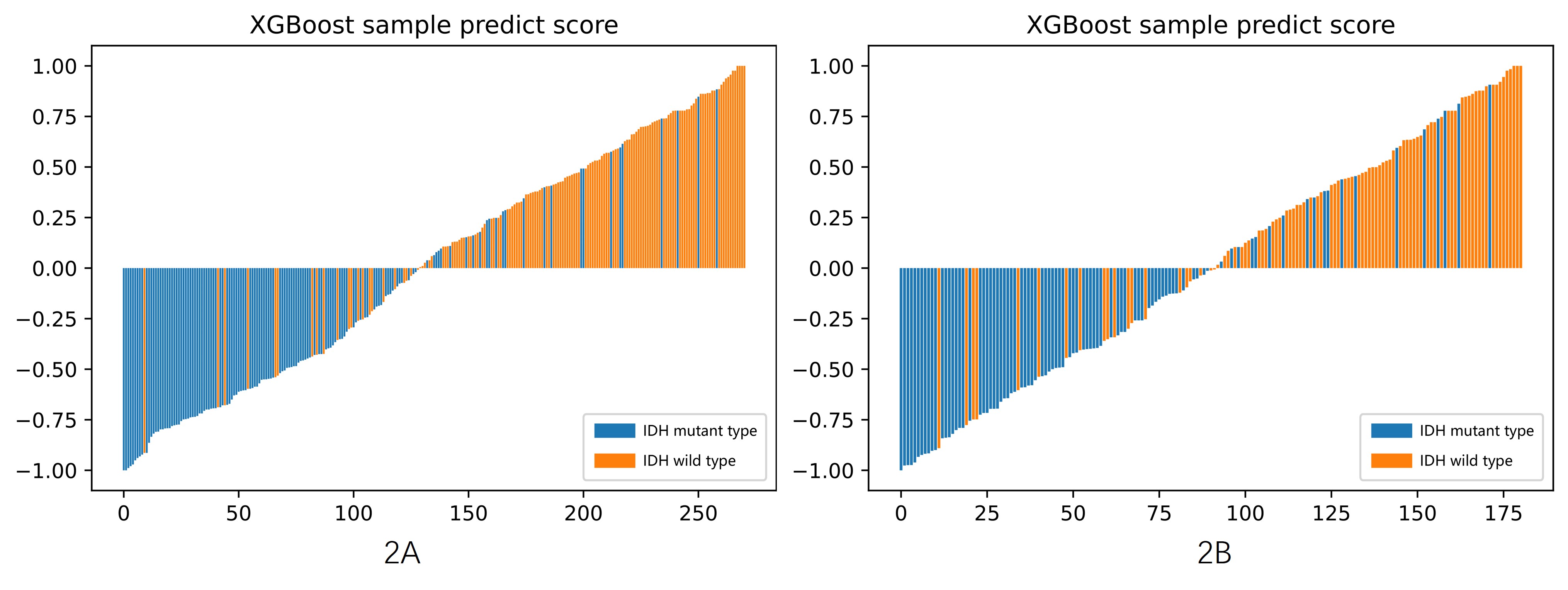
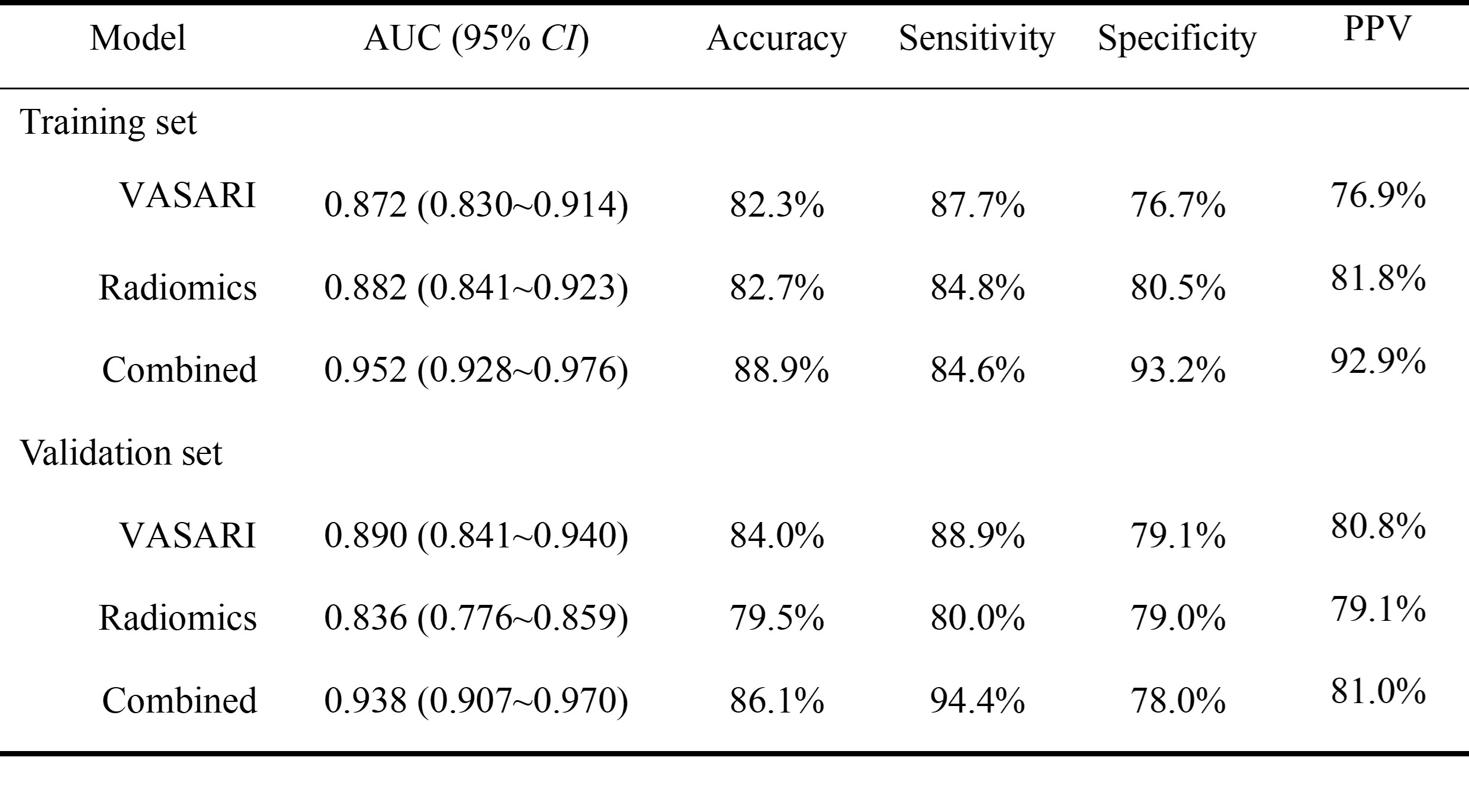
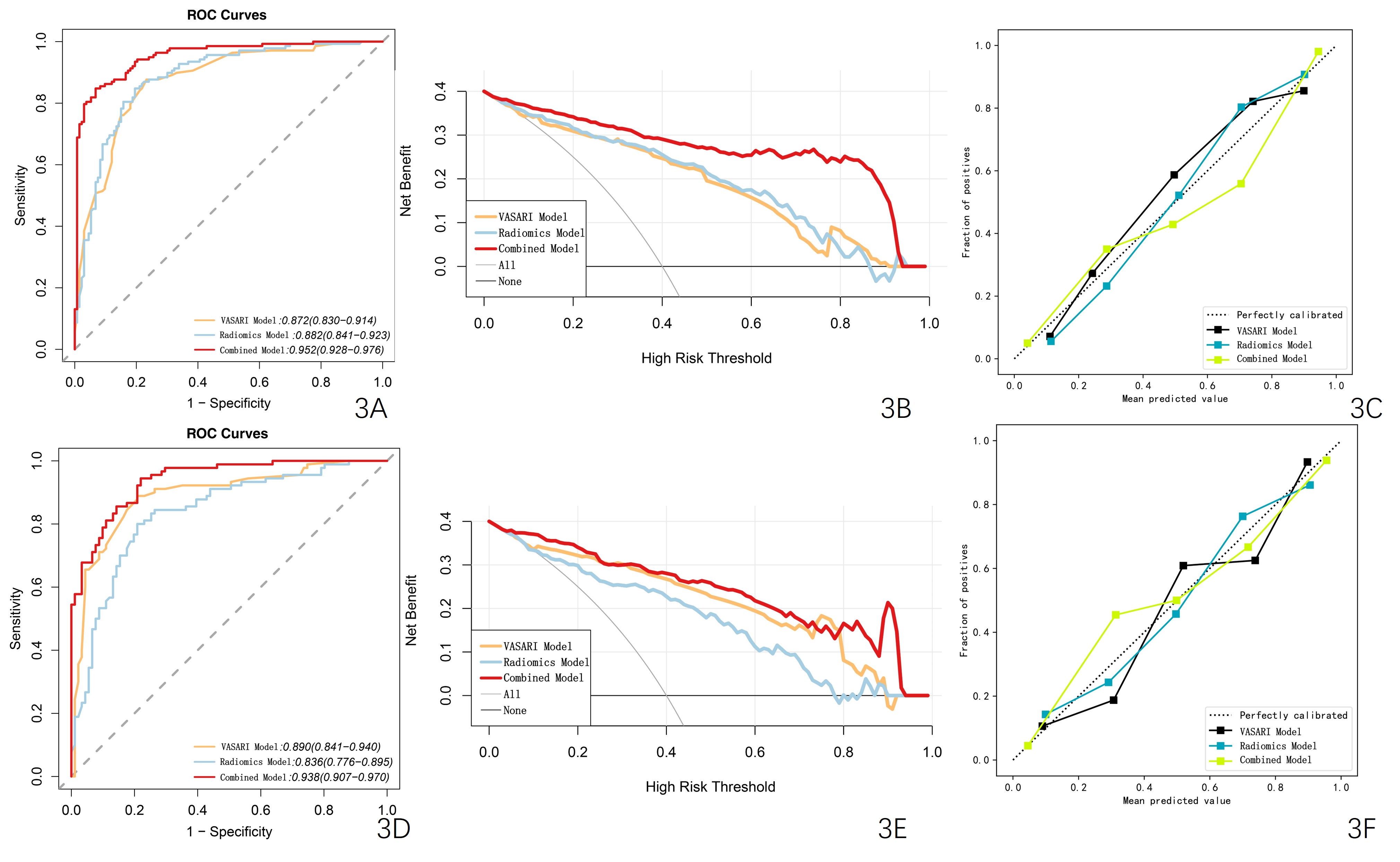
The F1, F4, F7, and F11 in the VASARI feature set were significant predictors of the IDH mutation status (Figure 1). Totally 11 optimal radiomics features were screened to calculate Rad-score and build radiomics model (Figure 2). The AUC of combined model were higher than VASARI model and radiomics model both in training set and validation set (training set: 0.952 vs. 0.872,0.882; validation set: 0.938 vs. 0.890, 0.836) (Figure 3,Table 2). The difference was statistically significant (Delong test, P<0.05). DCA showed the combined model had the largest net benefit and the best clinical practicality. The calibration curves showed that all the 3 models were well calibrated, while the combined model had the best calibration (Figure 3).Discussion
glioblastoma. Patients with the IDH-mutant subtype generally have a longer median survival time compared to those with the wild-type subtype[5]. Our study successfully developed a model that combines conventional MRI radiomics and VASARI features to predict the IDH mutation status in gliomas. This model demonstrated good stability and repeatability in quantitatively predicting the molecular subtypes of gliomas. By integrating macro (VASARI) and micro (Radiomics) features, the accuracy of the model was improved. However, it is important to note that machine learning models require a large amount of data to ensure stability and prevent overfitting. One limitation of our study is the lack of an external validation set. Therefore, future studies with larger cohorts of subjects are needed to validate and further improve the model.Conclusion
In conclusion, our study shows that the IDH1 status of gliomas can be predicted using radiomics and VASARI models based on conventional MR imaging.Acknowledgements
No acknowledgement found.References
[1] Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary[J]. Neuro Oncol,2021,23(8):1231-1251. [2] Kayabolen A, Yilmaz E, Bagci-Onder T. IDH Mutations in Glioma: Double-Edged Sword in Clinical Applications? [J]. Biomedicines,2021,9(7):799. [3] Li Y, Wei D, Liu X, et al. Molecular subtyping of diffuse gliomas using magnetic resonance imaging: comparison and correlation between radiomics and deep learning [J]. Eur Radiol,2022,32(2):747-758. [4] Gevaert O, Mitchell LA, Achrol AS, et al. Glioblastoma multiforme: exploratory radiogenomic analysis by using quantitative image features[J]. Radiology,2014,273(1):168-174. [5] Hempel JM, Bisdas S, Schittenhelm J, et al. In vivo molecular profiling of human glioma using diffusion kurtosis imaging [J]. J Neurooncol,2017,131(1):93-101.Figures
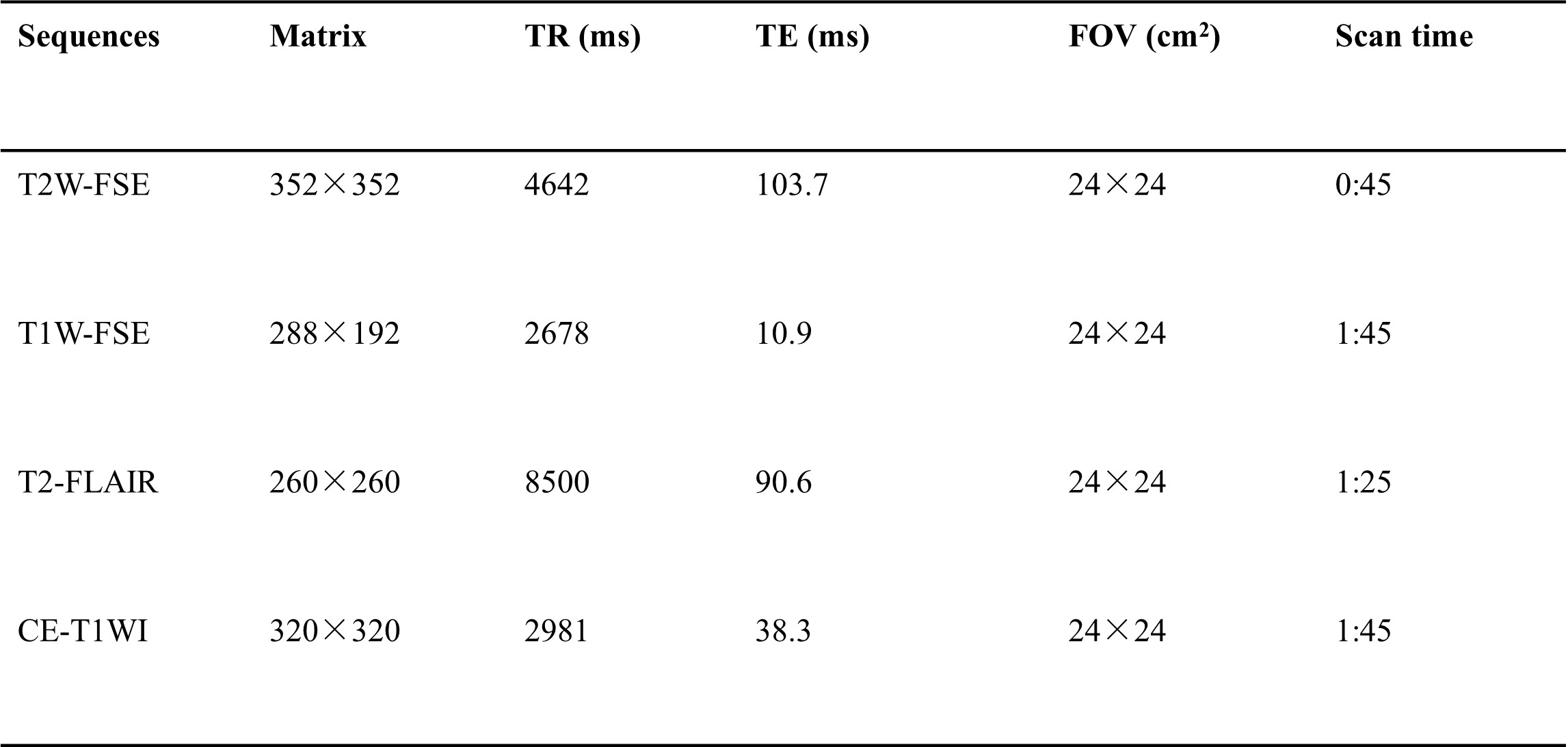
Table 1. The scan protocols and the main scan parameters used in this study.
Abbreviation: T2W-FSE: T2-weighted fast spin echo; T1W-FSE: T1-weighted fast spin echo; T2-FLAIR: T2-weighted fluid attenuation inversion recovery; CE-T1WI: contrast-enhanced T1-weighted **slice thickness/gap = 5/1mm; all images were collected in transverse view.