3775
Mathematical Modelling of Survival in Low Grade Gliomas at Malignant Transformation with XGBoost.1UCL, London, United Kingdom
Synopsis
Keywords: Diagnosis/Prediction, Cancer, glioma
Motivation: Early detection of low-grade glioma (LGG) malignant transformation (MT) is vital for treatment decisions, prognosis, quality of life and patient-centered care.
Goal(s): To develop non-linear machine learning models using XGBoost algorithm to predict overall survival using clinical, molecular, genetic and radiomic data at MT.
Approach: 553 LGGs with histology and MRI underwent in-house tumour segmentation pipeline with radiomic feature extraction and masked disconnectome of map components.
Results: XGB Classifier model predicted OS > 5 years from MT with an accuracy of 64%. Age, IDH1 mutation, 1p/19q co-deletion, regularity of tumour shape, and disconnectome-related perilesional components were most predictive of survival.
Impact: Understanding malignant transformation of low-grade gliomas is crucial for research and the development of new treatment strategies. Defining the radiological features at malignant transformation allows for a timely shift in the treatment plan with potential to improve repsonse to therapy.
Background
Low grade gliomas (LGG) represent 13-16% of gliomas and may remain stable years after initial diagnosis1. Prognosis after MT is markedly poor 2. Defining the radiological features at MT through radiomics could enable superior prognostication and support clinical decision-making in this patient group.Aim
The aim of this study was to develop non-linear machine learning models using the XGBoost algorithm to predict a continuous (overall survival (OS) and a binary survival outcome (OS > 5 years) using clinical, molecular and genetic, and radiomic data.Method
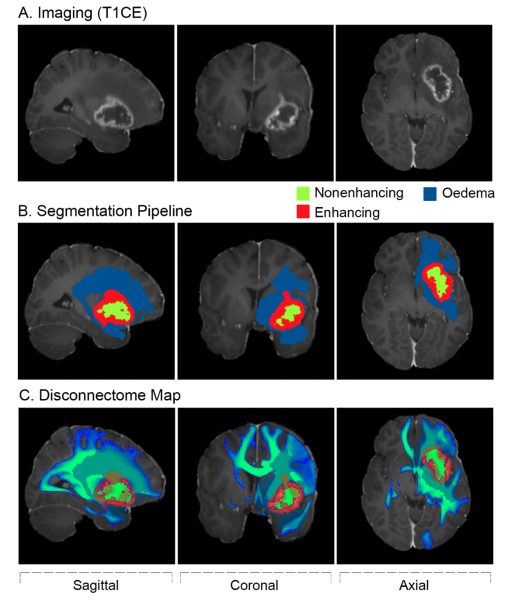
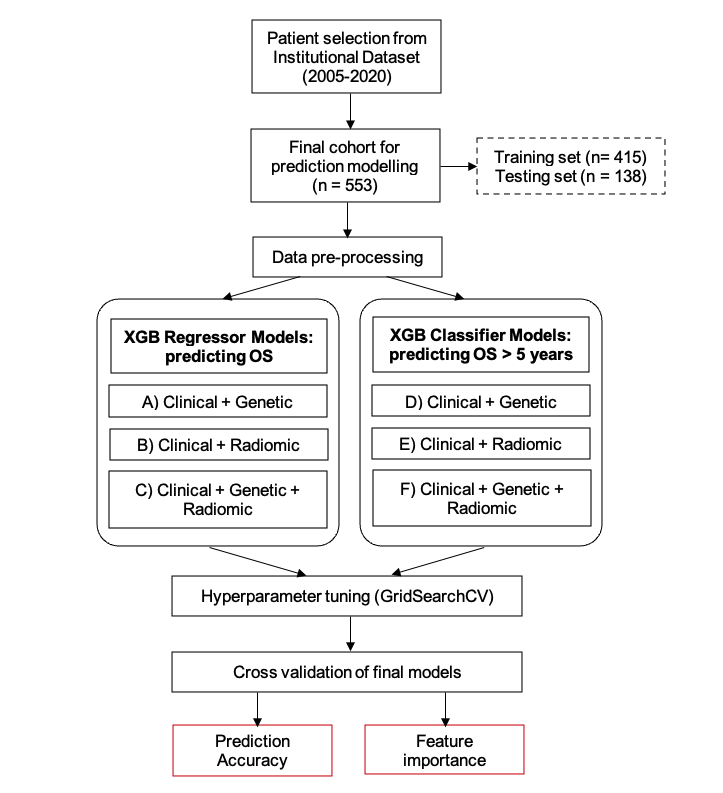
Patients with LGGs treated at a single institution (2005-2020) with histology and MRIs at the time of malignant transformation (MT) were retrospectively included in this study. MRIs underwent in-house tumour segmentation pipeline with radiomic feature extraction of whole tumour, enhancing, non-enhancing and oedema components 3, and masked disconnectome map components (Figure 1). Patients were split into training and testing sets for the development of the survival models which were assessed with mean absolute error (MAE) and root mean square error (RMSE) for the prediction of OS; and receiver operating characteristics analysis for the prediction of OS > 5 years.Results
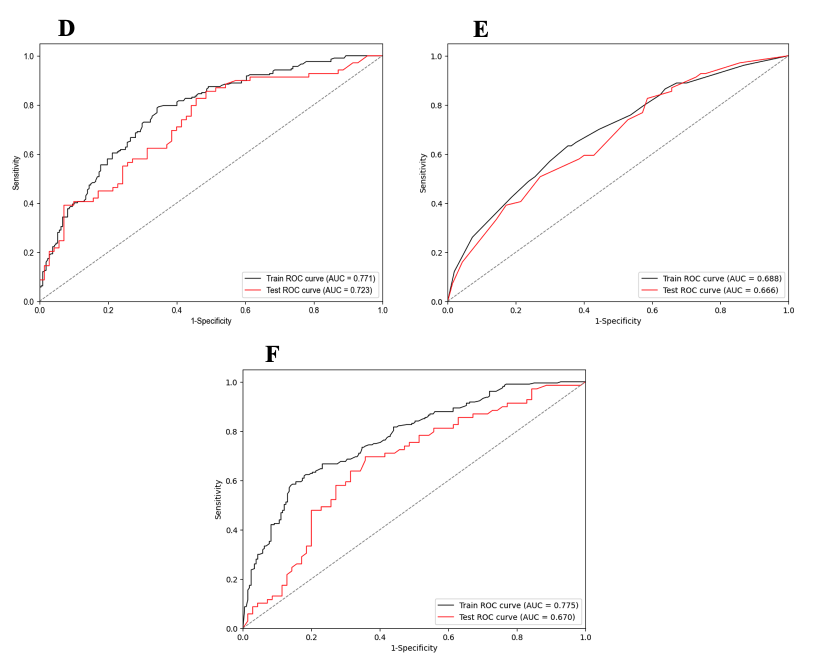
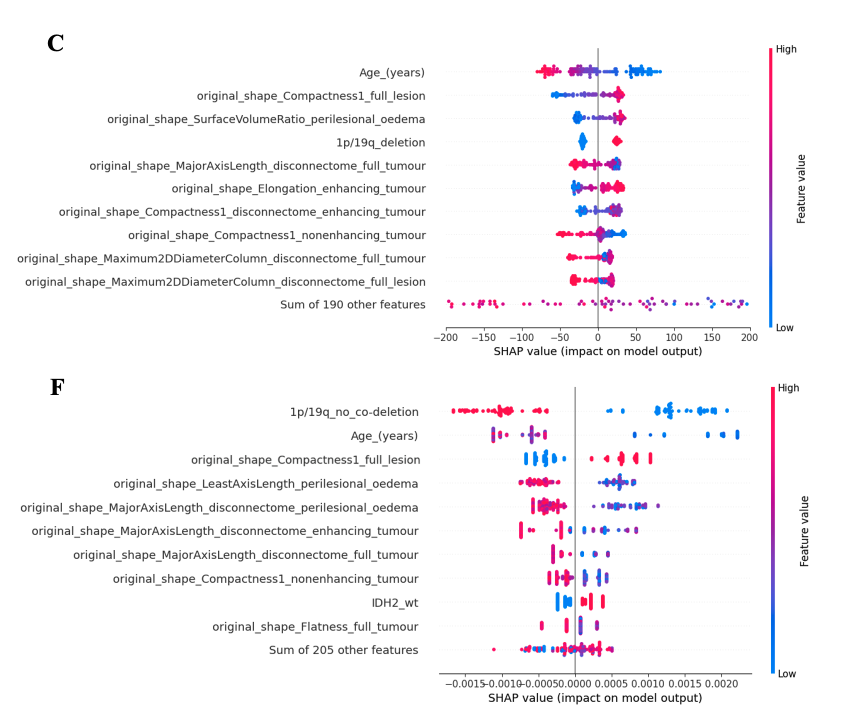
Of the total 553 patients, 415 patients were included in the training set and 138 patients in the testing set (Figure 2). The XGB Regressor model4 was able to predict overall survival (OS) from the time of malignant transformation (tMRI) with an MAE of 953 days (RMSE: 1163 days). The XGB Classifier model was able to predict the probability of OS > 5 years from tMRI with an accuracy of 64% (sensitivity: 58%, specificity: 70%). See Figure 3 for ROC-AUC curves of the three XGB Classifier models. Age, IDH1 mutation, 1p/19q co-deletion, regularity of tumour shape, and disconnectome-related perilesional components were most predictive of survival outcome (Figure 4).Conclusion
This study has investigated the predictive capabilities of clinical, molecular and genetic, and radiomic data to develop survival analysis models, using the XGBoost algorithm, to predict OS and OS beyond 5 years in patients with LGG at tMRI. This study corroborates previous findings that age, 1p/19q co-deletion and IDH1 mutation are positive prognosticators for survival. However, further investigation into the radiomics of the disconnectome, especially of the perilesional oedema compartment, would potentiate an intriguing and novel avenue for survival analysis of patients with LGG.Acknowledgements
This work has been supported by the NIHR UCLH/UCL Biomedical Research Centre.References
1. Rasmussen, Birthe Krogh, Steinbjørn Hansen, René J. Laursen, Michael Kosteljanetz, Henrik Schultz, Bente Mertz Nørgård, Rikke Guldberg, and Kim Oren Gradel. 2017. “Epidemiology of Glioma: Clinical Characteristics, Symptoms, and Predictors of Glioma Patients Grade I–IV in the the Danish Neuro-Oncology Registry.” Journal of Neuro-Oncology 135 (3): 571–79. https://doi.org/10.1007/s11060-017-2607-5.
2. Rees, Jeremy, Hilary Watt, H. Rolf Jäger, Chris Benton, Daniel Tozer, Paul Tofts, and Adam Waldman. 2009. “Volumes and Growth Rates of Untreated Adult Low-Grade Gliomas Indicate Risk of Early Malignant Transformation.” European Journal of Radiology 72 (1): 54–64. https://doi.org/10.1016/j.ejrad.2008.06.013.
3. Ruffle, J.K., Samia Mohinta, Gray, R., Harpreet Hyare and Parashkev Nachev (2023). Brain tumour segmentation with incomplete imaging data. Brain communications, [online] 5(2). doi:https://doi.org/10.1093/braincomms/fcad118.
4. Barnwal, A., Cho, H. and Hocking, T.D. (2020). Survival regression with accelerated failure time model in XGBoost. [online] arXiv.org. Available at: https://arxiv.org/abs/2006.04920
Figures