3774
Machine learning based MRI radiomics model in predicting postoperative progressive cerebral edema and hemorrhage after resection of meningioma1Advanced Neuroimaging Laboratory, The Affiliated Yuebei People's Hospital of Shantou University Medical College, Shaoguan, Guangdong Province, China, 2Department of Radiology, The Affiliated Yuebei People's Hospital of Shantou University Medical College, Shaoguan, Guangdong Province, China, 3GE Healthcare, MR Research China, Beijing, China, 4Department of Neurosurgery, The Affiliated Yuebei People's Hospital of Shantou University Medical College, Shaoguan, Guangdong Province, China
Synopsis
Keywords: Diagnosis/Prediction, Brain, Radiomics; Meningioma; Machine Learning; Hemorrhage; Cerebral Edema
Motivation: Prediction radiomics analysis of postoperative progressive cerebral edema and hemorrhage which are the most common complications after meningioma resection, is limited.
Goal(s): To develop and validate a machine learning model to predict progressive cerebral edema and hemorrhage after meningioma resection.
Approach: Reviewing the preoperative MRI of 148 pathology-confirmed meningiomas, extracting radiomics features of tumor enhancement and peritumoral edema regions, and combining clinical characteristics to build machine learning multiparametric MRI radiomics predictive models.
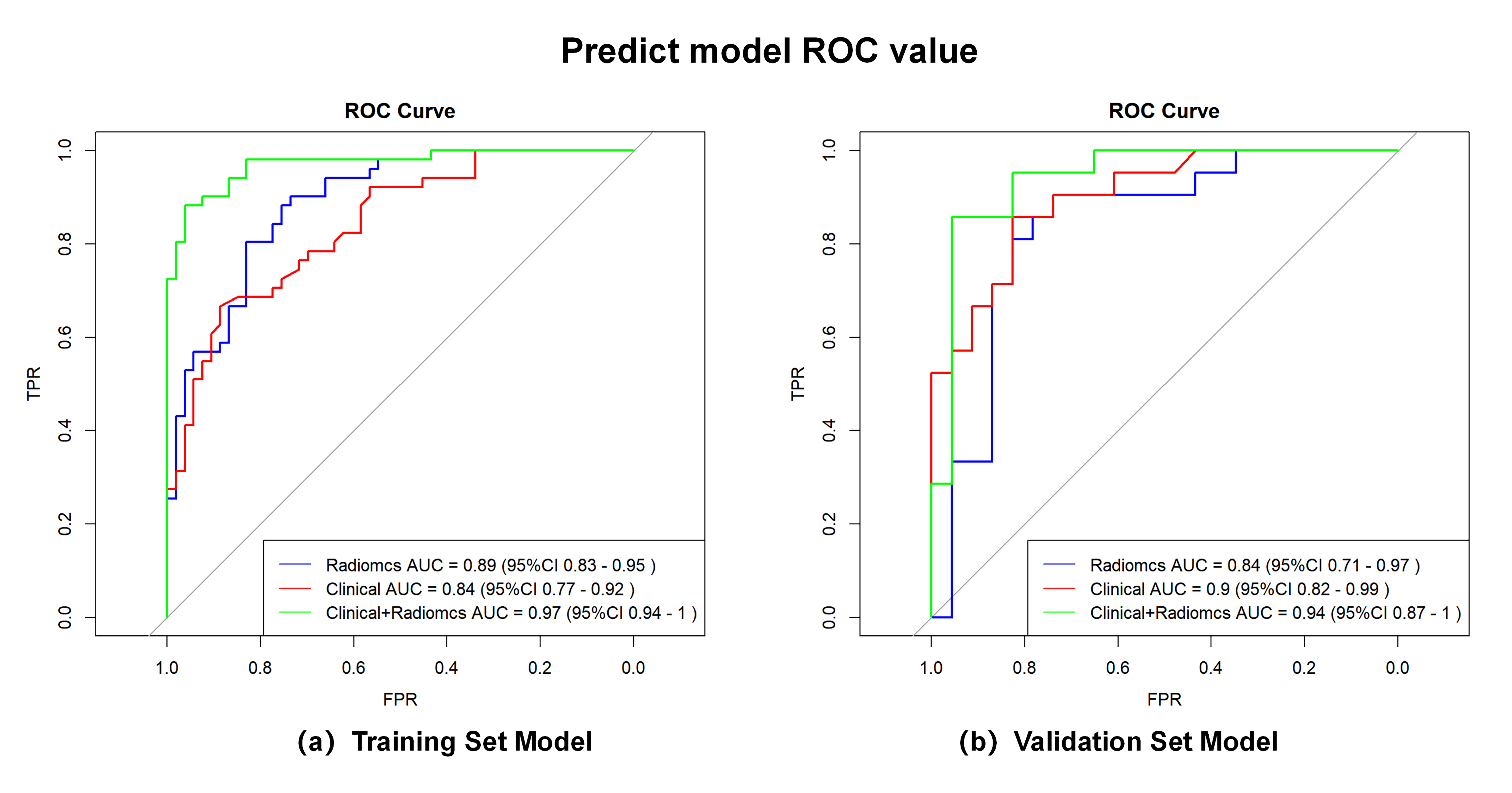
Results: The combining model including both enhancement and edema radiomics features, and clinical characteristics including systolic blood pressure, showed the best predictive performance with AUC of 0.94 for the validation set.
Impact: We proposed a novel model that included clinical indicators and multi-parameter radiomics features, which can accurately and non-invasively predict progressive cerebral edema and hemorrhage after meningioma resection, enabling improving clinical management and quality of life of patients with meningioma.
INTRODUCTION
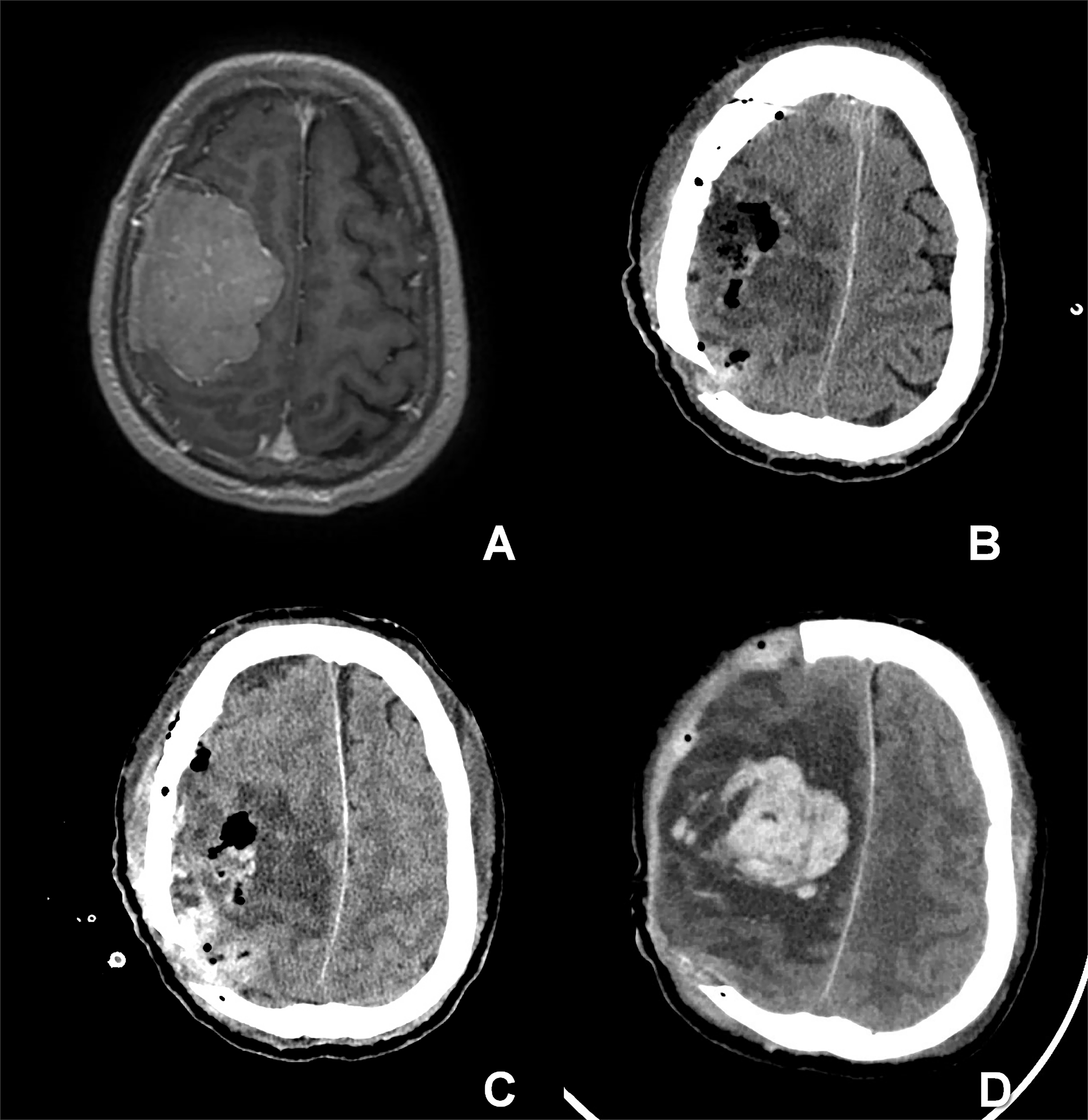
Meningioma is the most common intracranial tumor in the world 1, and total resection is the standard treatment approach. Progressive cerebral edema and hemorrhage are major complications after resection of intracranial meningioma 2, 3. However, their incidence and risk factors are still unclear. Most of the published radiomics studies in meningioma have focused on tumor grading using the MRI-based features of mass enhancement. In this study, we developed and validated a multiparametric MRI machine learning model based on features of both mass enhancement and peritumoral edema regions, and offered a nomogram for easy assessment in clinics.METHODS
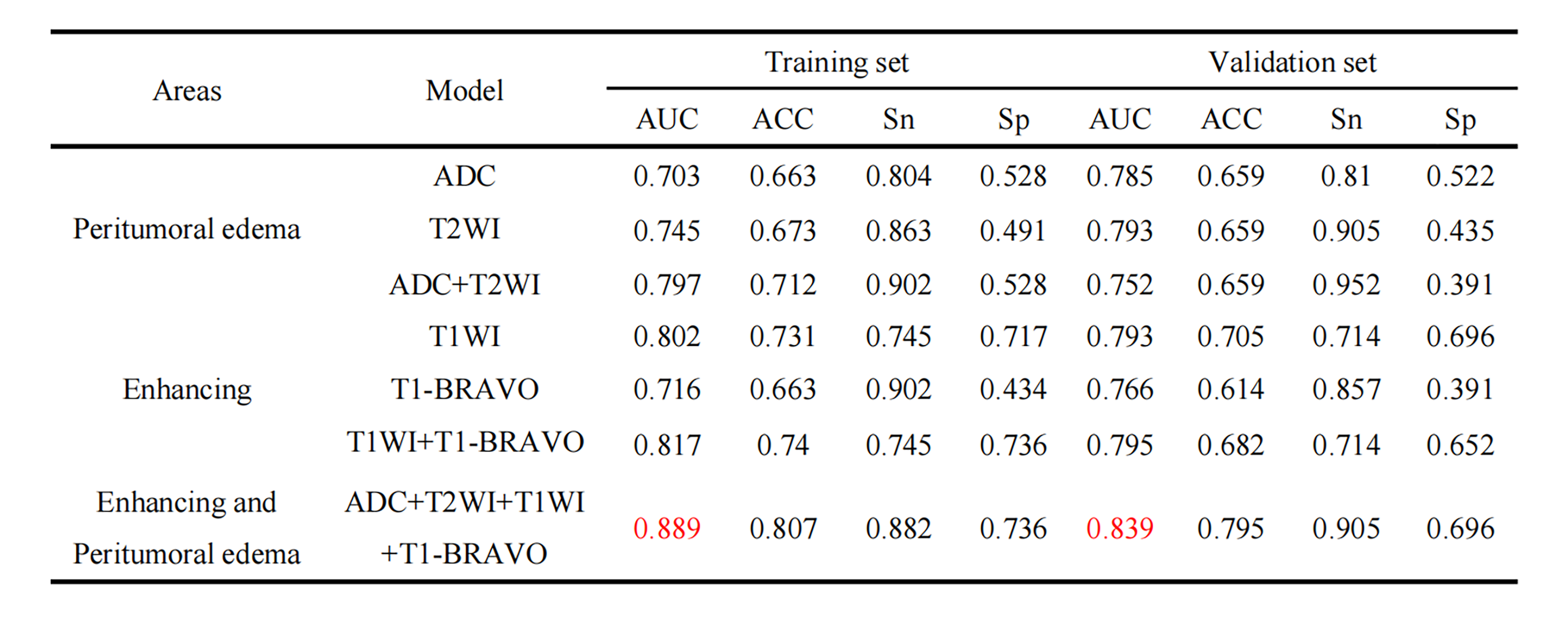
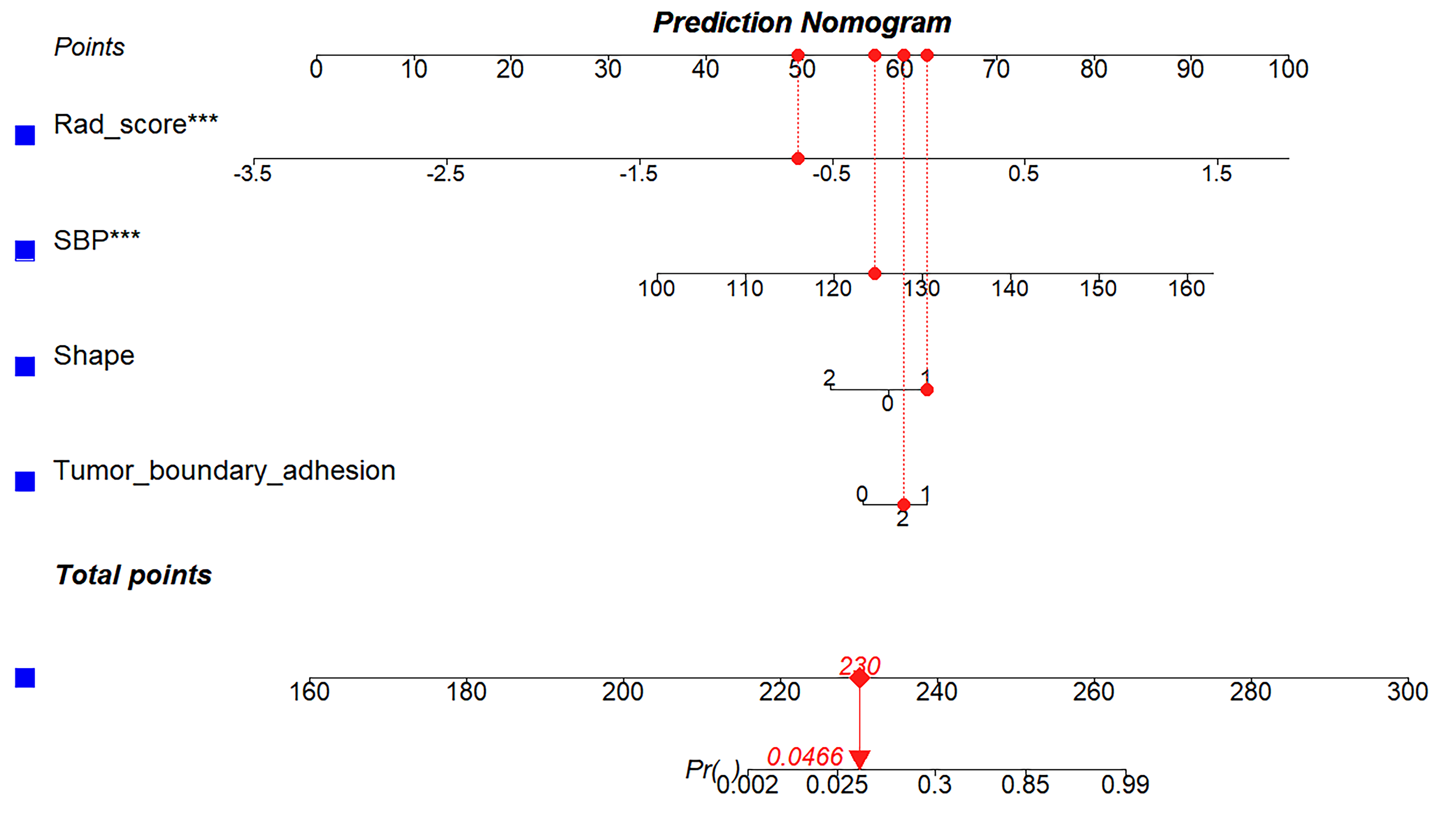
This study retrospectively collected 148 patients with pathology-diagnosed meningiomas and randomly divided them into the training and validation set at a ratio of 7:3. Radiomics features were extracted from enhancing part based on pre-contrast T1WI and post-contrast T1-BRAVO images and peritumoral edema areas based on ADC maps and T2WI images. Mann-Whitney U test and the least absolute shrinkage and selection operator (LASSO) were used to select the most representative features and compute the Rad-Score. Different radiomics models (T1WI only, T1-BRAVO only, ADC only, T2WI only, T1WI+T1-BRAVO, ADC+T2WI, and T1WI+T1-BRAVO+ADC+T2WI) were constructed by the support vector machine (SVM). Logistics regression (LR) was used to explore the clinical risk factors that influenced progressive cerebral edema and hemorrhage after resection of intracranial meningioma. The prediction models using both clinical information and radiomics features were built, and all diagnostic performance was assessed using the area under the curve (AUC) and visualized in the nomogram.RESULTS
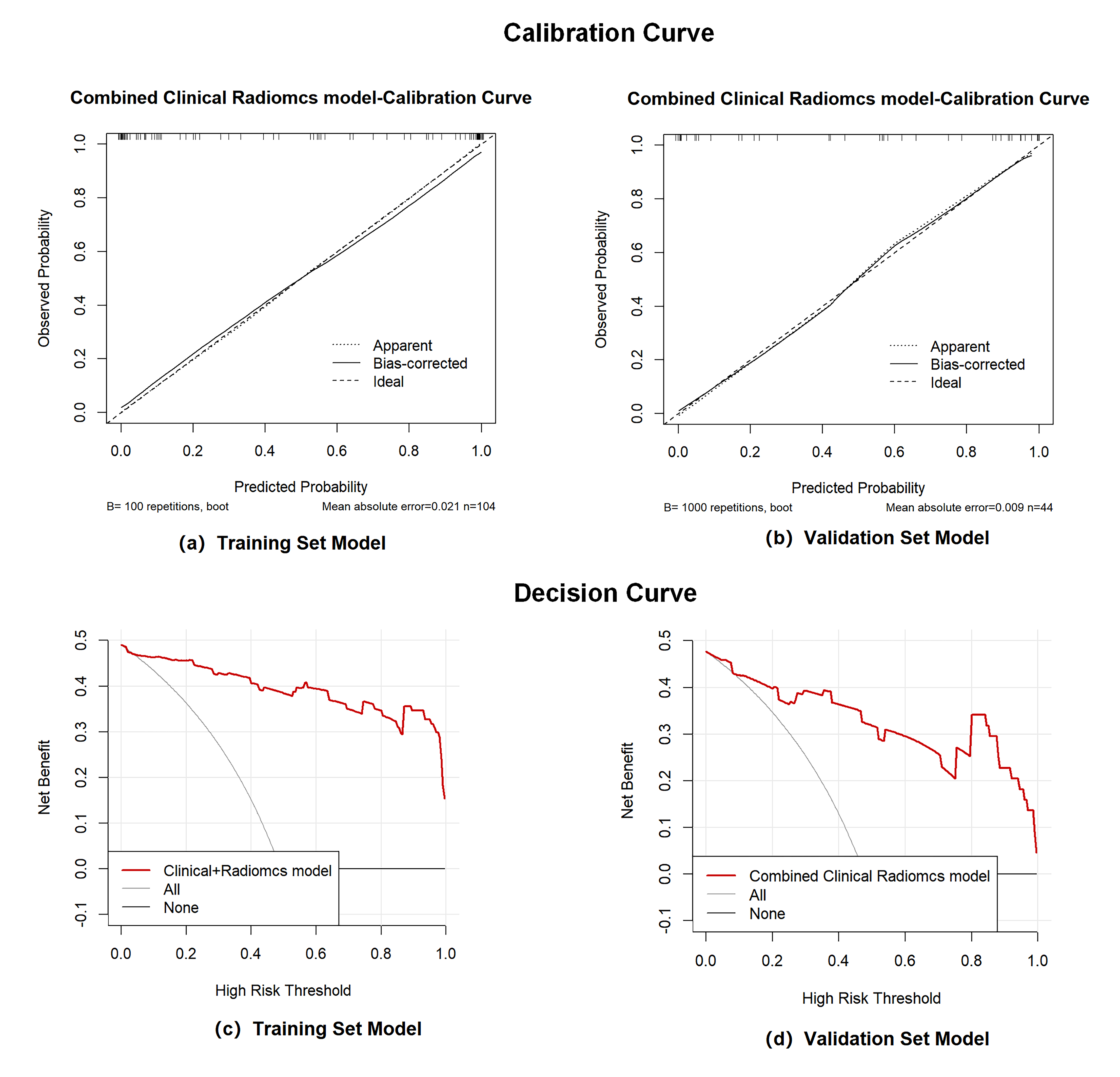
There are 72 cases (48.64%) of patients who suffered progressive cerebral edema and hemorrhage after resection of meningioma. Preoperative systolic blood pressure, tumor shape, and tumor boundary adhesion are clinically independent risk factors for progressive cerebral edema and hemorrhage after resection of meningioma. The traditional radiomics model with only enhanced tumor region (training set AUC: 0.817(95% CI: 0.74-0.90), validation set AUC: 0.795(95% CI: 0.66-0.93)) showed significantly lower predictive performance than the multiparametric MRI features model with peritumoral cerebral edema region (training set AUC: 0.889(95% CI: 0.83-0.95), validation set AUC: 0.839(95% CI: 0.71-0.97)). Furthermore, the predictive model combining clinical characteristics and radiomics features has the best performance, with AUC values of 0.97 (95% CI: 0.94-1.00) and 0.94 (95% CI: 0.87-1.00) for the training set and validation set.DISCUSSION
48.64% of patients in our study suffered progressive cerebral edema and hemorrhage following tumor resection, this finding shows a high prevalence of these complications and indicates the importance of the development of a predictive model in this field. Our findings demonstrated that the radiomics model using features of both the enhancement and peritumoral edema regions presents better prognostic performance than solely enhancing mass. These results suggest the extraction of imaging features of tumor enhancement only is limited in the prediction of postoperative progressive cerebral edema and hemorrhage. The severity of peri-enhancing tumor edema plays an important role in postoperative progressive cerebral edema and hemorrhage as an independent risk factor. Compared to the common radiomics tools of T1WI and T2WI in the evaluation of peritumoral edema characteristics, ADC map can provide more functional information. In addition, our findings showed preoperative systolic blood pressure was the best clinical characteristic in the combined predictive model. Further studies with larger cohorts will be necessary in the future for the mechanism exploration of radiomics features and systolic blood pressure in the development of postoperative progressive cerebral edema and hemorrhage after resection of meningioma. A nomogram to visualize our proposed prediction model may accelerate validation in more hospitals.CONCLUSION
We developed a novel model based on multi-parametric MRI radiomics derived from both enhancing mass and peritumoral edema regions, combining clinical characteristics, which can accurately and non-invasively predict progressive cerebral edema and hemorrhage after meningioma resection. This preliminary model can improve clinical management and quality of life of patients with meningioma in the future. In addition, our finding suggests the severity of the peritumoral edema plays an important role in the development of postoperative progressive cerebral edema and hemorrhage after the resection of meningioma, which may be useful for better understanding the potential mechanism of these complications.Acknowledgements
No acknowledgement found.References
1. Xiao D, Yan C, Li D, et al. National Brain Tumour Registry of China (NBTRC) statistical report of primary brain tumours diagnosed in China in years 2019-2020. Lancet Regional Health-Western Pacific, 2023, 34.
2. Gawlitza M, Fiedler E, Schob S, et al. Peritumoral Brain Edema in Meningiomas Depends on Aquaporin-4 Expression and Not on Tumor Grade, Tumor Volume, Cell Count, or Ki-67 Labeling Index. Molecular Imaging and Biology, 2017, 19(2): 298-304.
3. Gerlach R, Raabe A, Scharrer I, et al. Post-operative hematoma after surgery for intracranial meningiomas: Causes, avoidable risk factors and clinical outcome. Neurological Research, 2004, 26(1): 61-6.
Figures