3772
Machine Learning for Preoperative Prediction of EGFR Mutation in Lung Cancer Brain Metastasis1Department of Medical Imaging, Chi Mei Medical Center, Tainan, Taiwan, 2Department of Electrical Engineering, National Cheng Kung University, Tainan, Taiwan
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence, brain metastasis
Motivation: Lung cancer is the most common primary tumor showing brain metastasis (BM). Epidermal growth factor receptor (EGFR) mutations are detected in a significant proportion of lung cancer patients.
Goal(s): However, a subset of patients may show discordance in EGFR mutation status between the primary lung tumor and the corresponding BMs, which may affect decision-making in treatments.
Approach: We used machine learning (ML) based on pretreatment brain MRI and clinical data for prediction of EGFR mutation status in BMs of lung cancer.
Results: Among various ML algorithms, the best predictive performance with accuracy of 89%, precision of 88%, and AUC of 0.97 were obtained.
Impact: Machine learning based on pretreatment clinical data and brain MRI provides the potential to predict the EGFR mutation status in brain metastasis of lung cancer, and may affect decision-making in treatments.
Background and Purpose
Lung cancer is one of the leading causes of cancer-related death in the world, and 10-36% of all lung cancers developing brain metastasis (BM) during the course of the disease 1. Epidermal growth factor receptor (EGFR) mutations are detected in 10-60% of all non-small cell lung cancer (NSCLC) patients and are associated with poor survival 2, 3. It is known EGFR tyrosine kinase inhibitor improves survival in NSCLC patients with EGFR mutations 4. Therefore, the determination of EGFR mutation status is critical for prognosis and therapeutic decision-making. Recently, discordance in EGFR status between primary lung cancers and BMs has often been reported 5, indicating that it is not completely correct to determine the EGFR status of BMs based on the status of the primary lung tumor. Thus, pretreatment molecular diagnosis is recommended by clinical guidelines, to determine the eligibility of patients with advanced NSCLC for targeted therapies 6. The aim of this study was to establish a machine learning (ML) model to predict the EGFR status of BMs using preoperative brain MRI sequences and clinical data.Materials and Methods
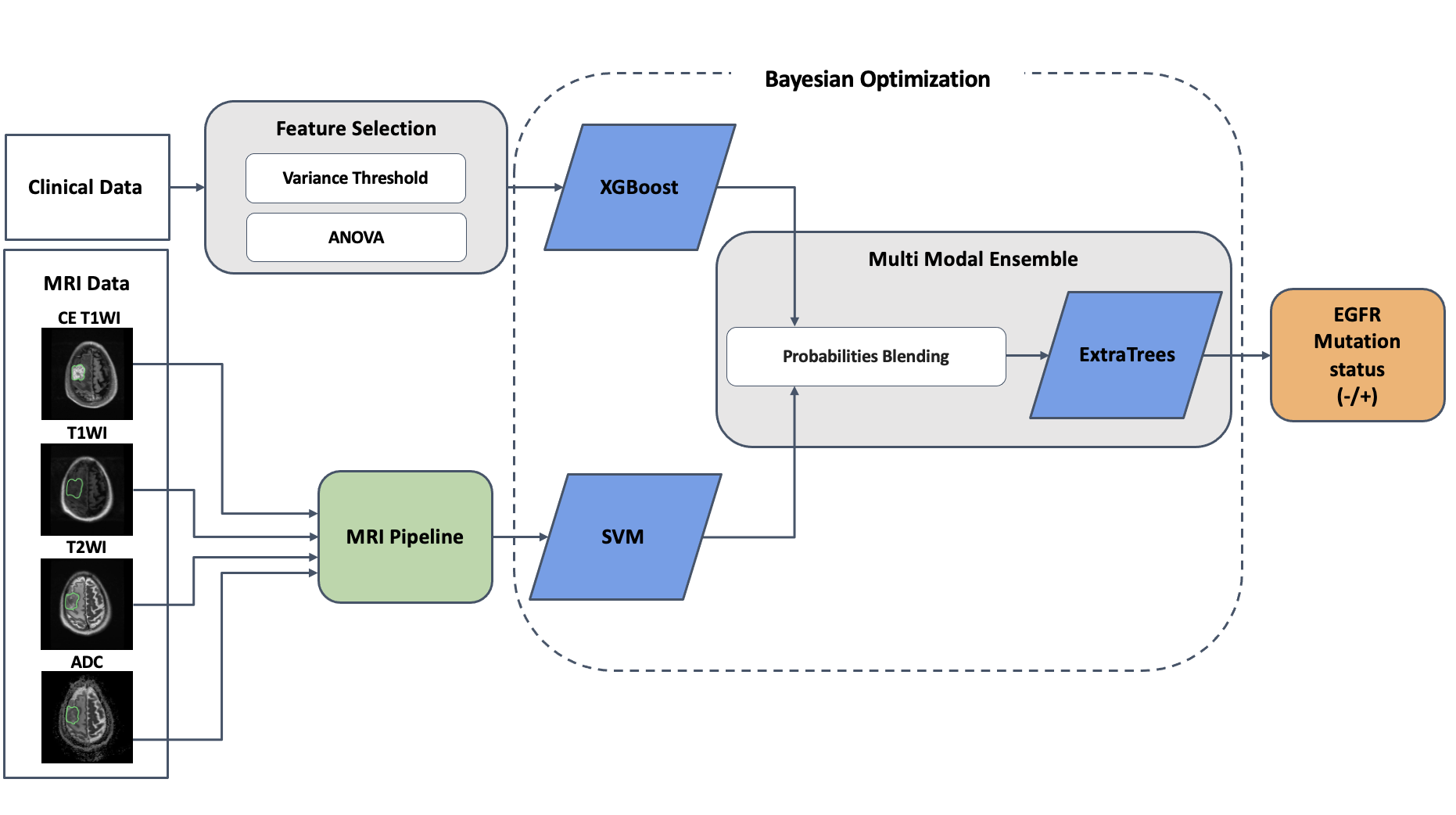
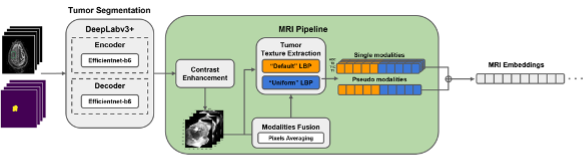
Data from 32 patients with resected BMs originating from lung cancer (20 with mutant EGFR, 12 with wild-type EGFR) were retrospectively analyzed. MR imaging features were extracted using preoperative brain MR images (contrast-enhanced T1-weighted imaging, CE T1WI; T1-weighted imaging, T1WI; T2-weighted imaging, T2WI; apparent diffusion coefficient, ADC) to establish ML-based models for predicting the EGFR status of excised BMs (24 cases for training, 4 cases for validation, and 4 cases for testing). Support Vector Machine (SVM) is selected for analysis of MRI 7, and XGBoost is for numerical clinical data 8. Besides, ExtraTrees is selected as the second-level model for fusing soft prediction from multi-modal data 9. After having multi-modal decisions from SVM, XGBoost, and ExtraTrees, a decision tree-based method is used and help ensemble the two decisions (Figures 1 and 2).Results
The results are summarized in Table 1. As compared to clinical data or MRI only, the best-performing ML model was a combination of clinical data and MRI features selected from multiple sequences (CE T1WI, T1WI, T2WI, and ADC). The accuracy, precision, and AUC of 0.89, 0.88, and 0.97 were obtained in the best predictive model. All metrics are averaged from the out-of-fold set over ten-fold cross-validation.Conclusions
This study attempted to use ML for the prediction of EGFR mutation status of BMs in lung cancer. Our results showed that ML based on pretreatment clinical data and brain MRI had the potential for predicting the EGFR mutation status in lung cancer BMs.Acknowledgements
NoneReferences
1. Villano JL, Koshy M, Shaikh H, Dolecek TA, McCarthy BJ. Age, gender, and racial differences in incidence and survival in primary CNS lymphoma. British journal of cancer. 2011;105(9): 1414-1418. https://doi.org/10.1038/bjc.2011.357.
2. Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9): 2892-2911.
3. Selvaggi G, Novello S, Torri V, et al. Epidermal growth factor receptor overexpression correlates with a poor prognosis in completely resected non-small-cell lung cancer. Ann Oncol. 2004;15(1): 28-32. https://doi.org/10.1093/annonc/mdh011.
4. Kris MG, Natale RB, Herbst RS, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer: a randomized trial. Jama. 2003;290(16): 2149-2158. https://doi.org/10.1001/jama.290.16.2149.
5. Lee CC, Soon YY, Tan CL, et al. Discordance of epidermal growth factor receptor mutation between primary lung tumor and paired distant metastases in non-small cell lung cancer: A systematic review and meta-analysis. PloS one. 2019;14(6): e0218414. https://doi.org/10.1371/journal.pone.0218414.
6. Le Rhun E, Guckenberger M, Smits M, et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann Oncol. 2021;32(11): 1332-1347. https://doi.org/10.1016/j.annonc.2021.07.016.
7. Hearst MA, Dumais ST, Osuna E, Platt J, Scholkopf B. Support vector machines. IEEE Intelligent Systems and their Applications. 1998;13(4): 18-28. https://doi.org/10.1109/5254.708428.
8. Chen T, Guestrin C. Xgboost: A scalable tree boosting system. Proceedings of the 22nd acm sigkdd international conference on knowledge discovery and data mining. 2016:785-794.
9. Geurts P, Ernst D, Wehenkel L. Extremely randomized trees. Machine learning. 2006;63: 3-42.
Figures