3769
An MRI-based nomogram predicts intracranial recurrence of brain metastases after surgery in lung cancer patients: A multicenter study1Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China, 2The First Affiliated Hospital of USTC, Hefei, China, 3The Tenth Affiliated Hospital of Southern Medical University, Dongguan People's Hospital, Dongguan, China, 4Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China, 5Capital Medical University, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence
Motivation: There is currently no reliable tool to predict postoperative recurrence for patients who undergo surgery for brain metastases (BrMs).
Goal(s): This study aimed to develop and externally validate a prognostic model to predict intracranial recurrence and recurrence-free survival (RFS) for lung cancer patients receiving BrM surgery.
Approach: A combined prognostic model-based nomogram was developed by incorporating clinical and structural MRI predictors, radiomics and deep signatures extracted from MR images.
Results: The nomogram predicted accurately for RFS and intracranial recurrence prediction, both in the training and test sets .
Impact: The combined prognostic model-based nomogram can be used as a preoperative tool to predict intracranial recurrence and recurrence-free survival after surgical resection of brain metastases in lung cancer patients.
Introduction
Brain metastases (BrMs) are the most prevalent intracranial malignancy, primarily caused by lung cancer1,2. Surgery is recommended to treat a limited number of BrMs3. Nevertheless, craniotomies can lead to severe complications4. Moreover, approximately 40% of BrMs recurred intracranially after surgical removal5. Unfortunately, there is a lack of models for predicting survival in lung cancer patients undergoing BrMs surgery. Therefore, the development of a reliable prognostic model for BrM resection is vital to guide the selection of eligible patients for surgical intervention.Methods
This study included 215 patients with 244 BrMs who underwent BrM surgical resection from five centers. They were divided into a training set of 167 patients (186 BrMs) at three centers and a test set of 48 patients (58 BrMs) from two centers. All patients underwent MRI examinations, including contrast-enhanced T1-weighted (CE-T1W) and T2-weighted (T2W) within 2 weeks before the surgery. Follow-up brain MRI scans were conducted every 3 months for the first year after BrM resection and thereafter every 6 months. Recurrence-free survival (RFS) was calculated from brain surgery to the occurrence of the first intracranial recurrence, death, or last follow-up. Radiologists evaluated ten structural MRI features for BrMs.Two radiologists manually delineated the enhanced edges on each slice of CE-T1WI using ITK-SNAP to generate the volume of interest (VOI) of BrMs. Then, the CE-T1WI-based VOIs were duplicated and aligned with the T2W images of BrMs to obtain the T2WI-based BrM VOI. After imaging normalization, 1595 radiomics features were obtained using the PyRadiomics toolkit, while, within each VOI, 3584 deep features were extracted using the MedicalNet models (https://github.com/Tencent/MedicalNet). Features with good agreement were included in the subsequent analysis. Using univariate and multivariable Cox proportional hazards regression to assess the clinical and structural MRI features associated with RFS in the training set, respectively. Radiomics features and deep features were selected using max-relevance and min-redundancy (mRMR) and least absolute shrinkage and selection operator (LASSO) Cox regression, respectively. Multicollinearity analysis was performed between these features. The combined prognostic model and other ensemble models were built based on the Cox regression coefficients. The ability of the combined model to predict RFS was evaluated using the calibration curve, Harrell's concordance index (C-index), continuous net reclassification improvement (NRI), Kaplan-Meier’s (K-M) survival analysis, time-dependent receiver operating characteristic (ROC) analyses, and decision curve analyses (DCA). A two-sided P < 0.05 indicates a significant difference.Results
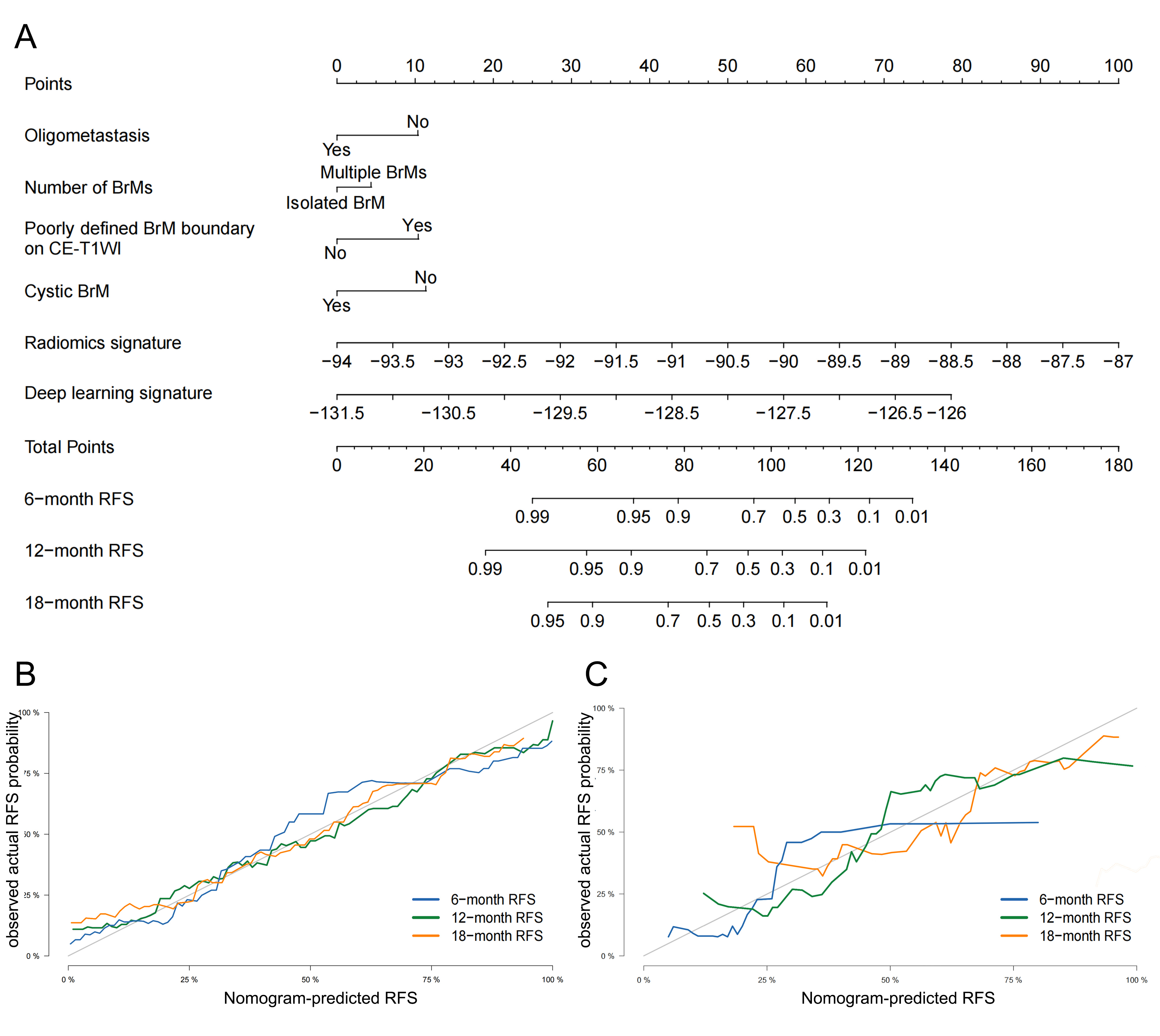
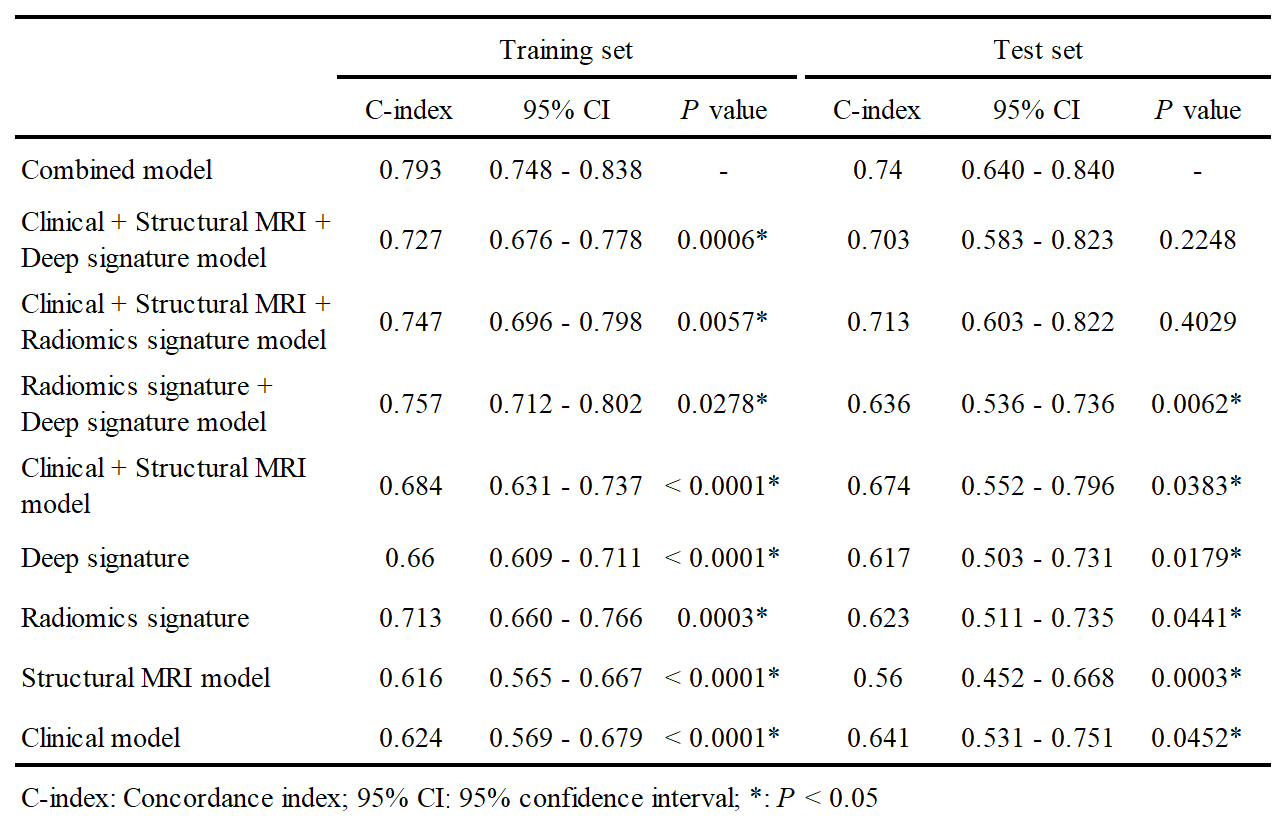
In clinical and structural MRI features, oligometastasis, number of BrMs, BrM boundary on CE-T1WI, and cystic BrM were independent predictors for RFS. 13 radiomics features and 10 deep features were selected as the most significant predictive features. The combined model was developed based on these features, and the nomogram is shown in Figure. 1.The combined model achieved the highest C-index for RFS prediction in the training and test sets. Its performance was significantly superior to models except clinical + structural MRI + deep signature model and clinical + structural MRI + radiomics signature model both in the training and test sets (P < 0.05) (Table 1). The continuous NRI revealed that the combined model outperformed these two in training and test sets.
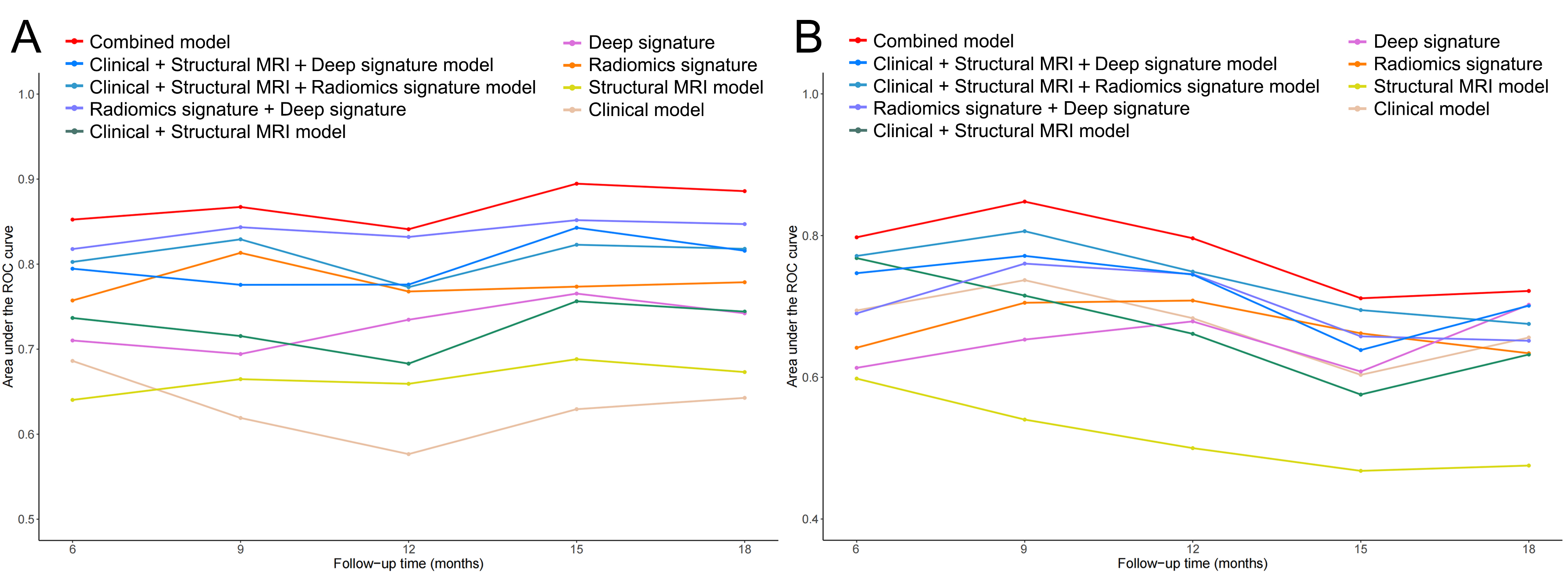
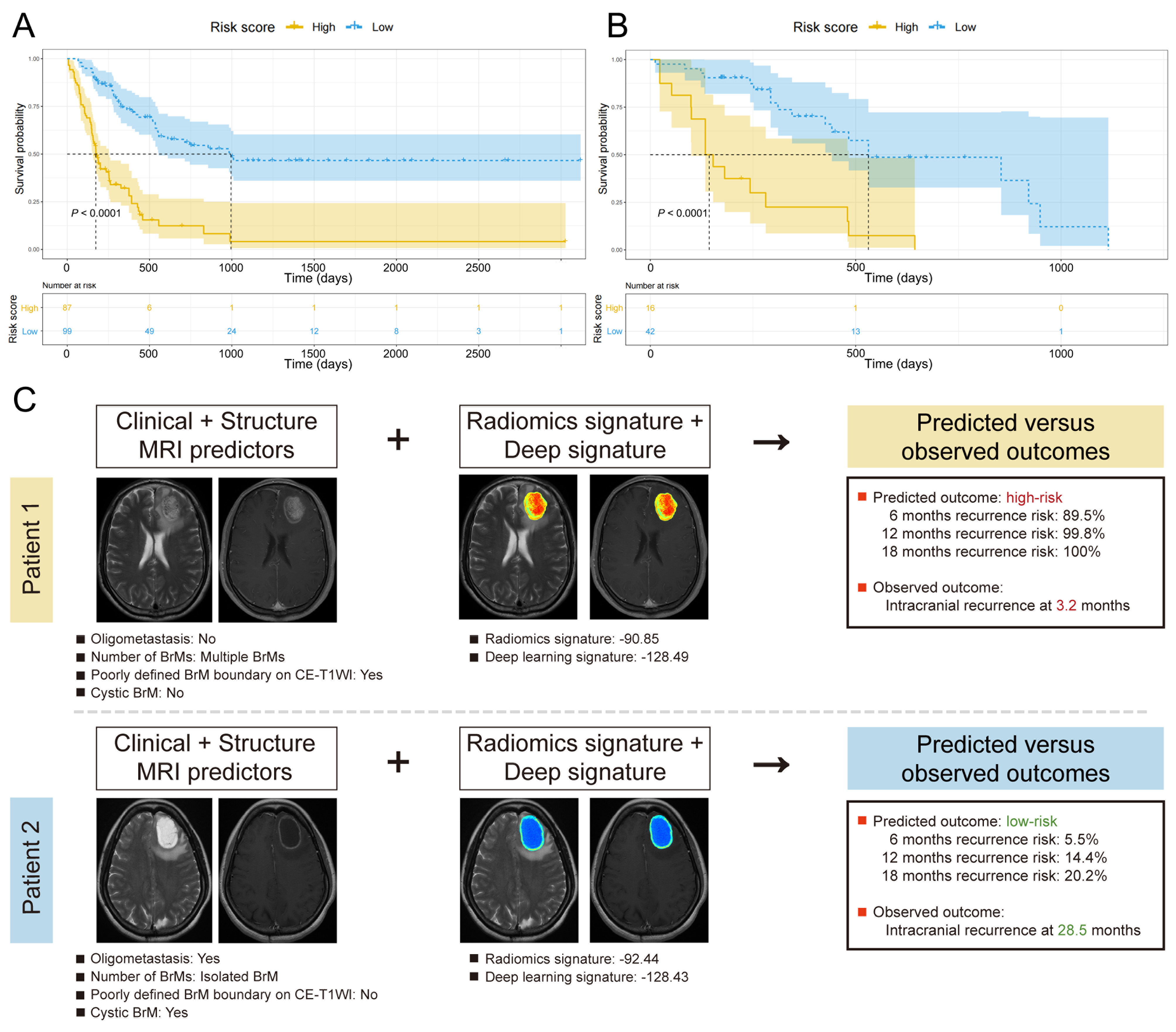
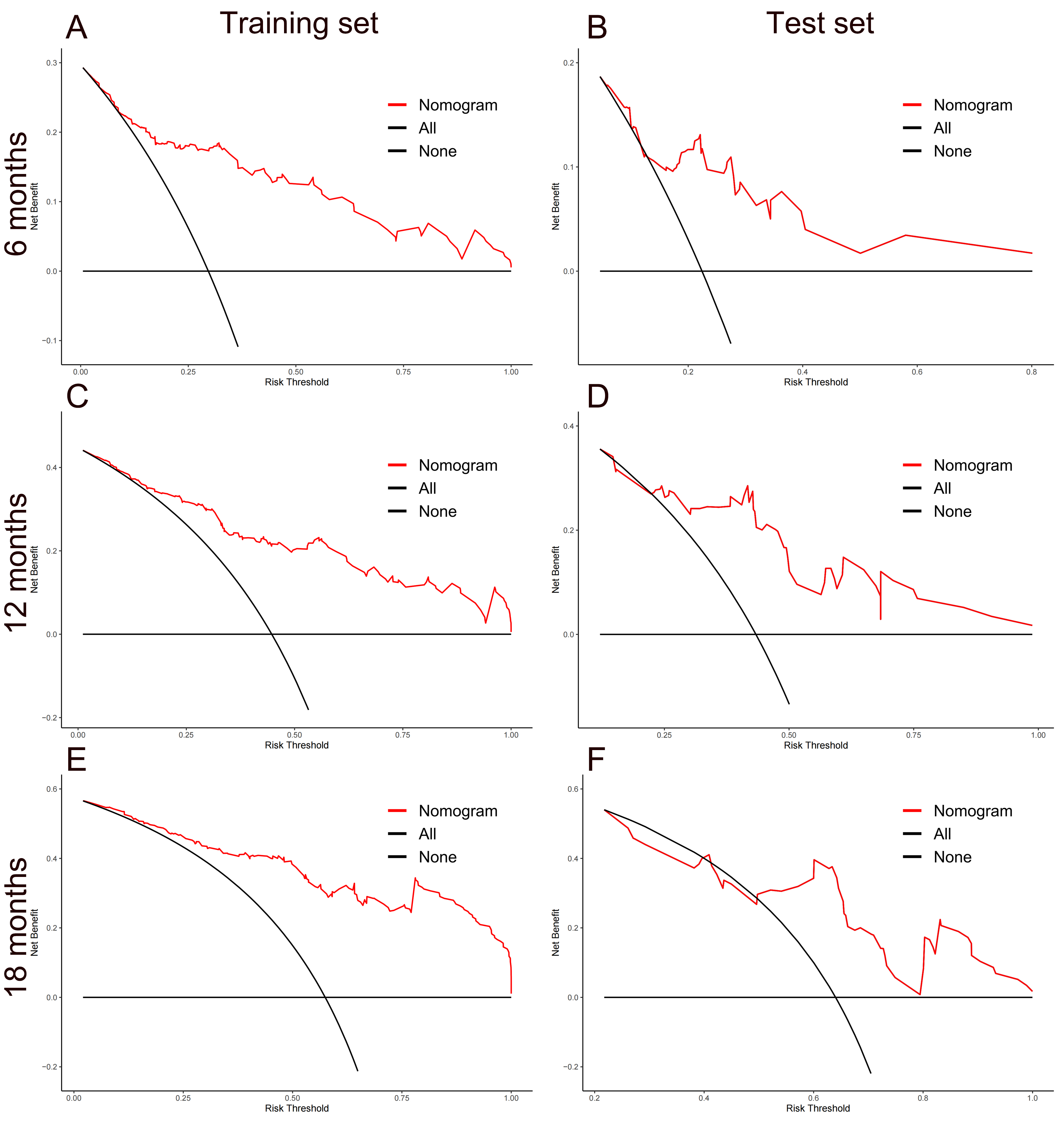
Time-dependent ROC curves confirmed that the combined model outperformed all other models in the training (AUCs: 0.841-0.895) and test sets (AUCs: 0.712-0.848) at 6-18 months after BrM resection (Fig. 2). The K-M curves indicated that patients in the low-risk group exhibited better RFS compared to high-risk patients in the training and test sets (both P < 0.05, Figure. 3A, B). DCA demonstrated that the combined model yielded a net benefit for 6-month, 12-month, and 18-month recurrence across the entire spectrum of threshold probabilities in the training set and within the threshold probabilities of > 13.2%, > 22.8%, and > 49.7% in the test set (Figure. 4). Two representative cases are displayed to demonstrate the prediction performance of the nomogram (Figure. 3C).
Discussion
In this multicenter study, an MRI-based nomogram was developed and externally validated to predict intracranial recurrence and RFS in lung cancer patients after surgical resection of BrMs. Incorporating both radiomics and deep signatures into the clinical + structural MRI model can further enhance the predictive capacity of MRI-based models. The result showed that this combined model provided a reliable tool to estimate the risk for intracranial relapse after BrM neurosurgery.Conclusion
The MRI-based nomogram can be used as a preoperative tool to predict intracranial recurrence after surgical resection of BrMs in lung cancer patients.Acknowledgements
No acknowledgement found.References
1. Lamba, N., Wen, P. Y. & Aizer, A. A. Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. 2021; 23:1447-1456.
2. Cagney, D. N. et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol. 2017; 19:1511-1521.
3. Suh, J. H. et al. Current approaches to the management of brain metastases. Nat Rev Clin Oncol. 2020;17:279-299.
4. Proescholdt, M. A. et al. The Management of Brain Metastases-Systematic Review of Neurosurgical Aspects. Cancers (Basel). 2021;13.
5. Jünger, S. T., Reinecke, D., Meissner, A. K., Goldbrunner, R. & Grau, S. Resection of symptomatic non-small cell lung cancer brain metastasis in the setting of multiple brain metastases. J Neurosurg. 2022;136:1576-1582.
Figures