3767
DeepDenoiseNet: a convolutional neural network trained with synthesized images from inversion-recovery maps for SASHA denoising1Shool of Medical Technology, Beijing Institute of Technology, Beijing, China, 2China Electronics Harvest Technology Co.,Ltd, Beijing, China, 3Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 4Department of Infectious Diseases, The Affiliated Hospital of Yan’an University, Yan’an, Shanxi, China
Synopsis
Keywords: Myocardium, Myocardium, SASHA
Motivation: SASHA T1 has high accuracy but low precision due to the low SNR of T1-weighted images. Convolutional neural network has the potential to improve SASHA T1 precision by using spatio-temporal correlations.
Goal(s): The aim of this study is to develope a convolutional neural network for improving SASHA T1 precision.
Approach: We implemented a convolutional neural network (DeepDenoiseNet) and trained it using synthesized SASHA images from co-registered high-quality T1, T2, and M0 images. Different-level noise was added to simulate low SNR SASHA images.
Results: DeepDenoiseNet could reduce the impaction from noise and improve SASHA T1 precision.
Impact: The deep convolutional neural network trained with synthesized images and simulated noise could improve SASHA T1 precision.
INTRODUCTION
Cardiovascular magnetic resonance T1 mapping enables the quantification of myocardium tissue properties, which has been considered a promising technique in heart disease diagnosis [1]. MOLLI and SASHA are two representative sequences for the inversion- and saturation-recovery techniques and are mostly used [2,3]. The accuracy of MOLLI is impacted by several confounders (e.g. heart rate, off-resonance, T2) and the adoption of the look-locker imaging scheme. Conversely, because of the low SNR, SASHA T1 has low precision but high accuracy which hinders its clinical applications [4]. Therefore, as a major step towards precision medicine for heart diseases, myocardial T1 mapping with high accuracy and precision still needs to be investigated.Recently, deep learning-based approaches have been proposed for myocardial T1 mapping on accuracy improvement, acceleration, and automatic analysis [5-7]. However, there is no study that sought to improve SASHA T1 precision through a deep convolutional neural network due to the lack of ground truth for training.
In this study, we sought to reduce noise in SASHA T1-weighted images by a deep convolutional neural network (DeepDenoiseNet) using synthesized training data.
METHODS
Training Datasets: Sixty-two co-registered T1 and T2 maps from 19 volunteers were used. There images are collected by a joint inversion and T2 preparation sequence on a 3T Philips scanner and approved by IRB. Written informed consent was obtained prior to scan. As shown in Figure 1, these images have less variation over the myocardium. For the data augmentation, a bias from -75ms to 75ms in a step of 10ms was added to each T1 map. Correspondingly, T2 bias was calculated from a normal distribution with a mean of 0ms and SD of 5ms. Totally, 992 co-registered T1, T2, and M0 were prepared.SASHA Bloch-equation simulation was performed for the training datasets (Figure 2A). For each simulation, co-registered T1, T2, and M0 maps mentioned above were used with 100%±20% saturation efficiency and 60bpm±7.5bpm heart rate. Each pixel was independently simulated with following parameters: bSSFP readout, 70 excitations for 2 acceleration, B1=0.7, TR/Flip angle=2.7/35°. For a given SNR, Gaussian noise was added to the real and imaginary parts of the signal to simulate Rician distribution. The SNR was ranged from 10-100 with a step of 10.
DeepDenoiseNet and training: as shown in Figure 2B, DeepDenoiseNet was designed as a U-shape deep convolutional neural network. The encoder includes 20 channels for ten T1-weighted images and corresponding saturation-recovery time. The input T1-weighted images were normalized to 0-1.1. The decoder has 10 channels for the denoised T1-weighted images. ReLU was used as an activation function.
We implemented DeepDenoiseNet on a DELL 7920 server with one Quadro RTX 5000 GPU. DeepDenoiseNet was trained with 300 epochs. The batch size was 2. Mean absolute error between output and reference T1-weighted images was calculated to update the DeepDenoiseNet at a learning rate of 0.001.
Validation and Testing datasets: SASHA phantom and in-vivo imaging were performed on a Philips 3.0T scanner using commonly adopted parameters. In-vivo imaging included 24 volunteers (16 males, 27±8yrs) with IRB approval. All participants provided written informed consent prior to scan. Reference T1 of phantom were measured by IR-SE. In-vivo images used in validation and testing were 140 slices and 220 slices, respectively. All phantom images were used in the validation for picking trained model with the best performance.
SASHA in-vivo T1 were calculated using 3-paremeter and 2-parameter models (3-Para and 2-Para). DeepDenoiseNet outputs were fitted by a 3-Para model.
RESULTS
The 219th epoch had the lowest mean absolute relative error and was used in the testing.In Figure 3 and Figure 4, DeepDenoiseNet could efficiently reduce noise in SASHA T1-weighted images and improve quality of T1 map. The variation across myocardium in T1 map was significantly reduced. Meanwhile, compared to SASHA T1 map by 2-Para, the detail of myocardium was not blurred serious.
In table 1, SASHA T1 had lower SD by DeepDenoiseNet than those by 2-Para and 3-Para, indicating the improved T1 precision.
DISCUSSION and CONCLUSION
In this study, we used co-registered T1, T2 and M0 from a joint inversion and T2-prep sequence to generate SASHA images for training. Because of inversion-recovery T1 has high precision [4], ideally, the synthetized SASHA images have high SNR and keep the details of tissue, and noise could be simulated in different levels. Therefore, these images could be used to teach the neural network to remove noise in SASHA T1 weighted images. Our results indicated DeepDenoiseNet could efficiently alleviate variation in SASHA in-vivo T1 map. Further research on accuracy is warranted.Acknowledgements
This work is supported by the National Natural Science Foundation of China for Young Scholars (No. 82202138), the Fundamental Research Funds for the Young Investigator (No. XSQD-202213003), and the Fundamental Research Funds for the Central Universities (No. LY2022-22).
References
1. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, Mascherbauer J, Nezafat R, Salerno M, Schelbert EB, Taylor AJ, Thompson R, Ugander M, van Heeswijk RB, Friedrich MG. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19(75).
2. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med 2004;52(1):141-146.
3. Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T(1) mapping. Magn Reson Med 2014;71(6):2082-2095.
4. Kellman P, Hansen MS. T1-mapping in the heart: accuracy and precision. J Cardiovasc Magn Reson 2014;16(22).
5. Guo R, El-Rewaidy H, Assana S, Cai X, Amyar A, Chow K, Bi X, Yankama T, Cirillo J, Pierce P, Goddu B, Ngo L, Nezafat R. Accelerated cardiac T1 mapping in four heartbeats with inline MyoMapNet: a deep learning-based T1 estimation approach. J Cardiovasc Magn Reson 2022;24(1):6.
6. Guo R, Chen Z, Amyar A, El-Rewaidy H, Assana S, Rodriguez J, Pierce P, Goddu B, Nezafat R. Improving accuracy of myocardial T1 estimation in MyoMapNet. Magn Reson Med 2022;88(6):2573-2582.
7. Fahmy AS, El-Rewaidy H, Nezafat M, Nakamori S, Nezafat R. Automated analysis of cardiovascular magnetic resonance myocardial native T1 mapping images using fully convolutional neural networks. J Cardiovasc Magn Reson 2019;21(1):7.
Figures
Figure 1. Co-registered M0, T1 and T2 obtained by a joint T1 and T2 sequence using inversion and T2 preparation pulse. Visually, these images have high quality, especially T1 map. In this study, we used these images to simulate SASHA T1-weighted images.
Figure 2. Over view of this study. A: co-registered in-vivo T1, T2 and M0 images by a joint inversion (IR) and T2 preparation (T2prep) are used to synthetize SASHA T1-weighted images using Bloch-equation simulation. These simulated signals with noise were used to train a convolutional neural network (DeepDenoiseNet). The trained DeepDenoiseNet was validated and tested by SASHA in-vivo images and phantom data. Comparison was made between maps from SASHA T1-weighted images before and after denoising.
Figure 3. SASHA T1-weighted images before and after denoising and corresponding T1 maps. The proposed method improved quality of T1 map.
Figure 4. T1 maps of three subjects imaged by SASHA. T1 map was built by three-parameter (3-Para) and two-parameter (2-Para) model. Images after DeepDenoiseNet was fitted by a 3-Para model. Maps from DeepDenoiseNet and 2-Para model had less variation across images than those by 3-Para model.
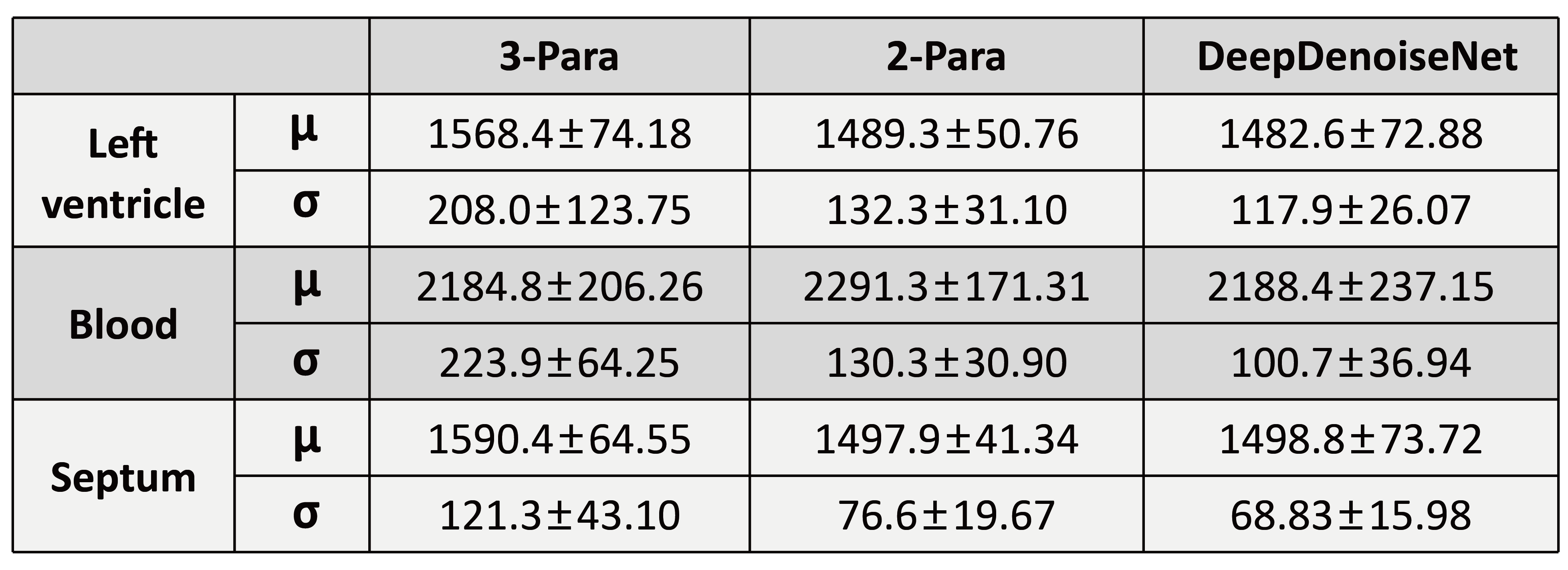
Table 1. The mean and SD of T1 averaged across all volunteers (N=22) in the testing dataset.