3761
SyntheticLGE.jl: An Open-Source Toolbox for Retrospective T1 Fitting and Synthetic LGE Image Generation1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Physical Sciences Platform, Sunnybrook Research Institute, Toronto, ON, Canada
Synopsis
Keywords: Synthetic MR, Cardiovascular, Late Gadolinium Enhancement, Synthetic MR
Motivation: Synthetic late gadolinium enhancement (SynLGE) has been proposed as a technique to quantify cardiac fibrosis from post-contrast T1 mapping. Current SynLGE techniques use site-specific code, limiting clinical adoption and standardization.
Goal(s): Develop a software toolbox for SynLGE image generation using retrospective T1* mapping.
Approach: An open-source software SyntheticLGE.jl was implemented in Julia and is publicly available on GitHub with two sample MOLLI datasets for software evaluation.
Results: SynLGE image generation is feasible for both SSFP and gradient-echo MOLLI imaging.
Impact: We hope that SyntheticLGE.jl can enable standardized and reproducible synthetic LGE image generation in simple and challenging clinical scenarios.
Introduction
Late gadolinium enhancement (LGE) imaging is a staple cardiac MRI sequence used to characterize myocardial fibrosis. Recently, synthetic LGE (SynLGE) has been proposed to generate an LGE image from post-contrast T1 mapping1,2,3. “Conventional” methods for SynLGE generation calculate the images directly from the outputted T1 map using the formula$$M({\rm TI}) = 1 - 2\exp(-{\rm TI}/T_1) (1)$$
for phase-sensitive (PSIR) reconstruction and $$$|M({ \rm TI})|$$$ for magnitude reconstruction. Recent work in synthetic cardiac phase-resolved LGE4 demonstrates the utility of retrospective two-parameter $$$(M_0^*, T_1^*)$$$ fitting to the formula
$$M({\rm TI}) = M_0^*( 1 - 2\exp(-{\rm TI}/T_1^*)). (2)$$
The constant 2 can be replaced with a fitting parameter $$$B$$$ for three-parameter fits. Current SynLGE image generation is performed using site-specific code, which inhibits standardization and adoption. In this submission, we present an open-source library called SyntheticLGE.jl, which provides an integrated Julia environment for synthetic LGE image generation compatible with the DICOM standard.
Methods
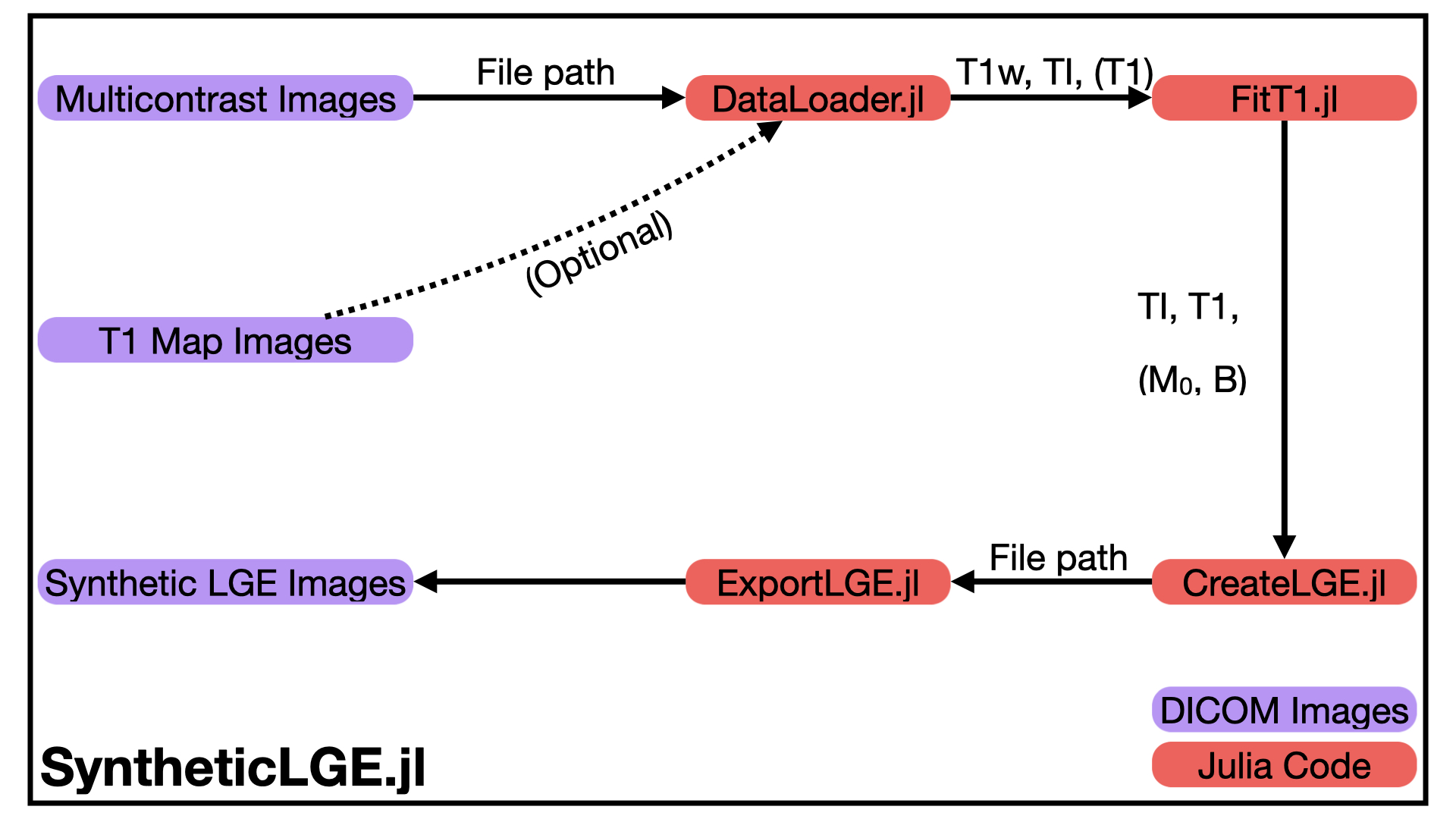
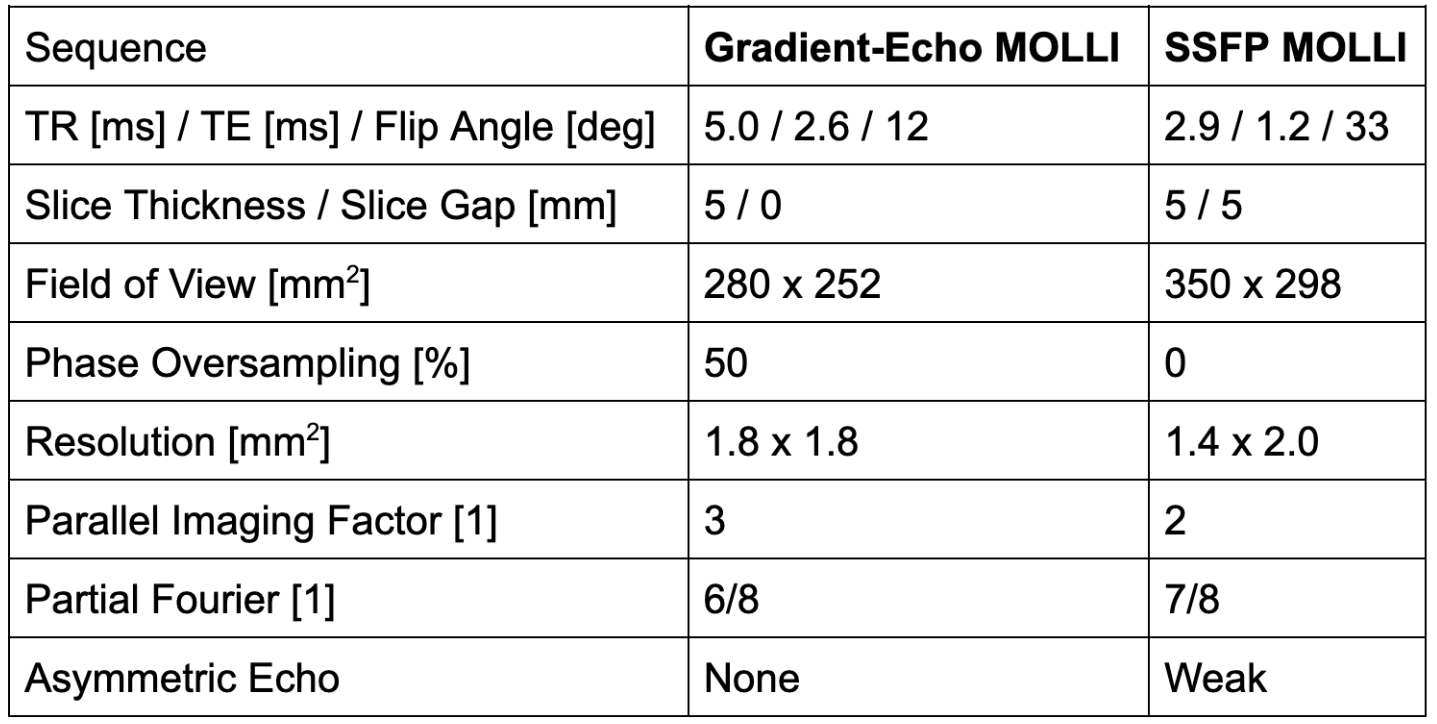
SyntheticLGE.jl was implemented in Julia, a free and open-source programming language that combines high-level syntax with just-in-time compilation for ease of readability and rapid performance5. The built-in @threads macro was used for CPU multithreading when looping over voxel indices [i, j, k]. Several SynLGE generation methods are implemented: conventional SynLGE using Equation (1); two-parameter fitting to Equation (2); and three-parameter fitting to Equation (2). Fitting was performed using the LsqFit.jl package, which employs the Levenberg-Marquardt optimizer. For more information on the software workflow, see Figure 1.Two sample datasets from the same subject are included with this package for demonstration purposes. One Yorkshire pig (F, weight 53kg) was imaged at 3 Tesla (Biograph mMR, Siemens Healthineers AG, Germany) five weeks after a simulated myocardial infarction modeled by a balloon occlusion of the left anterior descending artery. Two variations of a Modified Look-Locker (MOLLI) T1 mapping sequence were performed after the administration of gadobutrol (Gadavist, Bayer Healthcare, USA): an SSFP MOLLI and a prototype wideband gradient-echo MOLLI [6] imaged with an externally taped defibrillator (Cognis 100D, Boston Scientific, USA). For more details on sequence parameters, see Table 2.
Results
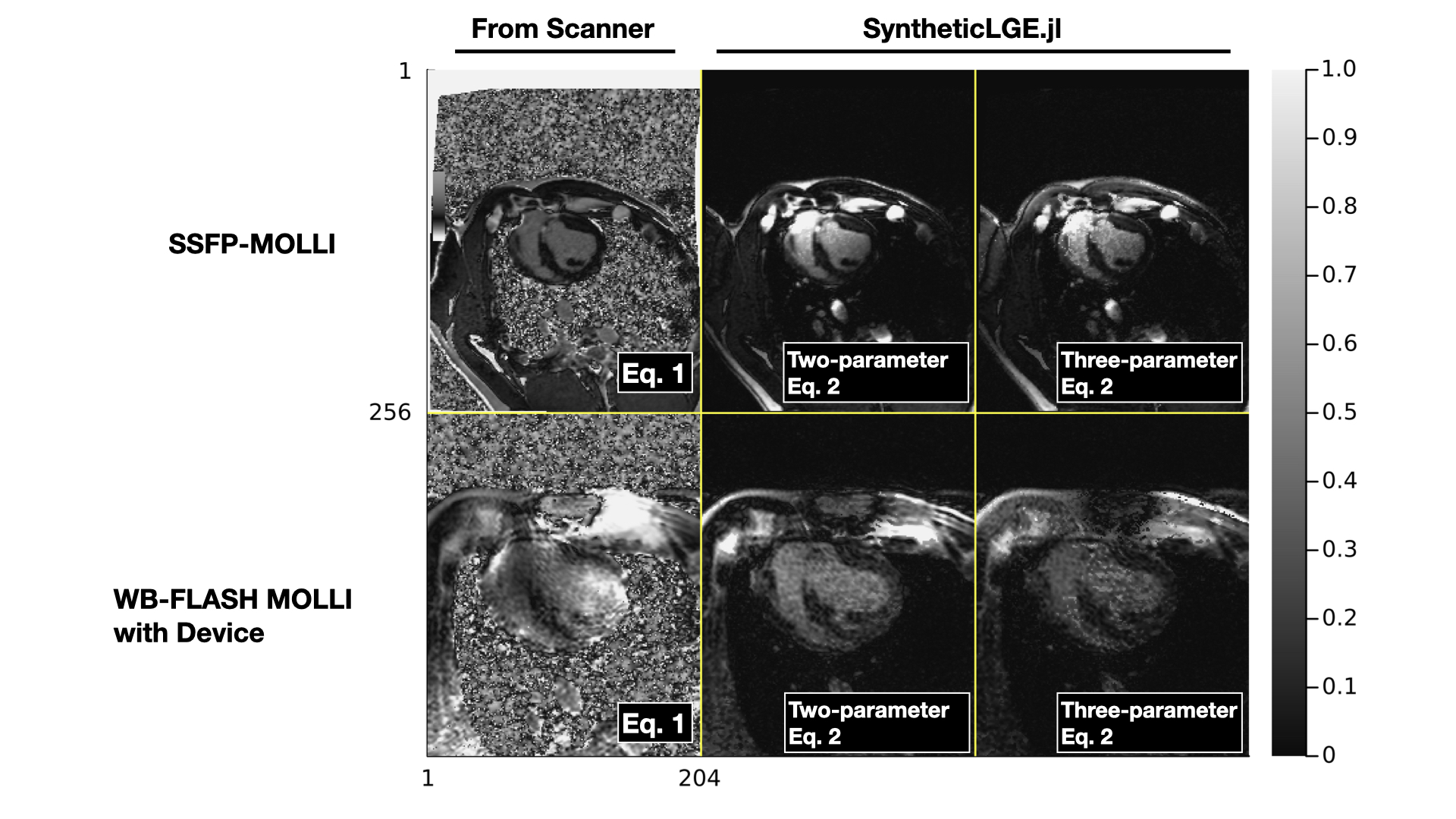
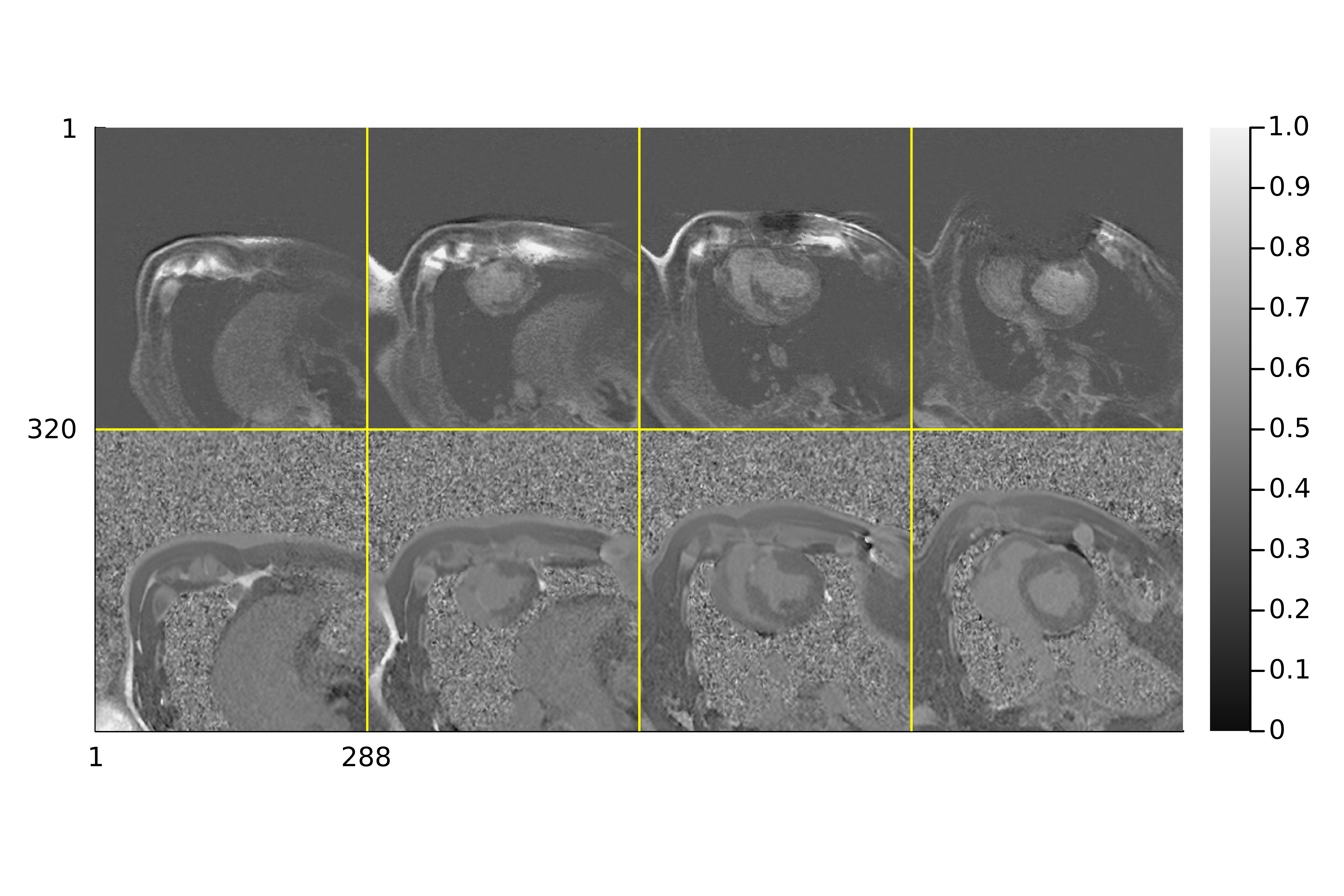
SyntheticLGE.jl is available at https://github.com/WrightGroupSRI/SyntheticLGE.jl. Julia code installs successfully, and the demonstration script runs without error when used by a second Julia user not involved with software prototyping. The most computationally intensive step in a representative pipeline, two-parameter T1 mapping, requires 3 seconds per slice to run, which is feasible in clinical practice. Code to generate the figures in this manuscript is available in the docs/ismrm/figures folder, and utilized the MIRTjim library for plotting.Figure 3 demonstrates sample image quality for conventional SynLGE reconstruction, two-parameter fitting, and three-parameter fitting for magnitude and phase-sensitive reconstructions. Two-parameter fitted images demonstrate good image quality for both MOLLI variants, with improved image quality over three-parameter fitted images. Conventional SynLGE reconstruction provides optimal image quality for SSFP-MOLLI due to the reduction in coil shading artifacts, but is non-diagnostic for wideband gradient-echo MOLLI.
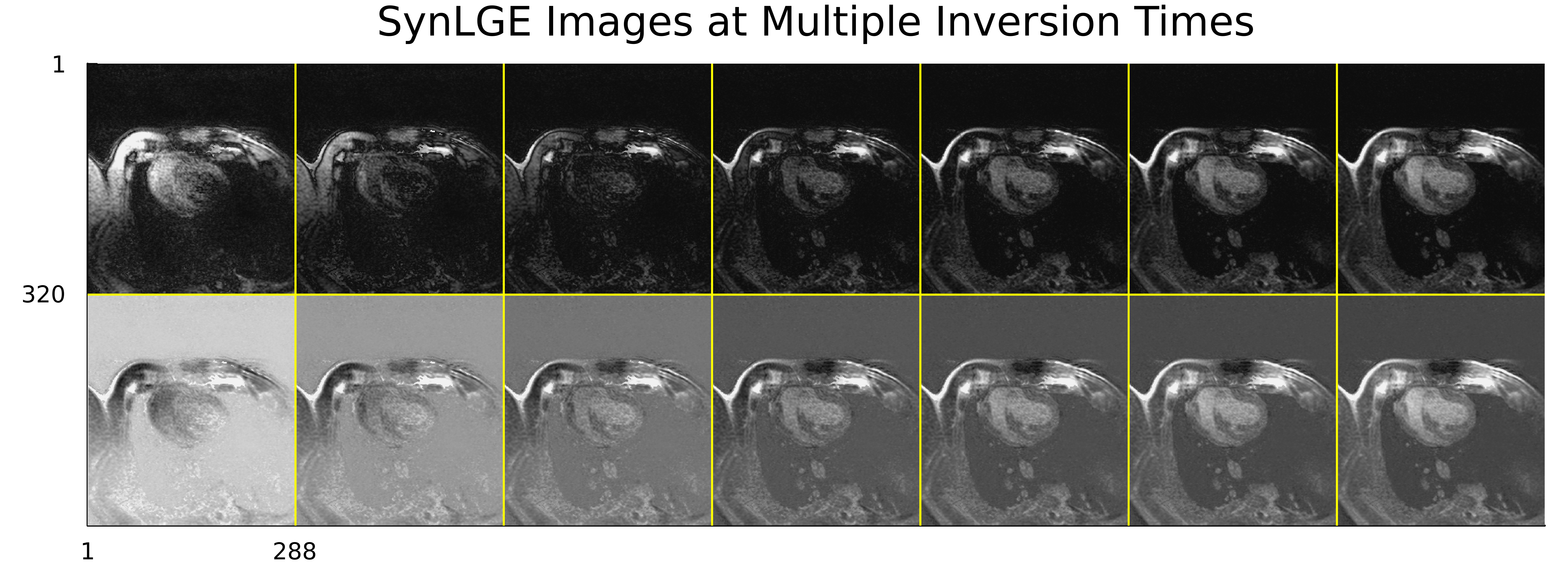
Figure 4 demonstrates the flexible reconstruction at multiple inversion times in both magnitude and phase-sensitive reconstruction. Proper inversion time selection is important to ensure good contrast between healthy myocardium, blood pool, and dense fibrosis.
Figure 5 exhibits a comparison of synthetic PSIR LGE images reconstructed with our software and reference PSIR images, displaying similar contrast and image quality. Device artifacts are spatially localized and do not obscure the myocardium and fibrosis in clinically relevant regions.
Discussion
In this abstract, a software library called SyntheticLGE.jl was proposed for retrospective $$$M_0, T_1^*$$$ fitting and SynLGE image generation. Performance was demonstrated on two porcine datasets across image processing strategies, with similar computation times as C++ implementations.This study has several limitations. Similar to magnitude LGE, synthetic LGE requires a choice of optimal inversion time, which is dependent on the time since gadolinium injection. However, this choice can be performed retrospectively, allowing for reduced scan time and improved flexibility in image analysis. This software only supports inversion-recovery $$$T_1^*$$$ mapping; we aim to support saturation-recovery T1 mapping in the future. Image quality in gradient-echo MOLLI may be improved by incorporating denoising libraries that improve SNR while preserving physiological edges7. Finally, while the DICOM standard is convenient, integrating this framework into the MRD standard8,9 would allow for on-scanner reconstructions, although an automated method will be needed to determine the optimal inversion time.
Conclusion
In conclusion, the SyntheticLGE.jl software library has been successfully implemented with demonstrated functionality for SSFP and gradient-echo MOLLI. Future work will improve the software platform flexibility and SynLGE image quality.Acknowledgements
This work is supported by the Canadian Institutes of Health Research (CDS, JHP, GAW) and the National Sciences and Engineering Research Council of Canada (BTTT, AZL). CDS, JHP, and GAW receive research funding from GE Healthcare and Vista AI and non-monetary research support from Siemens Healthineers.References
1. Hong, K., DiBella, E., Kholmovski, E. et al, Synthetic LGE derived from cardiac T1 mapping for simultaneous assessment of focal and diffuse cardiac fibrosis. Journal of Cardiovascular Magnetic Resonance (2014).
2. Abdula, G., Nickander, J., Sörensson, P. et al, Synthetic late gadolinium enhancement cardiac magnetic resonance for diagnosing myocardial scar. Scandinavian Cardiovascular Journal (2018).
3. Lee, S., Kim, P., Im, D.J. et al, The image quality and diagnostic accuracy of T1-mapping-based synthetic late gadolinium enhancement imaging: comparison with conventional late gadolinium enhancement imaging in real-life clinical situation. Journal of Cardiovascular Magnetic Resonance (2022)
4. Weingärtner, S., Demirel, Ö., Gama, F., et al, Cardiac phase-resolved late gadolinium enhancement imaging. Frontiers in Cardiovascular Medicine (2022).
5. Bezanson, J., Karpinski, S., Shah, V., and Edelman, A., Julia: A Fast Dynamic Language for Technical Computing. arXiv:1209.5145 (2012).
6. Shao, J., Rashid, S., Renella, P., et al, Myocardial T1 mapping for patients with implanted cardiac devices using wideband inversion recovery spoiled gradient echo readout. Magnetic Resonance in Medicine (2016).
7. Athavale, P., Xu, R., Radau, P., et al, Multiscale properties of weighted total variation flow with applications to denoising and registration. Medical Image Analysis (2015).
8. Hansen, M.S. and Sorenson, T.S., Gadgetron: An open source framework for medical image reconstruction. Magnetic Resonance in Medicine (2012).
9. Inati, S.J., Naegele, J.D., Zwart, N.R., et al, ISMRM Raw data format: A proposed standard for MRI raw datasets. Magnetic Resonance in Medicine (2016).
Figures