3755
Predicting the efficacy of induction chemotherapy for nasopharyngeal carcinoma: histogram analysis of quantitative synthetic MRI1Chongqing University Cancer Hospital, School of Medicine, Chongqing University, Chongqing, China, 2GE HealthCare MR Research, Beijing, China
Synopsis
Keywords: Synthetic MR, Quantitative Imaging, nasopharyngeal carcinoma
Motivation: In nasopharyngeal carcinoma (NPC) patients, there is a significant variation in tumor response to induction chemotherapy (ICT), which directly impacts prognosis. To address this issue, we aimed to explore a novel imaging biomarker based on pre-treatment synthetic MRI to predict which patients would benefit the most from the additional ICT.
Goal(s): Evaluating the value of pre-treatment synthetic MRI quantitative parameter map histogram characteristics in predicting the efficacy of ICT for NPC.
Approach: 40 NPC patients were prospectively enrolled, and each was imaged with synthetic MRI.
Results: T2_Minimun and T2_RootMeanSquared show promise as imaging markers for predicting the response to ICT in NPC.
Impact: The utilization of synthetic MRI may serve as an effective diagnostic tool for evaluating the response to ICT in clinical practice. Identifying patients who are unlikely to respond to ICT early on, can help offer them alternative treatment options.
Introduction
Induction chemotherapy (ICT) followed by concurrent chemoradiotherapy (CCRT) or CCRT alone are both now recommended for locoregionally advanced nasopharyngeal carcinoma (NPC) in 2023 CACA guideline1. While ICT+CCRT has shown improved patient prognosis, it is associated with high toxicity and side effects2-4. Additionally, a significant portion of patients (10%) exhibit a poor response to treatment, resulting in NPC treatment failure5. Therefore, predicting the patient's response to ICT before treatment and adjusting the treatment plan can avoid unnecessary treatment and side effects. Synthetic MRI (SyMRI) is a cutting-edge technique capable of generating T1, T2, and PD maps, as well as synthesizing multiple contrast-weighted images, all within a clinically feasible time frame6. Moreover, histogram analysis can provide multiple parameters reflecting tumor heterogeneity and changes in the tumor microenvironment. Recent studies have successfully applied histogram analysis of SyMRI to investigate prognostic factors in breast cancer, nasopharyngeal cancer, and rectal cancer7-9. However, no research has yet examined the therapeutic effect of NPC using this approach. Therefore, the purpose of our study is to investigate the predictive value of histogram characteristics derived from quantitative parameters obtained through SyMRI in NPC patients after ICT.Materials and Methods
This prospective study was approved by the Ethics Committee of our hospital, and informed consent was obtained from all patients before MRI examination.Patients
40 NPC patients were prospectively enrolled. The Response Evaluation Criteria in Solid Tumors (RECIST1.1) guidelines were used to evaluate the efficacy: patients with partial response (PR) and complete response (CR) were defined as effective group, and stable disease (SD) was defined as ineffective group.
MRI Acquisition
MRI was performed using a 3T scanner (SIGNATM Premier, GE Healthcare) with a 48-channel head and neck unite coil. SyMRI, the parameters were as follows: TR, 4000 ms; TE, 16.0/89.4 ms; slice thickness/ gap, 3.0/0mm; FOV, 180 mm; acquisition matrix, 192 × 192; NEX, 1; acquisition time, 4 min 32 s. Data Analysis The acquired raw images were processed using SyMRI software (version 8.0, Synthetic MR) to generate three quantitative maps (T1 map, T2 map, and PD map). ITK-SNAP software is used to outline volumes of interest (VOIs), 3D Slicer software to extract histogram features.
Data Analysis
All statistical analyses were performed using SPSS 26.0 software and MedCalc 19.8. The Kolmogorov–Smirnov test was adopted to assess whether the continuous variable was normally distributed. the histogram parameters were compared between two groups using Student’s t test or Mann–Whitney U test. Then, parameters with statistically significant differences were included in multivariate logistic regression analysis. the receiver operating characteristic (ROC) curve was generated based on the significant features, and the area under the curve (AUC), sensitivity, and specificity were reported.
Results
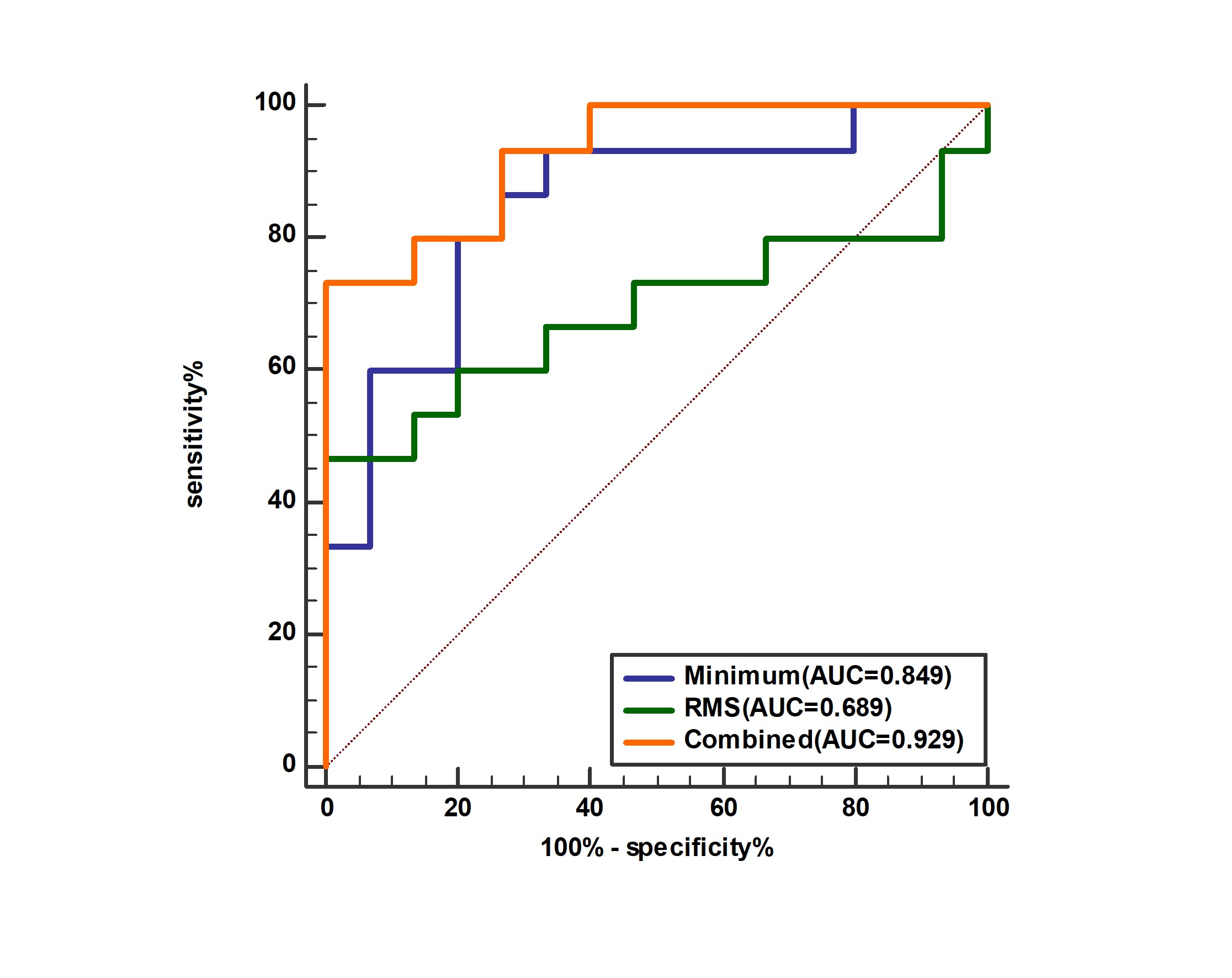
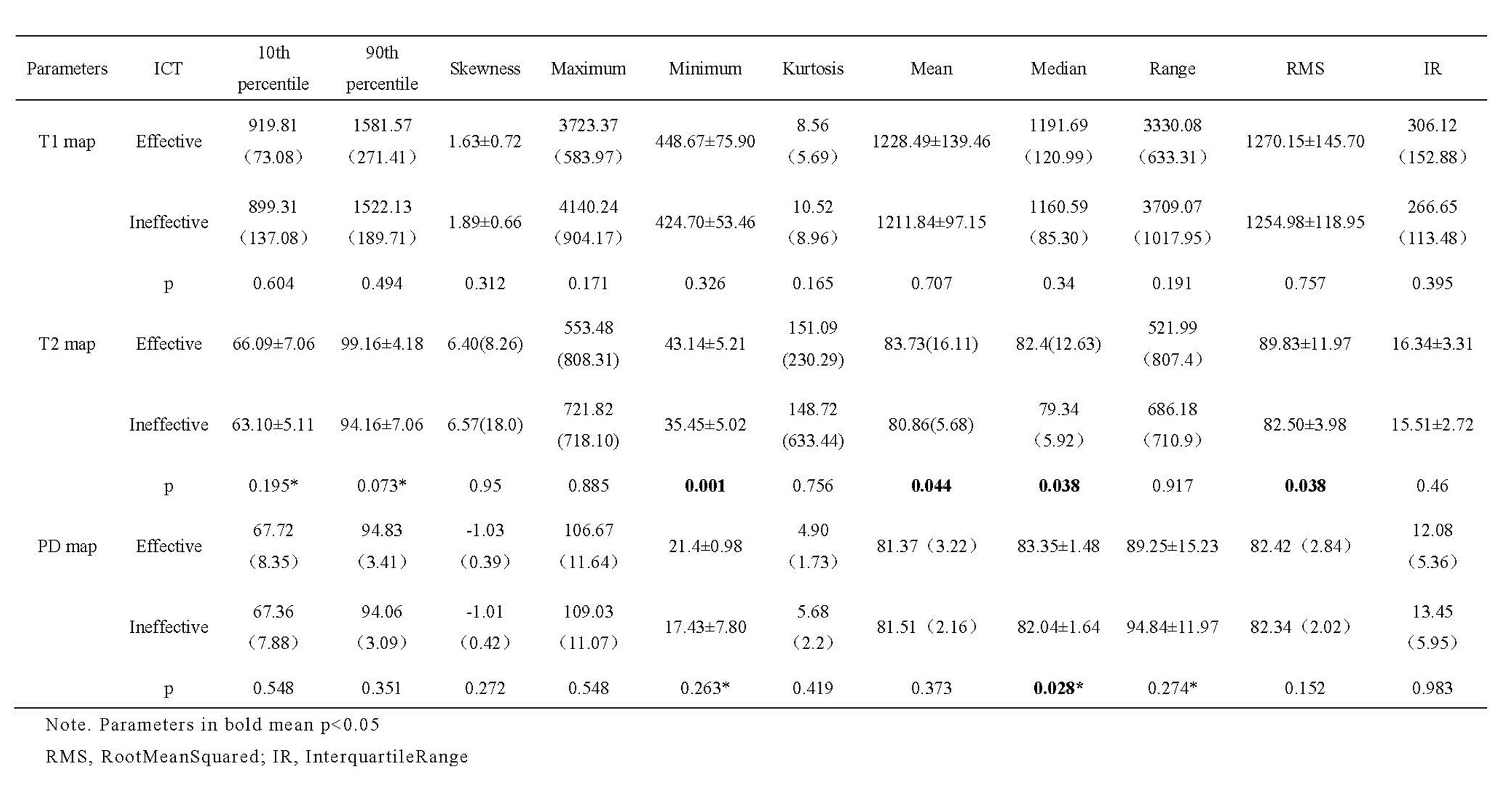
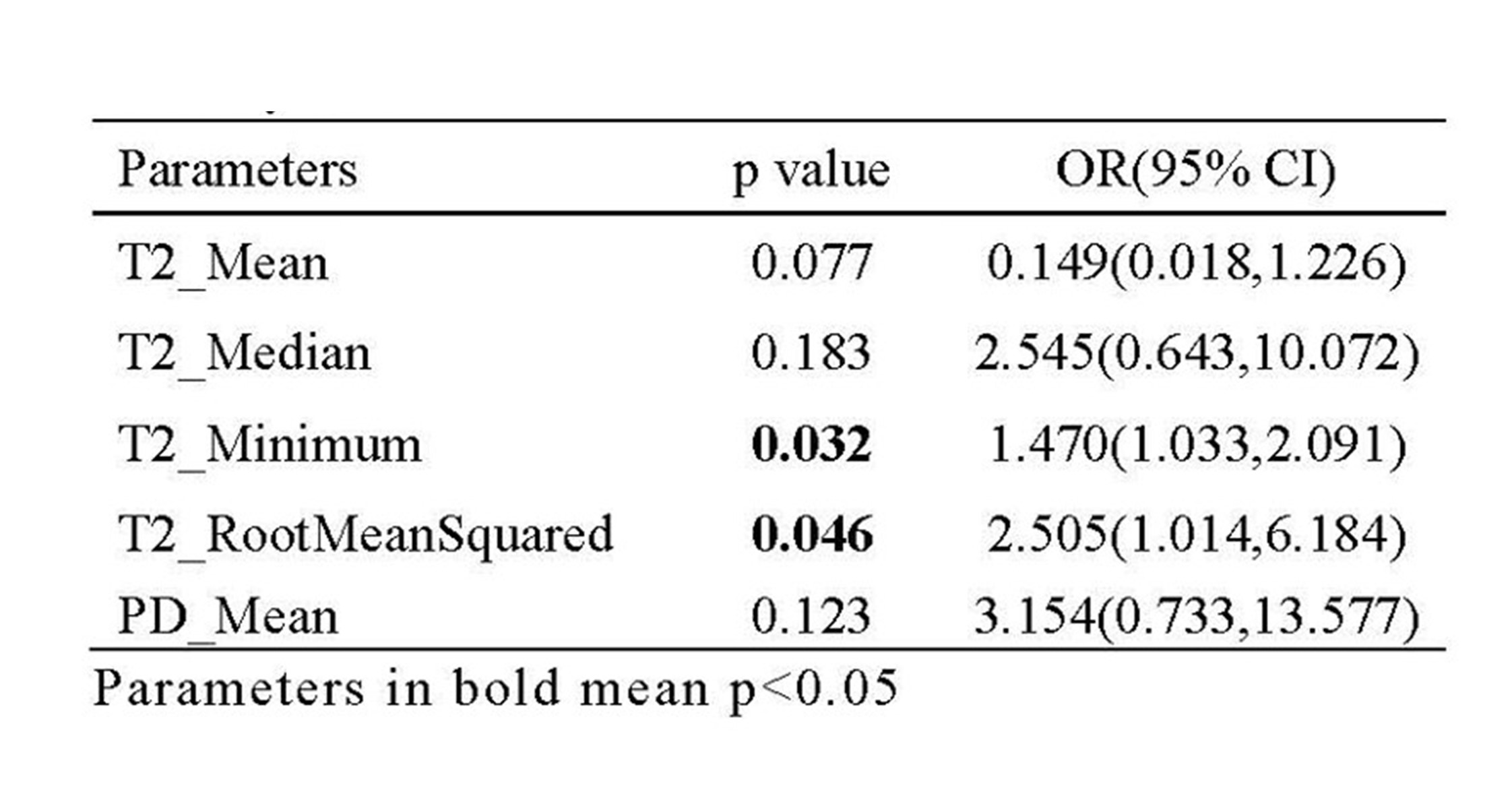
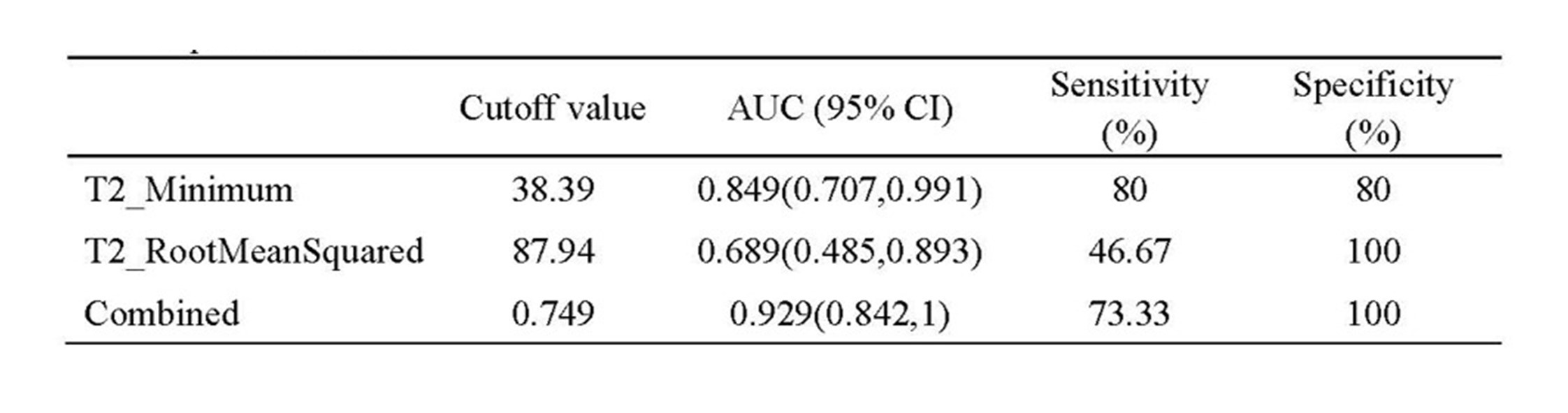
Table 1 showed that there were significant differences in T2_Mean, T2_Median, T2_Minimum, T2_RootMeanSquared and PD_Mean between the effective and the ineffective group (P< 0.05). Multivariate analysis demonstrated that T2_Minimum(P=0.032) and T2_RootMeanSquared(P=0.046) were the independent prediction factor for predicting the response to ICT in NPC (Table 2). Clinical examples are provided in Figure 1.The ROC analysis showed the AUC of T2_RootMeanSquared (AUC = 0.689) was slightly lower than that of T2_Minimum (AUC 0.849, P= 0.118), the AUC of T2_Minimum (AUC = 0.849) was slightly lower than that of combined (AUC 0.929, P= 0.167). Combined demonstrated the optimal performance with AUC of 0.929, which was significantly higher than T2_Minimum (AUC = 0.849, P= 0.01) (Table 3, Figure2)
Discussion and Conclusion
ICT plays a crucial role in the treatment of patients with locally advanced NPC, as the response to ICT is closely associated with long-term prognosis. Our study revealed that T2_Minimun and T2_RootMeanSquared are independent predictors of the effectiveness of ICT for NPC, and the model of T2_Minimun and combined parameters has high predictive efficiency.T2 relaxation time, a tissue-specific magnetic resonance parameter, was found to be informative in our analysis. We observed significantly lower histogram parameters derived from the T2 map in the ineffective group compared to the effective group. Tumors with lower T2 values usually have a higher cellular density, lymphocyte/plasma cell infiltration, and necrotic materials in the intercellular space, which might cause reduced extracellular space and free water content in tissue, resulting in shorter T2 values10. Many previous studies have found that high-grade tumors have lower T2 values than low-grade tumors and are more heterogeneous11,12. We speculate that intra-tumor heterogeneity may contribute to differences in efficacy.
In summary, the histogram parameters derived from baseline syMRI were found to be promising imaging markers for predicting the response to ICT in NPC. This suggests that syMRI could serve as a valuable diagnostic tool for evaluating ICT response in clinical practice.
Acknowledgements
No acknowledgement found.References
1. Tang L-L, Chen L, Hu C-S, Yi J-L, Li J-G, He X, Jin F, Zhu X-D, Chen X-Z, Sun Y et al: CACA guidelines for holistic integrative management of nasopharyngeal carcinoma. Holistic Integrative Oncology 2023, 2(1).
2. Sun Y, Li W-F, Chen N-Y, Zhang N, Hu G-Q, Xie F-Y, Sun Y, Chen X-Z, Li J-G, Zhu X-D et al: Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase3, multicentre, randomised controlled trial. The Lancet Oncology 2016, 17(11):1509-1520.
3. Chen Y-P, Tang L-L, Yang Q, Poh S-S, Hui EP, Chan ATC, Ong W-S, Tan T, Wee J, Li W-F et al: Induction Chemotherapy plus Concurrent Chemoradiotherapy in Endemic Nasopharyngeal Carcinoma: Individual Patient Data Pooled Analysis of Four Randomized Trials. Clinical Cancer Research 2018, 24(8):1824-1833.
4. Zhang Y, Chen L, Hu G-Q, Zhang N, Zhu X-D, Yang K-Y, Jin F, Shi M, Chen Y-P, Hu W-H et al: Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. New England Journal of Medicine 2019, 381(12):1124-1135.
5. Peng H, Chen L, Li WF, Guo R, Mao YP, Zhang Y, Guo Y, Sun Y, Ma J: Tumor response to neoadjuvant chemotherapy predicts long‐term survival outcomes in patients with locoregionally advanced nasopharyngeal carcinoma: A secondary analysis of a randomized phase 3 clinical trial. Cancer 2016, 123(9):1643-1652.
6. Warntjes JBM, Dahlqvist O, Lundberg P: Novel method for rapid, simultaneous T1, T*2, and proton density quantification. Magnetic Resonance in Medicine 2007, 57(3):528-537.
7. Lian S, Liu H, Meng T, Ma L, Zeng W, Xie C: Quantitative synthetic MRI for predicting locally advanced rectal cancer response to neoadjuvant chemoradiotherapy. European Radiology 2022, 33(3):1737-1745.
8. Yang F, Li X, Li Y, Lei H, Du Q, Yu X, Li L, Zhao Y, Xie L, Lin M: Histogram analysis of quantitative parameters from synthetic MRI: correlations with prognostic factors in nasopharyngeal carcinoma. European Radiology 2023, 33(8):5344-5354.
9. Zhao R, Du S, Gao S, Shi J, Zhang L: Time Course Changes of Synthetic Relaxation Time During Neoadjuvant Chemotherapy in Breast Cancer: The Optimal Parameter for Treatment Response Evaluation. Journal of Magnetic Resonance Imaging 2023, 58(4):1290-1302.
10. Gao W, Zhang S, Guo J, Wei X, Li X, Diao Y, Huang W, Yao Y, Shang A, Zhang Y et al: Investigation of Synthetic Relaxometry and Diffusion Measures in the Differentiation of Benign and Malignant Breast Lesions as Compared to BI‐RADS. Journal of Magnetic Resonance Imaging 2020, 53(4):1118-1127.
11. Cui Y, Han S, Liu M, Wu Py, Zhang W, Zhang J, Li C, Chen M: Diagnosis and Grading of Prostate Cancer by Relaxation Maps From Synthetic MRI. Journal of Magnetic Resonance Imaging 2020, 52(2):552-564.
12. Cai Q, Wen Z, Huang Y, Li M, Ouyang L, Ling J, Qian L, Guo Y, Wang H: Investigation of Synthetic Magnetic Resonance Imaging Applied in the Evaluation of the Tumor Grade of Bladder Cancer. Journal of Magnetic Resonance Imaging 2021, 54(6):1989-1997.
Figures
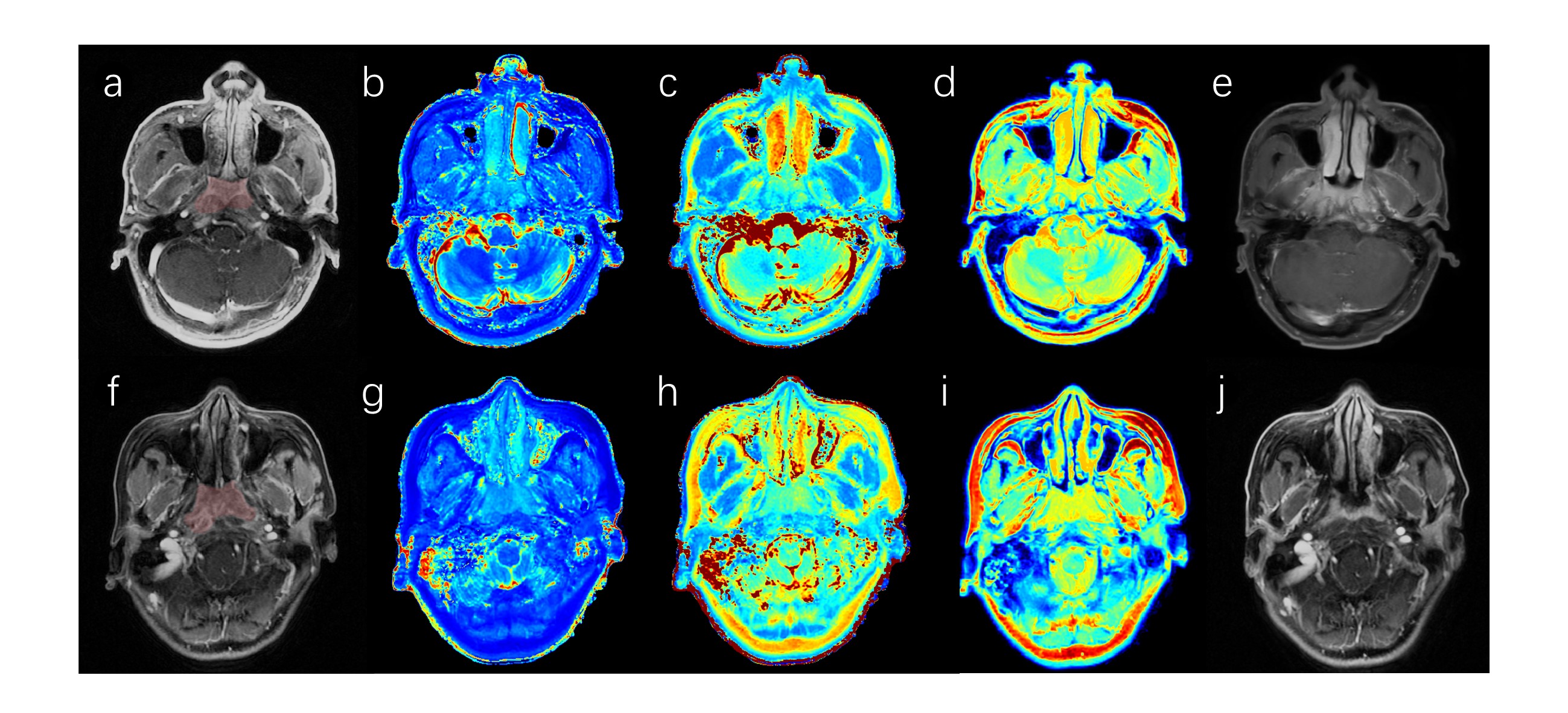
Figure1 Male,35-year-old, MRI images of nasopharyngeal carcinoma before treatment (a-d). a: Volumes of interest (VOI) in the tumor of the DCE-MRI; b-d: T1-mapping, T2-mapping and PD-mapping; e: 3 cycles of induction chemotherapy, the tumor subsided and the efficacy was evaluated as effective.
Female,48-year-old, MRI images of nasopharyngeal carcinoma before treatment (f-i). f: VOI in the tumor of the DCE-MRI; g-i: T1-mapping, T2-mapping and PD-mapping; j: 2 cycles of induction chemotherapy, the tumor no subsided and the efficacy was evaluated as ineffective.