3745
Approach to Improving Anatomical Accuracy of Numerical Body Models Repositioned to Match Subject Posture During MRI1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, Evanston, IL, United States, 4Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States
Synopsis
Keywords: Safety, In Silico, Numerical body position
Motivation: Use of commercial tools to reposition/pose numerical body models to match subject posture in MRI can result in significant non-anatomical distortions of the model.
Goal(s): Introduce approach to avoid non-anatomical distortions for a model in the seated position.
Approach: “Seated” versions of a body model were produced by: 1) using commercial software alone, and 2) strategically combining portions of the seated and original models offline followed by post-processing. SAR was calculated for both models in an open-bore double-donut MRI system.
Results: The Combined model avoided non-anatomical distortions seen when using the repositioning tool alone. These differences are also reflected in SAR distributions.
Impact: We introduce a method for avoiding significant non-anatomical distortions occurring in numerical body models when using commercial tools to reconfigure the posture/pose of the model. Use of this approach can also avoid related inaccuracies in calculated SAR and field distributions.
INTRODUCTION
Numerical body models have been repositioned/posed to match posture of subjects and staff in an MRI exam by, for example, for subjects moving arms away from the body or over the head (1) or bending of the knee (2), and for staff leaning over with arms in different positions (3, 4). This is most often done with repositioning tools available in commercial software, but the algorithms are simple and can result in significant non-anatomical distortions of the model. Here we present an approach to reduce some of these distortions with a focus on the challenging case of producing a numerical body model in a seated position.METHODS
Numerical models of a human body (“Duke” (5)) positioned with the femoral heads aligned with the center of a horizontal-bore double-donut type open MRI system allowing for standing or seated MRI were created. A “seated” version of the model was produced by two different methods: by using the “Poser” tool in a commercial software package (Sim4Life, Zurich MedTech AG) alone, and by strategically combining seated and original versions of the model offline using tools such as Matlab (The Mathworks) and ITK-Snap (6), conserving the pelvis and internal organs from the original model and portions distal to the middle of femoral heads (namely the legs and portion of the buttocks) from the seated model, followed by significant custom post-processing methods to ensure continuity of skin and subdermal fat.The body models were each then placed in a transmit RF coil consisting of two strategically-designed flat birdcages, one on either side of the body model. To accommodate the body in the seated position, a coil model from simulations for a vertical-bore double-donut type system (7) was scaled to increase all dimensions by 30%. For field simulations the coils, each having 12 radial “rungs” and (effectively) 3 circular “rings” were simulated in a commercial software environment (Sim4Life, Zurich MedTech AG) using current sources (12 in each ring, 36 in each coil, 72 total) at 21MHZ (0.5T) to approximate the current pattern in the strategically-designed commercial coil (8). Then fields were scaled to produce 2 microTesla at the coil center and resulting SAR was plotted for each body model.
RESULTS
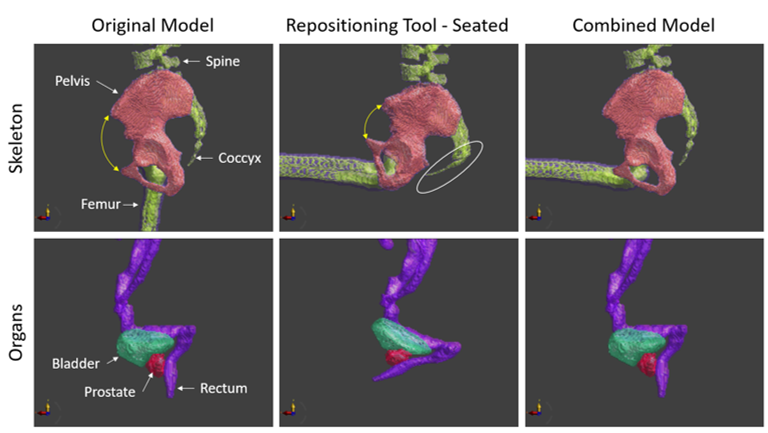
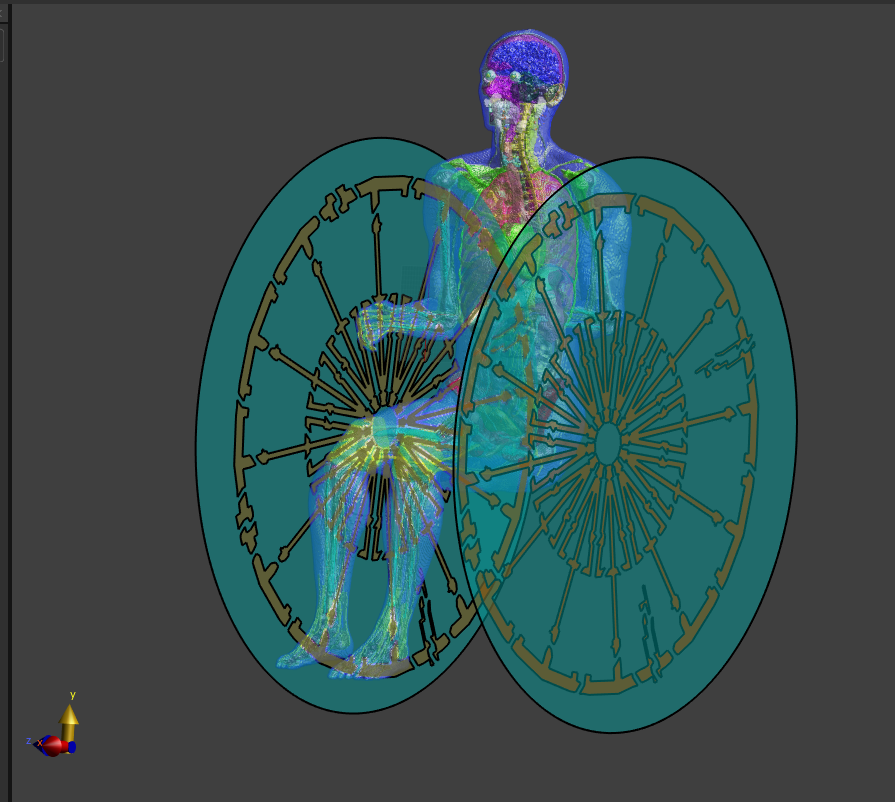
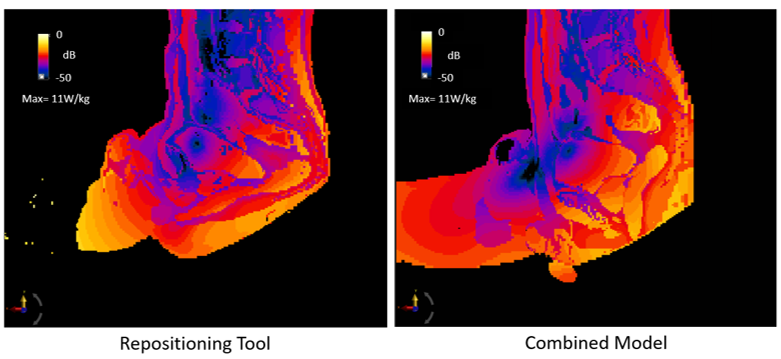
Figure 1 shows renderings of portions of the skeleton (top) and some internal organs (bottom) showing non-anatomical distortions of the Original model (left) when using the in-software repositioning tool (middle) such as severe bending of the pelvic bones and severe bending, rotation, and stretching of internal organs. These distortions are avoided with the Combined model (right). Figure 2 shows one of the seated anatomical models in the transmit RF coil. Figure 3 shows the peak SAR distribution in the two seated models during an RF pulse producing 2.0 microTesla at the coil center. Clear differences in the SAR distributions between the model created with the commercial Repositioning Tool (left) and our proposed Combined Model (right) are consistent with tissue configurations in the two models.DISCUSSION
We have shown that some significant distortions resulting from re-positioning body models to match the posture of subjects during MRI can be reduced by combining portions of the original model and re-positioned model from opposing sides of the articulating joint(s). This approach can require strategic choice of which tissues to preserve in overlapping regions and significant post-processing to ensure continuity of skin and anatomical integrity of other aspects of the final model.Acknowledgements
This work was performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), an NIBIB National Center for Biomedical Imaging and Bioengineering (NIH P41 EB017183).References
1. Collins CM, Wang Z. Calculation of radiofrequency electromagnetic fields and their effects in MRI of human subjects. Magnetic resonance in medicine. 2011 May;65(5):1470-82.
2. Brantner D, Collins CM. SAR Simulations with a Poseable Numerical Body Model for 3T MRI of Straight & Flexed Knee: First Results. Proc. 2023 ISMRM, p. 2700.
3. Oh S, Hong SE, Choi HD. Proposed Safety Guidelines for Patient Assistants in an Open MRI Environment. International Journal of Environmental Research and Public Health. 2022 Nov 17;19(22):15185.
4. Jia F, Littin S, Amrein P, Russe MF, Zaitsev M. Influence Of Arm Rotations On Peripheral Nerve Stimulation Thresholds For The Interventionalist In MR Guided Procedures. Proc. 2023 ISMRM, p. 2879.
5. Gosselin, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0, Physics in Medicine and Biology, 59(18):5287-5303, 2014.
6. http://www.itksnap.org/pmwiki/pmwiki.php
7. Kazemivalipour E, Vu J, Lin S, Bhusal B, Nguyen BT, Kirsch J, Elahi B, Rosenow J, Atalar E, Golestanirad L. RF heating of deep brain stimulation implants during MRI in 1.2 T vertical scanners versus 1.5 T horizontal systems: A simulation study with realistic lead configurations. In2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC) 2020 Jul 20 (pp. 6143-6146). IEEE.
8. https://patents.google.com/patent/JPWO2008108048A1/en?oq=JPWO2008108048A1
Figures