3743
On the combination of simulations from various human models to account for variabilities while limiting SAR10g overestimation for UHF pTx MRI1Aix Marseille Univ, CNRS, CRMBM, Marseille, France, 2APHM, Hôpital Universitaire Timone, CEMEREM, Marseille, France, 3School of Electrical Engineering and Computer Science, The University of Queensland, Brisbane, Australia, 4Siemens Healthcare Pty Ltd, Brisbane, Australia
Synopsis
Keywords: Safety, Safety, Parallel transmit (pTx); Spinal cord; Specific absorption rate;
Motivation: Reports highlight variability in 10g-averaged specific absorption rate (SAR10g) when varying subjects and radiofrequency coil position, necessitating safety factors to prevent underestimation, leading to overconservative SAR constraints.
Goal(s): To provide a method for selecting appropriate body models to balance RF safety and sequence performance, while investigating SAR10g variability in 7T spinal cord pTx MRI.
Approach: The impact of tissue properties, anatomy, body-mass index, and coil positioning on SAR10g was evaluated according to multiple metrics.
Results: The mean absolute percentage error can complement the safety factor to decrease SAR10g overestimation and guide the choice of human models used for SAR-monitoring.
Impact: Simulations of local-SAR in generic human models are widely used to ensure RF safety at 7T. We show that optimizing the choice of models used for SAR-monitoring may lead to less conservative SAR-constraints, which may improve sequence and pTx performance.
Introduction
Ultra-high field MRI at 7T has great potential for clinical and research applications, but challenges remain regarding the radiofrequency (RF) fields (B1 and specific absorption rate (SAR))1. Parallel transmit (pTx) technology is gaining traction, but RF safety remains a concern2. Reports highlight significant intersubject variability in 10g-averaged SAR (SAR10g), necessitating the use of safety factors to prevent underestimation3–5, which may lead to overconservative SAR constraints. Furthermore, SAR-monitoring is often based on simulations of arbitrarily chosen human models, sometimes lacking model variations (e.g varying RF coil positions, tissue properties,..) and a standardized method for selecting appropriate body models to balance RF safety and sequence performance.This study investigates the impact of tissue properties, anatomy, body-mass index (BMI), and coil positioning on SAR variability in 7T spinal cord pTx MRI. A novel method is introduced to select the best combination of human models to monitor SAR10g when calculating virtual observation points (VOP)6, ensuring both safety and performance are optimized.
Methods
Simulations of two 8Tx/Rx pTx RF coils were performed in Sim4Life (ZMT, Switzerland): a cervical spinal cord RF coil (Rapid Biomedical GmbH, Germany)7,8 and a thoracolumbar (TL) RF coil9 in a lumbar spinal cord MRI configuration10. Several human models11 were simulated with variations of tissue properties8 and coil position (see Fig.1 for details). VOPs of each model were calculated12 and used to obtain the peak-SAR10g for 1,000,000 random amplitude and phase RF shims.Safety factors (SF) were calculated to evaluate intersubject, BMI, tissue property and position-induced variabilities, as the factor required to prevent underestimation of the SAR10g for 99.9% of RF shims4 between a ‘predictor’ and ‘predicted’ model for all pairs of simulated cases for a given RF coil.In this work, different metrics were evaluated to also limit overestimation of the SAR10g between a predicted and predictor model, after applying SF to the latter: Overestimation factor (OF), as the lowest values of the ratio between SAR10g predicted and [predictor×SF] for 99.9% of RF shims; Normalized root mean square error (NRMSE), mean absolute percentage error (MAPE), correlation coefficient (R) and mean of the gaussian fit (µ) between SAR10g predicted and [predictor×SF].
The best combination of k models to use as VOPs from all N simulated models, according to the introduced metrics, was evaluated for k = [1:4] (with maximum 1 variation of each of the four human models included in the VOPs), and by comparing the peak SAR10g from those [predictor×SF] models to the N-k predicted ones for all $$$\binom{N}{k}$$$ possible combinations of models.
Results
Fig.2 shows the SF for all pairs of models for the two different coils. Highest SF were observed when using Jeduk as a predictor model for the cervical coil and with high BMI Ella and Fats as predictors for the TL coil.Fig.3 shows histograms of SAR10g ratios between variations and corresponding reference models, as well as the associated safety factor. For the cervical (thoracolumbar) RF coil, varying the subject position led to SF = [1.17:1.41] (SF = [1.2;1.46]), varying the tissue properties resulted in SF = 1.22 (SF = 1.3), and changing the BMI led to SF = 1.33 (SF = [1.18;1.56]).
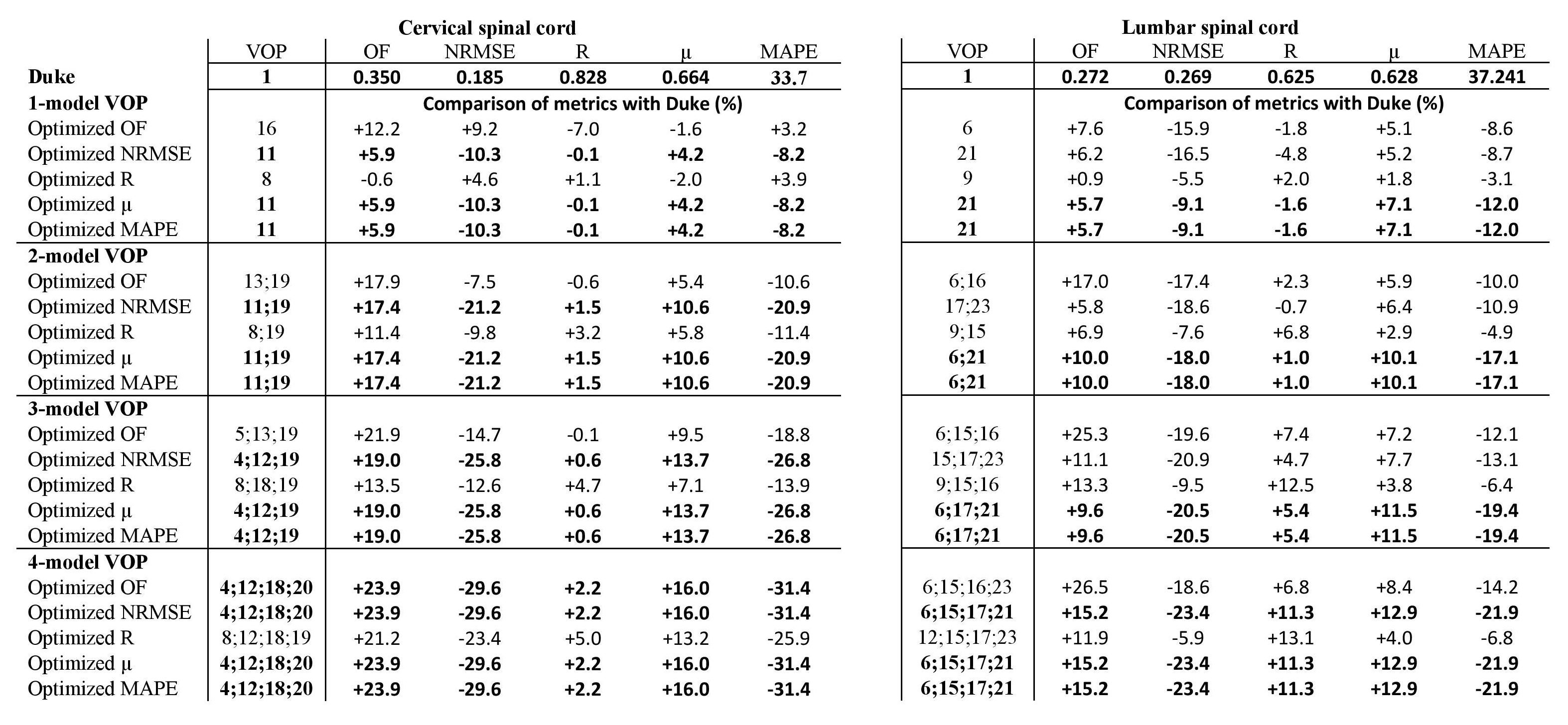
Fig.4 shows histograms of the ratios between models and the best VOPs with k = 4 according to the different metrics and when using Duke as VOP. Table 1 shows a quantitative comparison of the metrics for Duke and when k models were included in the VOPs. Best results for all metrics were obtained for k = 4, with improvements for the cervical (thoracolumbar) coil of 23.7% (26.5%), 30.3% (22.1%), 5% (13.1%), 15.8% (13%) and 31.3% (22%) for optimized OF, NRMSE, R, µ and MAPE, respectively.
Discussion and Conclusion
The intersubject variability observed in this study is in agreement with previous works on body MRI3–5. Although few works have included investigations of tissue property and coil position-induced SAR10g variability13,14, corresponding SF are in the same range as comparing completely different subjects (with the exception of certain predictors requiring higher SF). Furthermore, arbitrarily choosing a ‘reference’ model (e.g. Duke only, as found in the literature) to provide VOPs led to suboptimal SAR10g monitoring, with a high level of overestimation. Optimizing MAPE or µ led to the best performance among included metrics, resulting in MAPE being used in our group as a metric to complement SF. Future studies should include as many human models and variations as possible and optimize the choice of models to create VOPs, which may lead to performance gains for SAR-demanding sequences and when using pTx methods15 (improved coverage and B1 uniformity, for instance, by relaxing SAR constraints).Acknowledgements
Fondation pour l’aide à la recherche sur la sclérose en plaques (ARSEP), Institut Marseille Imaging, A*midex and France Life Imaging (FLI) for funding this project; ZMT (Zurich MedTech, Switzerland) for providing the academic license of the software Sim4Life.References
1. Ugurbil K. Imaging at ultrahigh magnetic fields: History, challenges, and solutions. Neuroimage. 2018;168:7-32. doi:10.1016/j.neuroimage.2017.07.007
2. Padormo F, Beqiri A, Hajnal JV, Malik SJ. Parallel transmission for ultrahigh-field imaging. Nmr in Biomedicine. 2016;29(9):1145-1161. doi:10.1002/nbm.3313
3. Ipek O, Raaijmakers AJ, Lagendijk JJ, Luijten PR, van den Berg CA. Intersubject local SAR variation for 7T prostate MR imaging with an eight-channel single-side adapted dipole antenna array. Magnetic Resonance in Medicine. 2014;71(4):1559-1567. doi:10.1002/mrm.24794
4. Meliado EF, den Berg CAT, Luijten PR, Raaijmakers AJE. Intersubject specific absorption rate variability analysis through construction of 23 realistic body models for prostate imaging at 7T. Magnetic Resonance in Medicine. 2019;81(3):2106-2119. doi:10.1002/mrm.27518
5. Schmidt S, Ertürk MA, He X, Haluptzok T, Eryaman Y, Metzger GJ. Improved 1H body imaging at 10.5 T: Validation and VOP-enabled imaging in vivo with a 16-channel transceiver dipole array. Magnetic Resonance in Medicine. 2023;n/a(n/a). doi:10.1002/mrm.29866
6. Eichfelder G, Gebhardt M. Local Specific Absorption Rate Control for Parallel Transmission by Virtual Observation Points. Magnetic Resonance in Medicine. 2011;66(5):1468-1476. doi:10.1002/mrm.22927
7. Massire A, Taso M, Besson P, Guye M, Ranjeva JPP, Callot V. High-resolution multi-parametric quantitative magnetic resonance imaging of the human cervical spinal cord at 7T. NeuroImage. Published online 2016. doi:10.1016/j.neuroimage.2016.08.055
8. Destruel A, Jomin P, Wichmann T, Guye M, Abdeddaim R, Callot V. B1 shimming for cervical spine 7T parallel transmission MRI: preliminary in vivo imaging and preparation of virtual observation points. Proceedings of the Annual Meeting of ISMRM. 2022;London, England:1463.
9. Destruel A, Jin J, Weber E, et al. Integrated Multi-Modal Antenna With Coupled Radiating Structures (I-MARS) for 7T pTx Body MRI. IEEE Transactions on Medical Imaging. 2022;41(1):39-51. doi:10.1109/TMI.2021.3103654
10. Destruel A, Weber E, Li M, et al. A novel type of radiofrequency antenna for multi-regional 7T MRI. In: Proceedings of the Annual Meeting of ISMRM. ; 2021:0135.
11. Gosselin MC, Neufeld E, Moser H, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0. Physics in Medicine and Biology. 2014;59(18):5287-5303. doi:10.1088/0031-9155/59/18/5287
12. Orzada S, Fiedler TM, Quick HH, Ladd ME. Local SAR compression algorithm with improved compression, speed, and flexibility. Magnetic Resonance in Medicine. 2021;86(1):561-568. doi:10.1002/mrm.28739
13. Terekhov M, Elabyad IA, Lohr D, et al. Complementary analysis of specific absorption rate safety for an 8Tx/16Rx array with central symmetry of elements for magnetic resonance imaging of the human heart and abdominopelvic organs at 7 T. NMR in Biomedicine. 2023;36(12):e5023. doi:10.1002/nbm.5023
14. Doran E, Naim I, Bowtell R, Gowland PA, Glover PM, Bawden S. The impact of variations in subject geometry, respiration and coil repositioning on the specific absorption rate in parallel transmit abdominal imaging at 7 T. NMR in Biomedicine. 2023;e5032. doi:10.1002/nbm.5032
15. Destruel A, Mauconduit F, Massire A, et al. Optimized interferometric encoding of presaturated TurboFLASH B1 mapping for parallel transmission MRI at 7 T: Preliminary application for quantitative T1 mapping in the spinal cord. Magnetic Resonance in Medicine. 2023;90(4):1328-1344. doi:10.1002/mrm.29708
Figures
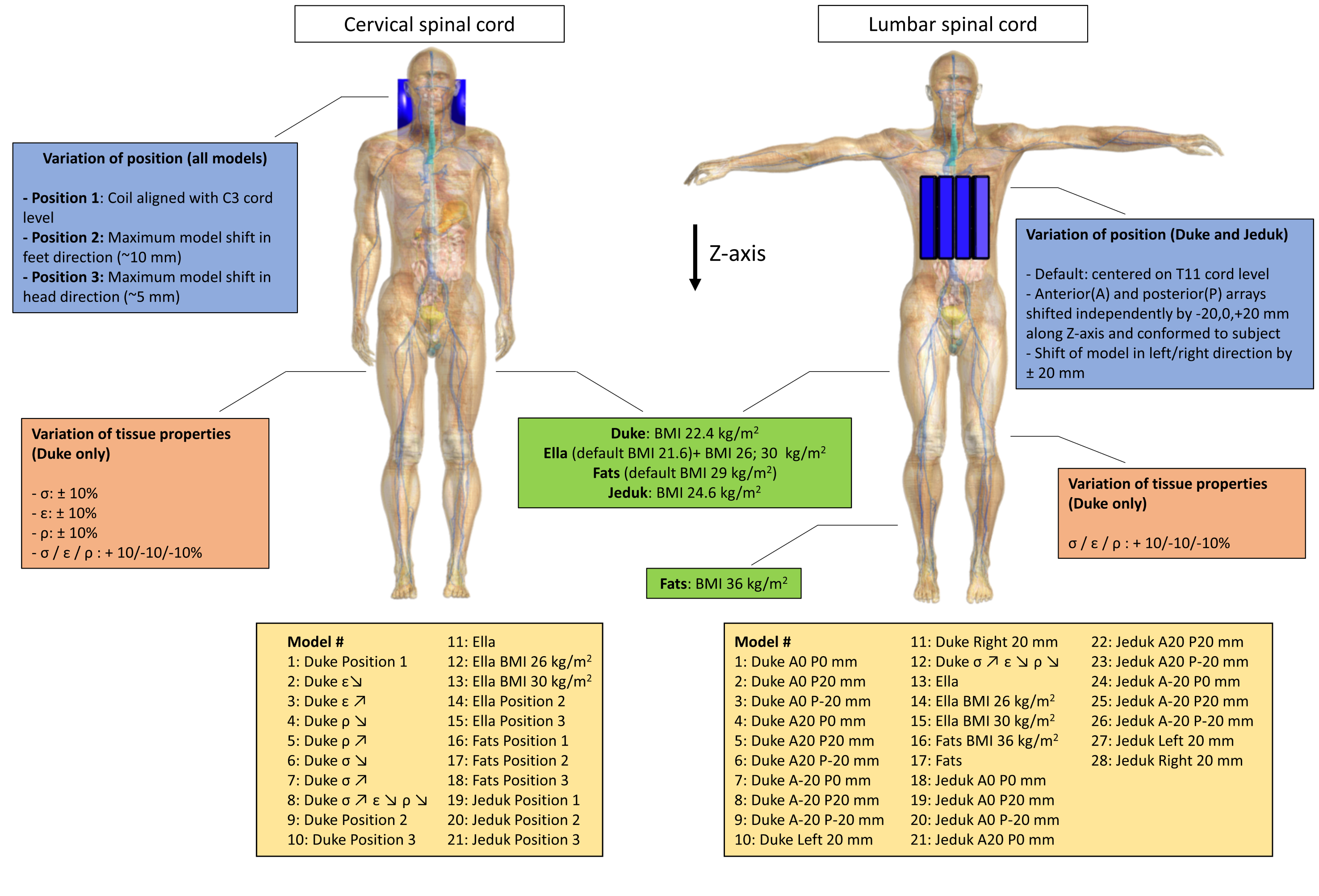
Fig.1: Human models and their variations in: (A) a cervical spine RF coil; (B) a thoracolumbar spine RF coil (anterior and posterior 4-channel arrays). For the cervical spine coil, Z-axis shift was limited by contact between back of the head and shoulders with the housing; for the thoraco-lumbar spine coil, anterior (A) and posterior (P) arrays were shifted independently along the Z-axis, and simultaneously in the left/right direction, and each element was repositioned to best conform with the human model; (σ: conductivity; ε: relative permittivity; ρ: density).
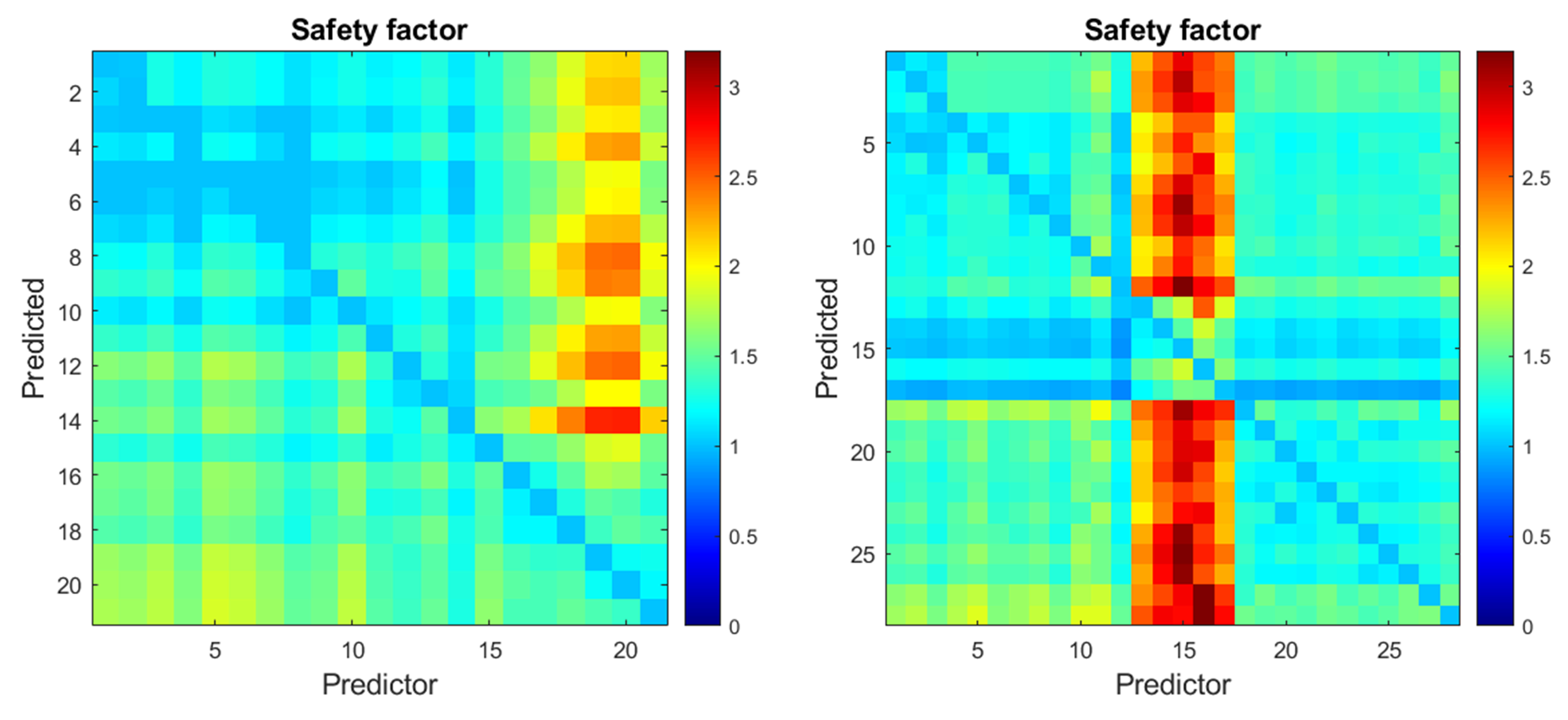
Fig.2: Safety factor (SF) to prevent underestimation of the SAR10g for 99.9% of RF shims, calculated for all pairs of human models simulated with the (A) cervical spine and (B) thoracolumbar spine RF coil. All simulations were normalized to 1W total input power (see Figure 1 for details on the models). For the cervical RF coil, maximum SF = 2.7 was observed when using model #20 (Jeduk Position 2) to predict the SAR10g in model #14 (Ella Position 2). For the thoracolumbar RF coil, maximum SF = 3.4 was observed when using model #16 (Fats) to predict the SAR10g in model #27 (Jeduk Left 20 mm).
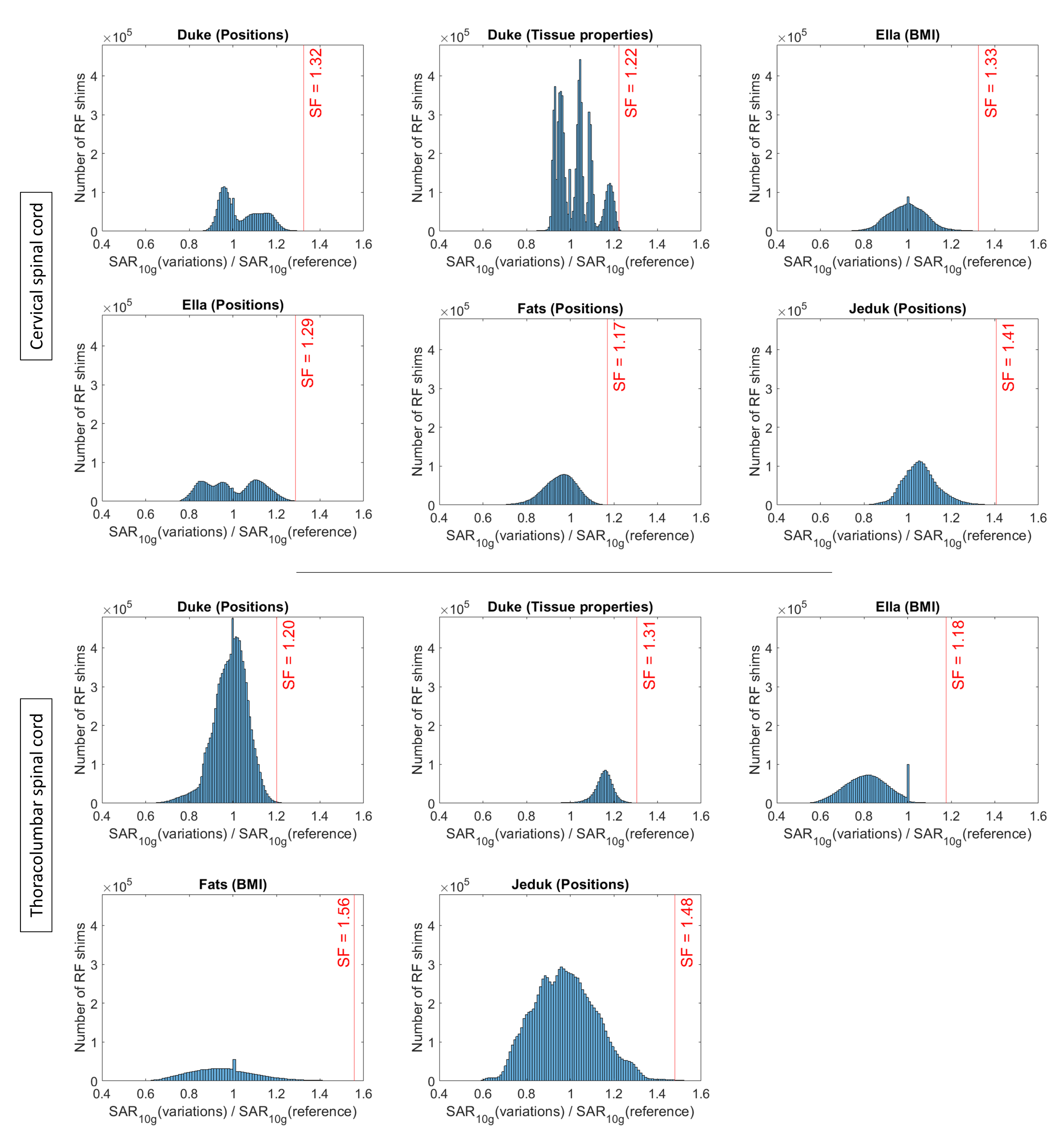
Fig.3: Histograms of the ratio between the SAR10g of reference human models and their variations with regard to position, tissue properties, and BMI, when applicable, for the (A) cervical and (B) thoraco-lumbar spine coil. For (A), reference models of Duke, Ella, Fats, and Jeduk were models #1, 11, 16, 19, respectively; for (B), reference models of Duke, Ella, Fats and Jeduk were models #1, 13, 16, 18, respectively (see Figure 1 for details).
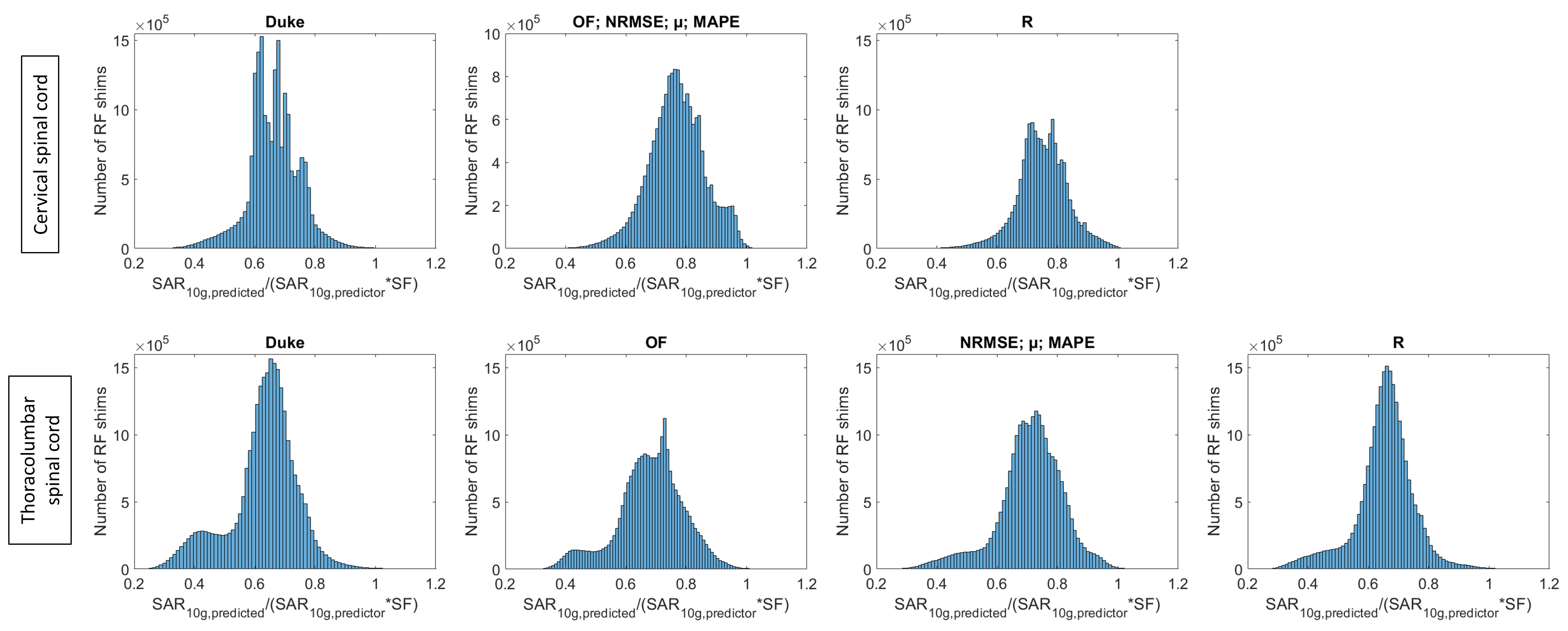
Fig.4: Histograms of the ratio between SAR10g of the predicted models, and of the predictor model after applying the safety factor, using Duke and best combinations of 4 human models according to each of the different metrics as predictors (metrics giving identical optimal VOPs were combined).