3731
Can B1+RMS help prevent overly restrictive MR Conditional labels for medical devices that are currently based on SAR?1MED Institute, West Lafayette, IN, United States
Synopsis
Keywords: Safety, Safety, Low-Field MRI, B1+RMS, SAR
Motivation: The primary RF exposure metric used for MR Conditional labeling of medical devices is whole-body(wb) average SAR, which is typically overestimated by MRI scanners, leading to potentially overly restrictive labels.
Goal(s): The purpose of this study was to determine if B1+RMS as an RF exposure limit can help prevent overly restrictive MR Conditional labels.
Approach: In-vivo RF-induced heating simulations in a 0.55 T MRI scanner were performed to compare potential labeling at the scanner-reported B1+RMS and wbSAR with the driving voltage maximized.
Results: Results depicted a 7-13x decrease in maximum temperature rise when the RF exposure is limited by B1+RMS instead of wbSAR.
Impact: The use of B1+RMS to limit RF exposure instead of SAR has significant potential to prevent unnecessarily restrictive MR Conditional labels for medical devices, especially in lower magnetic field strength MRI systems that are incapable of achieving high SAR levels.
Introduction
Radiofrequency (RF)-induced heating is one of the primary safety concerns for patients with implanted medical devices in an MR environment, but the concern may be mitigated by limiting RF exposure. The primary metric used for limiting RF exposure is whole-body average specific absorption rate (wbSAR). Since wbSAR is dependent on patient habitus and positioning within the RF coil, it is typically overestimated by scanner manufacturers to provide conservative safety conditions and can therefore result in unnecessarily restrictive MR Conditional labeling.An alternative RF exposure metric, the root mean square (RMS) of the component of the RF magnetic field that tilts the nuclear magnetization (B1+), is independent of the patient being scanned, allowing it to be directly and accurately calculated by an MRI scanner using a standardized equation1, potentially eliminating overestimation. This allows any scanning sequence that has a B1+RMS within the limit listed on an MR Conditional label to be applicable for any patient. Still, the SAR limits are predominantly used for MR Conditional labeling of electrically passive devices. The purpose of this study was to determine if using B1+RMS in place of SAR to limit RF exposure can help prevent overly restrictive MR Conditional labeling.
Methods
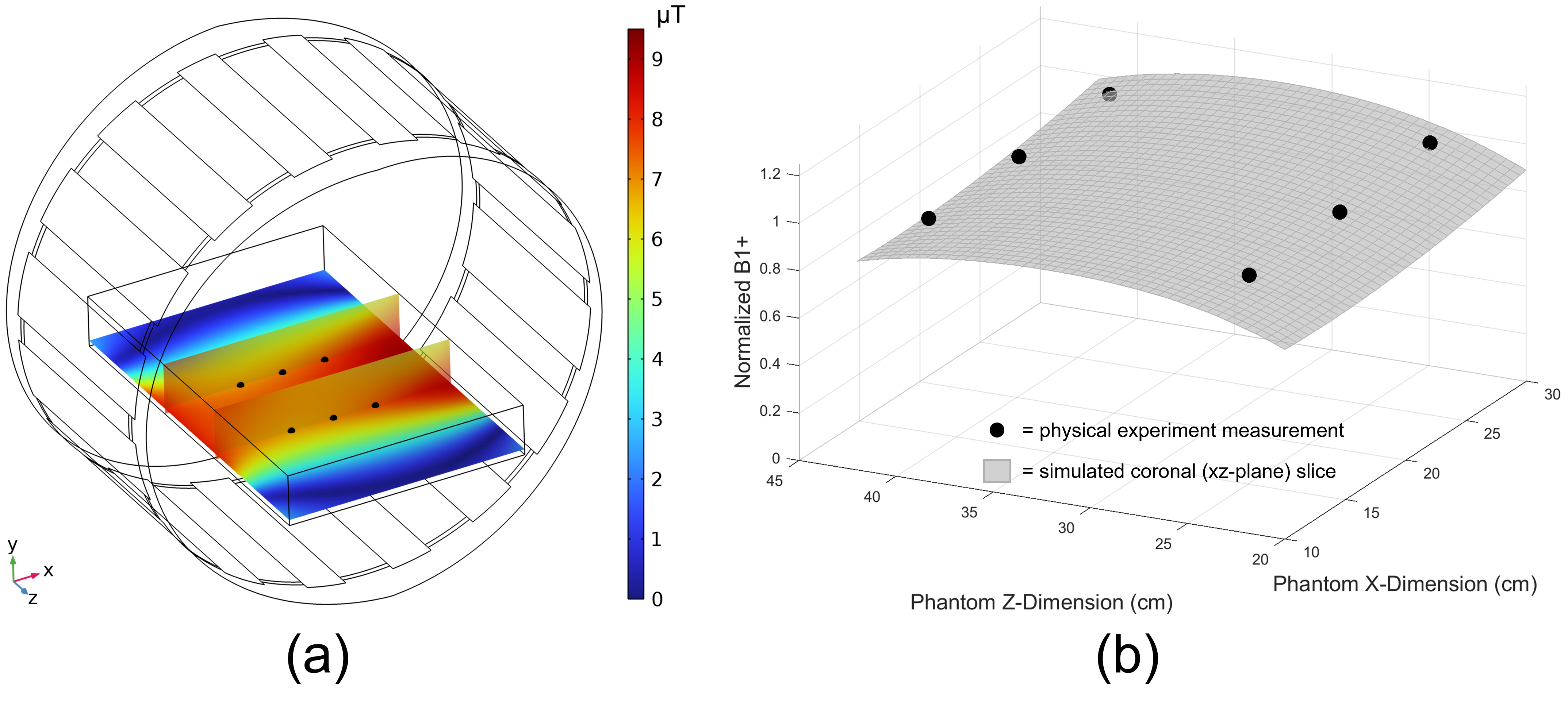
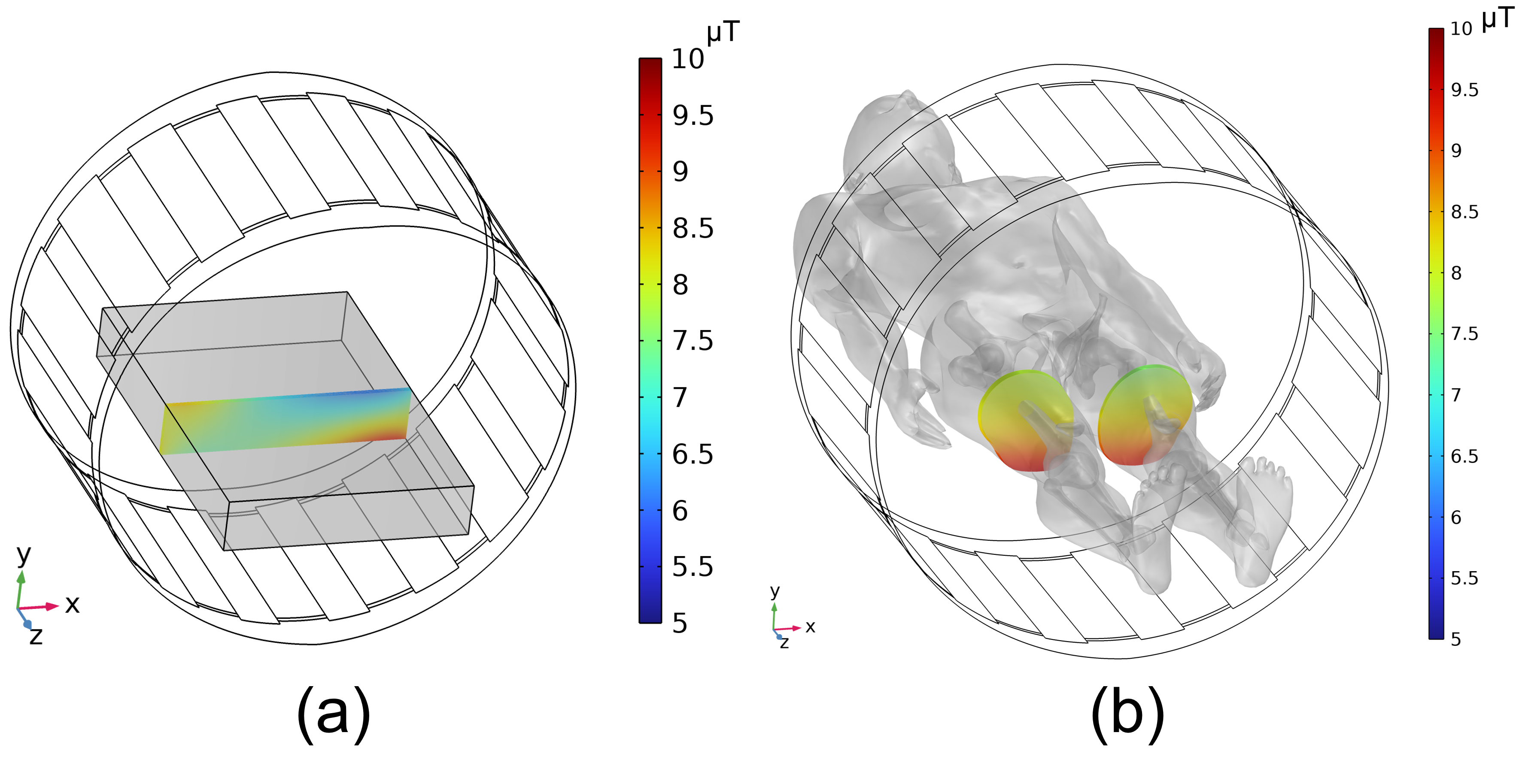
H-field measurements (H3DV8, SPEAG) within the ASTM gel phantom in a Siemens Healthineers 0.55 T MAGNETOM Free.Max MRI scanner were used to validate simulated B1+(Figure 1) using a scanning sequence that utilized the maximized the scanner driving voltage (i.e., worst-case RF exposure) and yields a known temperature rise for a titanium calibration rod. Fully-coupled electromagnetic and heat transfer simulations were conducted in COMSOL v6.0 using RF coil geometry provided by Siemens Healthineers and voltage calibrated to match the calibration rod temperature. Simulated RF-induced heating in the Duke virtual human anatomy with a 27 cm femoral intramedullary nail at three locations within the RF coil was determined for two different RF exposure limits, the scanner-reported B1+RMS and wbSAR. Simulated B1+RMS was calculated as the spatially averaged B1+ in a 10 mm thick axial slab through Duke at isocenter (Figure 2) per the standardized equation1, similar to previous studies2,3.Results
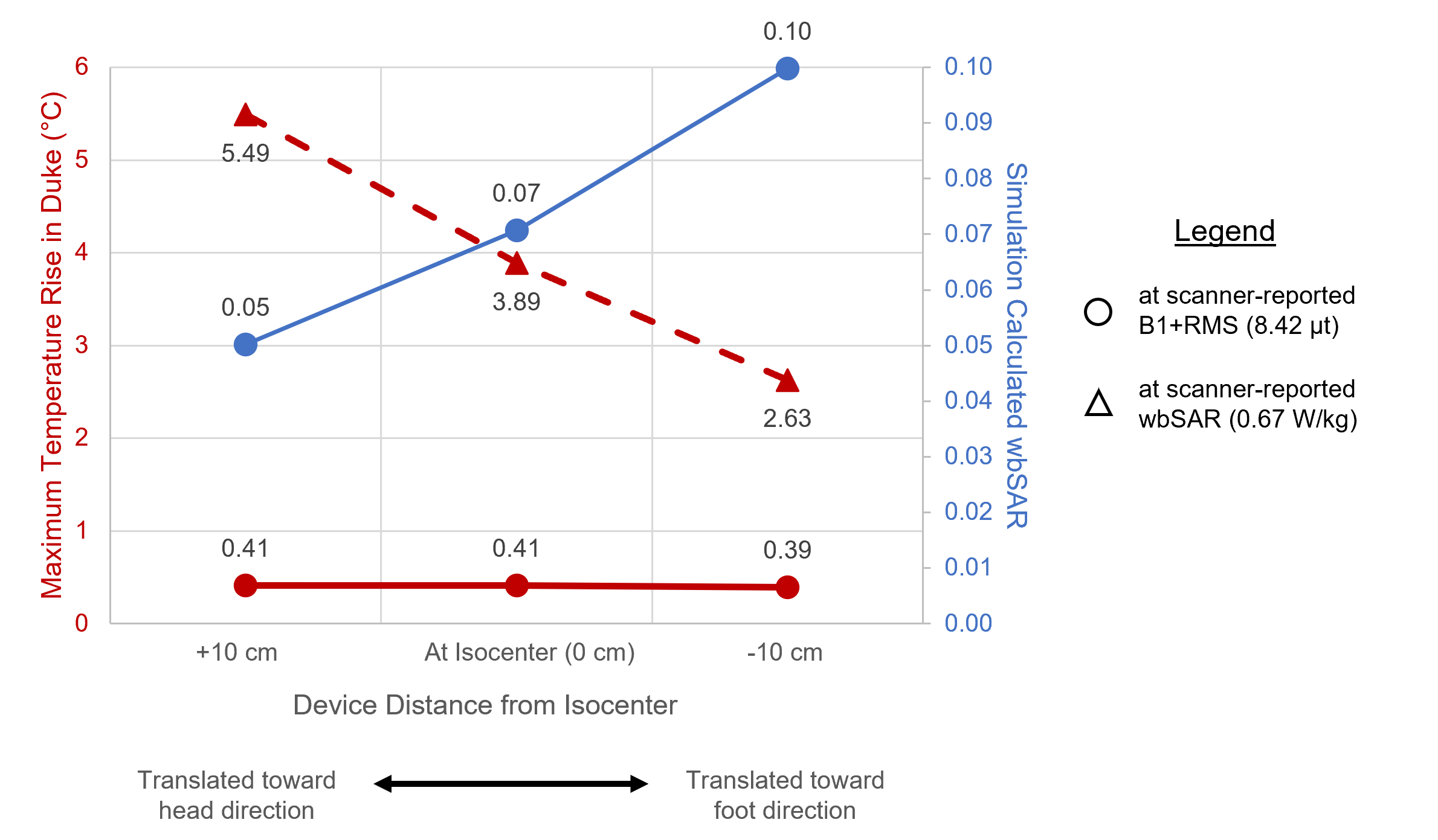
Normalized physical experiment and simulated B1+ measurements (Figure 1b) depict that the two measurements have good agreement when a linear adjustment factor is accounted for (maximum percent difference of 5.7% at physical experiment measurement points). The 10.7% difference between simulated B1+RMS in the ASTM gel phantom with voltage calibrated to match physical testing RF exposure and the scanner reported B1+RMS (7.52 µT and 8.42 µT, respectively) further validated the B1+RMS distribution within the simulation tool.In-vivo RF-induced heating results are displayed in Figure 3. As expected, due to conservative scanner calculations, the scanner-reported wbSAR of 0.67 W/kg is noticeably larger than the simulation-calculated wbSAR at the scanner-reported B1+RMS, approximately 7-13x, corresponding to an approximately 7-13x potential overestimation of in-vivo heating. The overly conservative nature of simulating at a calculated wbSAR value that corresponds to a scanner-reported wbSAR value is especially noticeable when a significant portion of the patient is outside of the RF coil, as depicted by the increase in disparity between temperature rise values in Figure 3 as the virtual human is translated towards the head direction (i.e., lower body within RF coil).
Discussion and Conclusions
SAR is directly proportional to the square of the static magnetic field strength (B0) of an MRI scanner. So, for a given pulse sequence, the wbSAR of a patient at 0.55 T would be 7.4x and 29.8x lower than at 1.5 T and 3 T, respectively. This allows for significantly less potential for RF-induced heating of devices at 0.55 T, as demonstrated by Campbell-Washburn et al.4 However, this also means that RF exposure limits based on overestimated scanner-reported wbSAR values have significant potential to be unnecessarily restrictive at 0.55 T where high levels of wbSAR are unachievable, as demonstrated in this study.Heating results from this study and current regulatory guidelines indicate that an hour-long scanning session for a patient with the femoral implant should incorporate cooling periods based on the scanner-reported wbSAR as a limit, whereas the patient could be scanned for an hour continuously based on the scanner-reported B1+RMS as an exposure limit. This indicates that B1+RMS has the potential to help prevent overly restrictive MR Conditional labeling. It is likely that these MR Conditional labeling differences would exist for other implants and even for MRI scanners with greater magnetic field strength, as these scanners also typically overestimate SAR. Future work could investigate the potential labeling differences for various devices in various MRI scanners.
Acknowledgements
The authors would like to thank Siemens Healthineers for providing information regarding their RF coil.References
[1] IEC 60601-2-33:2022, Medical electrical equipment – Part 2-33: Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis.
[2] K. Fujimoto et al., "Comparison of SAR distribution of hip and knee implantable devices in 1.5T conventional cylindrical-bore and 1.2T open-bore vertical MRI systems," Magnetic Resonance in Medicine, vol. 87, no. 3, pp. 1515-1528, 2021.
[3] M. Murbach, E. Zastrow and N. Kuster, "Virtual Population Based Correlations between B1+, Whole-Body and Local SAR," in Proc. Intl. Soc. Mag. Reson. Med. 26 (2018) (Abstract 4391), 2018.
[4] A. E. Campbell-Washburn et al., "Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI," Radiology, vol. 293, no. 2, pp. 384-393, 2019.
Figures