3728
SAR Efficient Imaging for Patients with Deep Brain Electrodes at 3 Tesla: Coil Length Matters1Biomedical Engineering, King's College London, London, United Kingdom, 2Centre for the Developing Brain, King's College London, London, United Kingdom
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems
Motivation: To improve the design of pTx head coils intended to produce uniform RF fields while controlling local SAR levels for patients with DBS implants.
Goal(s): To evaluate the effect of extended coil length and increased number of rows on performance using simulations.
Approach: Comparison of SAR and RF homogeneity in 3-row and 4-row pTx head coil configurations using FDTD simulations on a human head model with an implanted DBS lead.
Results: The 4-row coil offered the best SAR control for the whole brain, with length having a greater impact on local SAR than the number of rows.
Impact: The research indicates that the length of multi-row pTx coils affects local SAR in MRI for DBS patients, enhancing efficiency and safety, and broadening imaging possibilities, potentially advancing MRI-compatible devices and personalized imaging techniques.
Introduction
Multi-row parallel-transmit (pTx) coil arrays can provide improved control over excessive tissue heating in patients with Deep Brain Stimulation (DBS) devices, increasing transmit efficiency and improving radiofrequency field (B1+) homogeneity at 3T [1][2]. In an earlier study [3], we noticed that the peak SAR after whole-head RF shimming with multi-row pTx coils tended to be at the top of the head, which suggested that the overall length of the pTx array could be important for SAR control in this scenario. In this study, we tested this hypothesis by a) adding a row and b) stretching loop sizes to increase length.Method
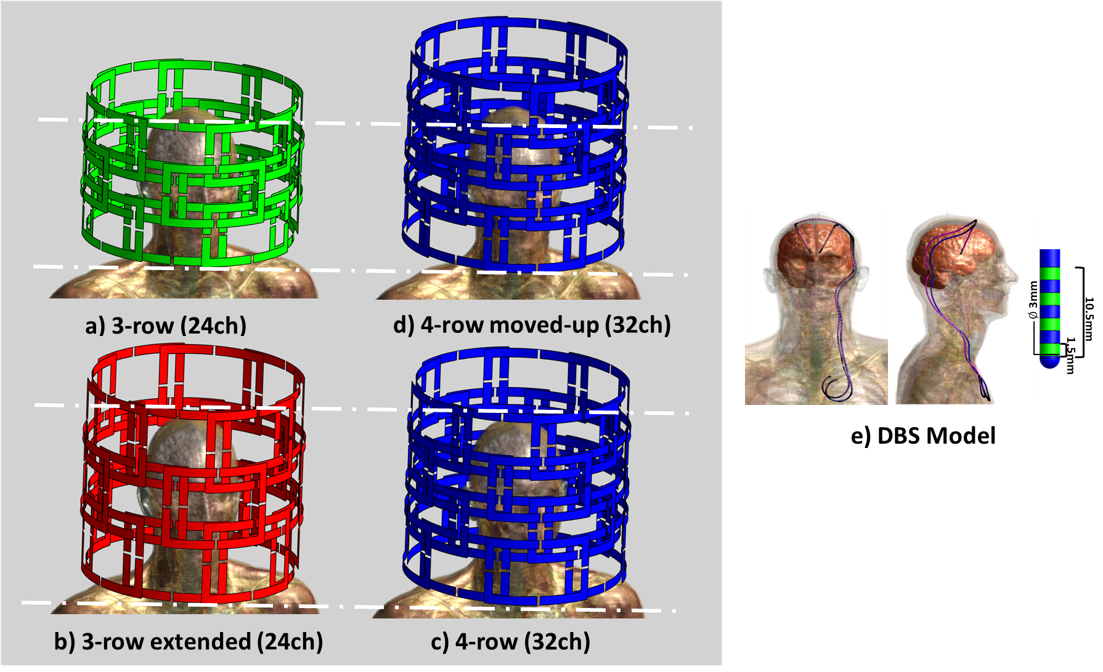
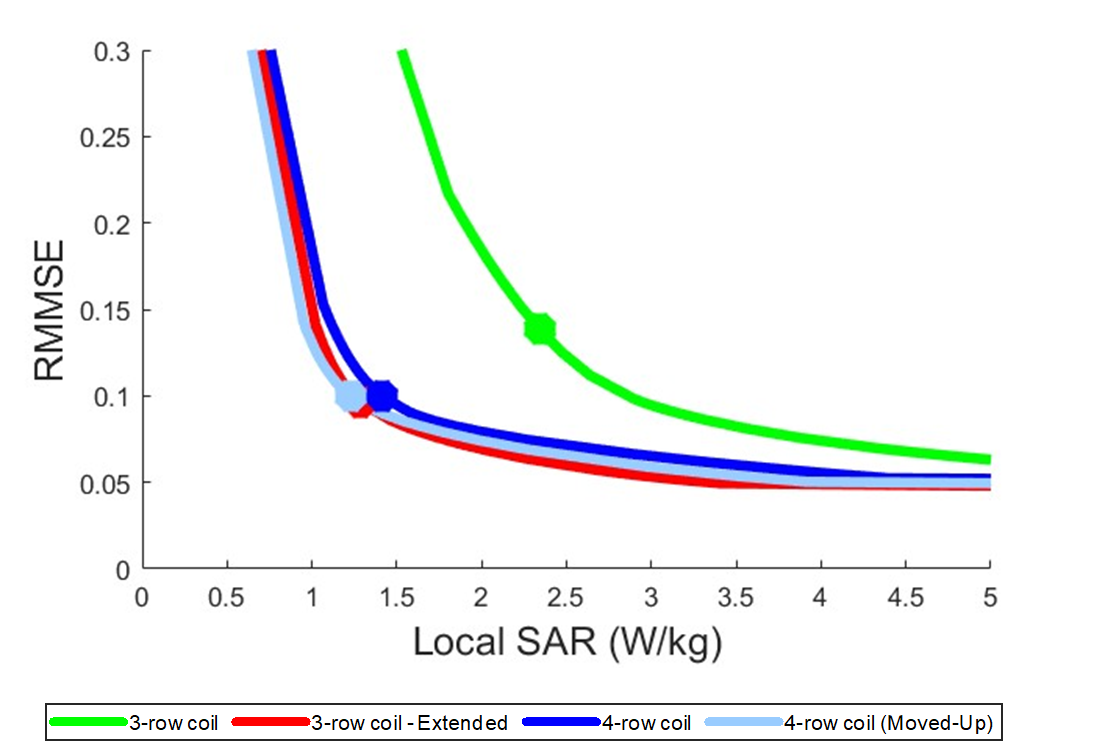
We evaluated three different pTx head coil configurations at 3T, all with diameter (D) of 360mm positioned head-centred on the Duke human model [4]: a baseline 3-row 24-channel (3x8) loop coil with length (L) of 250mm(Fig.1.a)[1], an extended 3-row 24-channel (3x8)(Fig.1.b), and a 4-row 32-channel (Fig.1.c) both with L: 320mm. The 4-row coil was also simulated such that the centre of the head was in the same position as for the shorter 3-row coil(Fig.1.d), which required a translation by 35mm of the longer coil. All coil arrays consisted of overlapped loops, placed in the iso-centre of the magnet bore and simulated using multiport FDTD simulations Sim4Life 7.1(ZMT, Switzerland) tuned at 123MHz and matched to 50Ω using co-simulation software co-simulation(Optenni Ltd, Finland).The DBS lead (trajectory obtained from Medtronic) comprises a conductive wire (D: 1mm) insulated by a 1mm thick layer following the realistic bilateral DBS electrode model (Medtronic-3387) with four pad electrodes (D:1.5mm, L:1.5mm) placed 1.5mm apart at the lead's distal end (Fig.1.e). Individual B1+ fields and electric fields were extracted on a head and chest sensor volume (201x251x401mm), resampled to a 1mm isotropic image grid, and exported to Matlab (MathWorks,Inc.). Q-matrices were derived from simulated E-fields and 1-g tissue mass-average to evaluate SAR1gr,avg[5]. Virtual Observation Points (VOP) were generated from these Q-matrices[6] and used to regularise a Magnitude Least Square (MLS) shim optimization with a uniform target field of 1μT over the entire brain[7]. L-curves were produced by systematically varying the regularisation parameter and used to select optimal solutions (marked by dots in Fig. 3). These were assessed in more detail by constructing histograms of B1+ and examining maximum intensity projections (MIP) of B1+ and local SAR as determined from the full Q-matrices.
Results
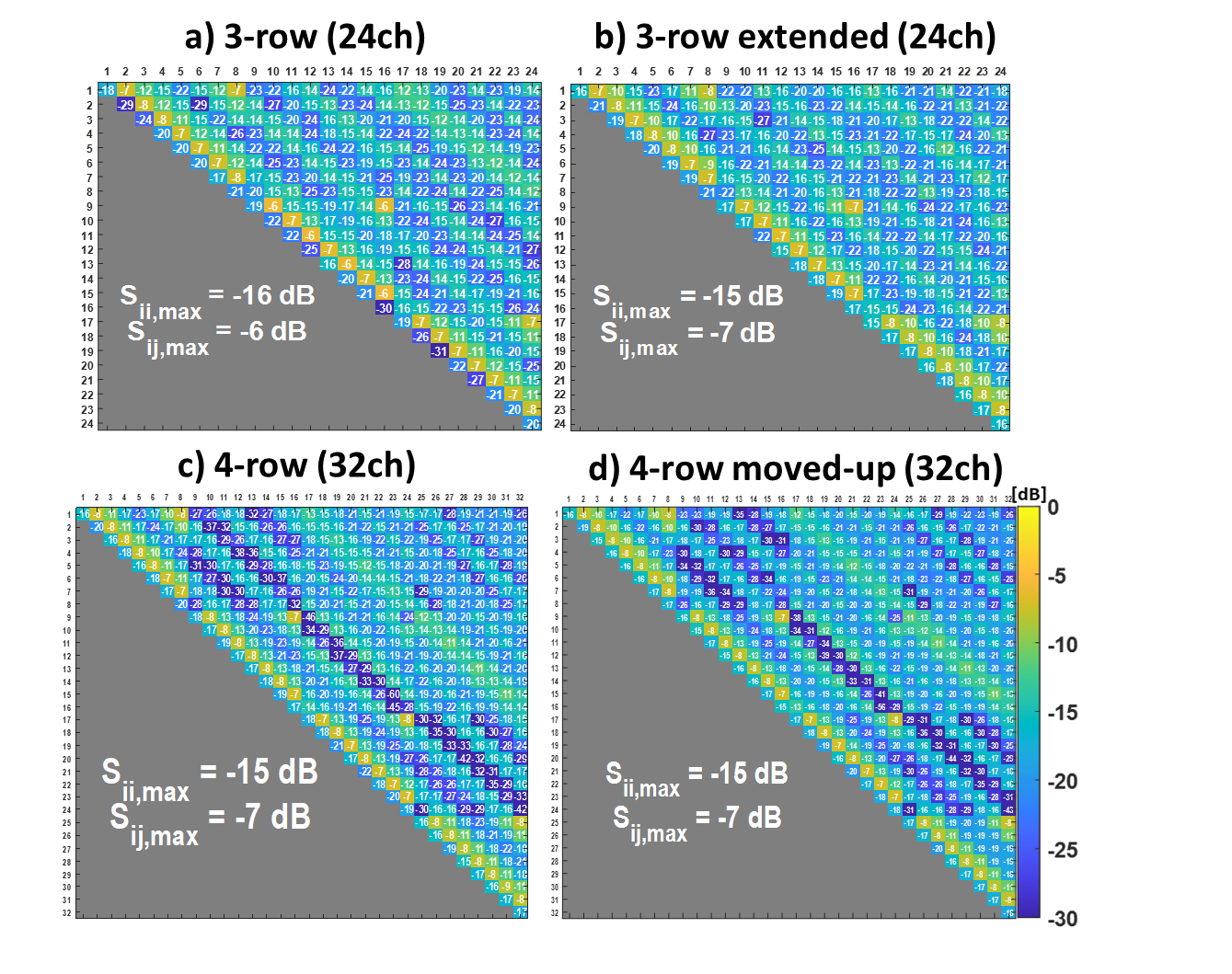
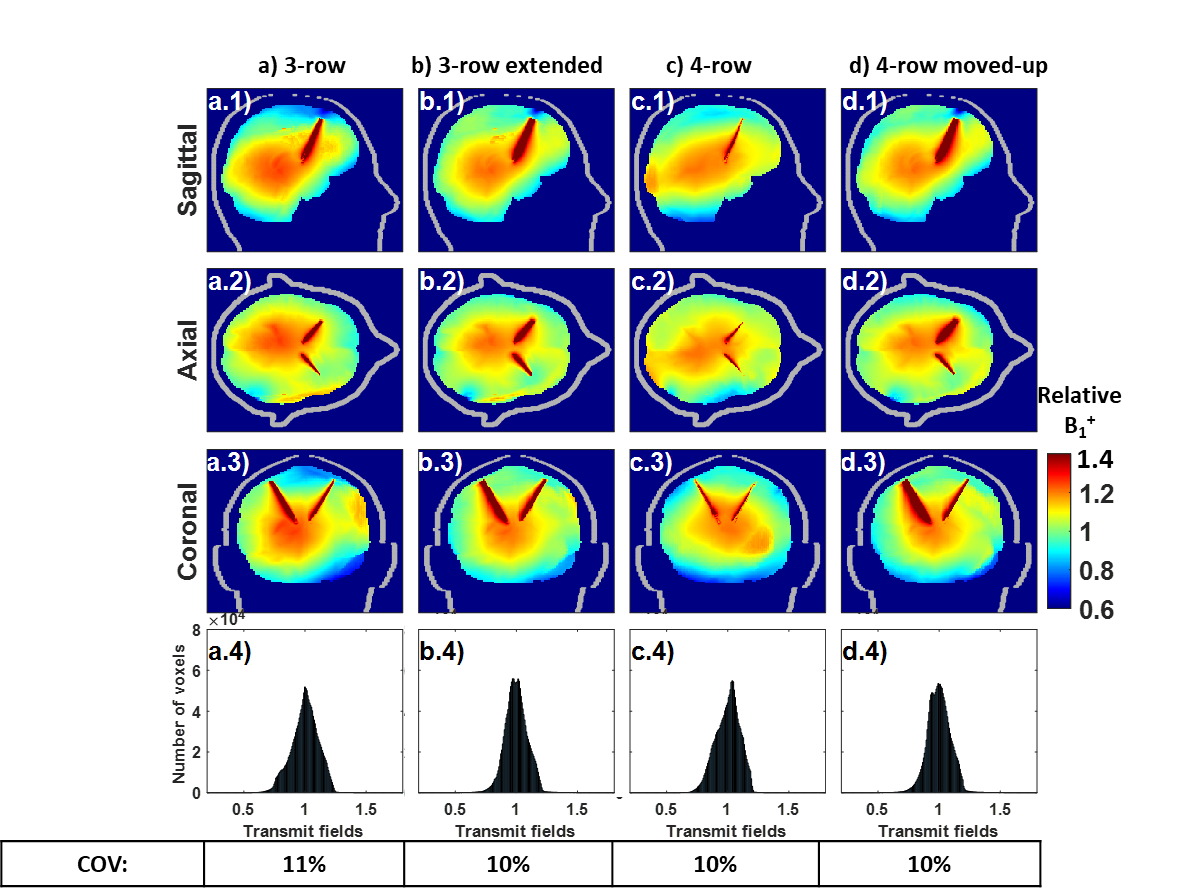
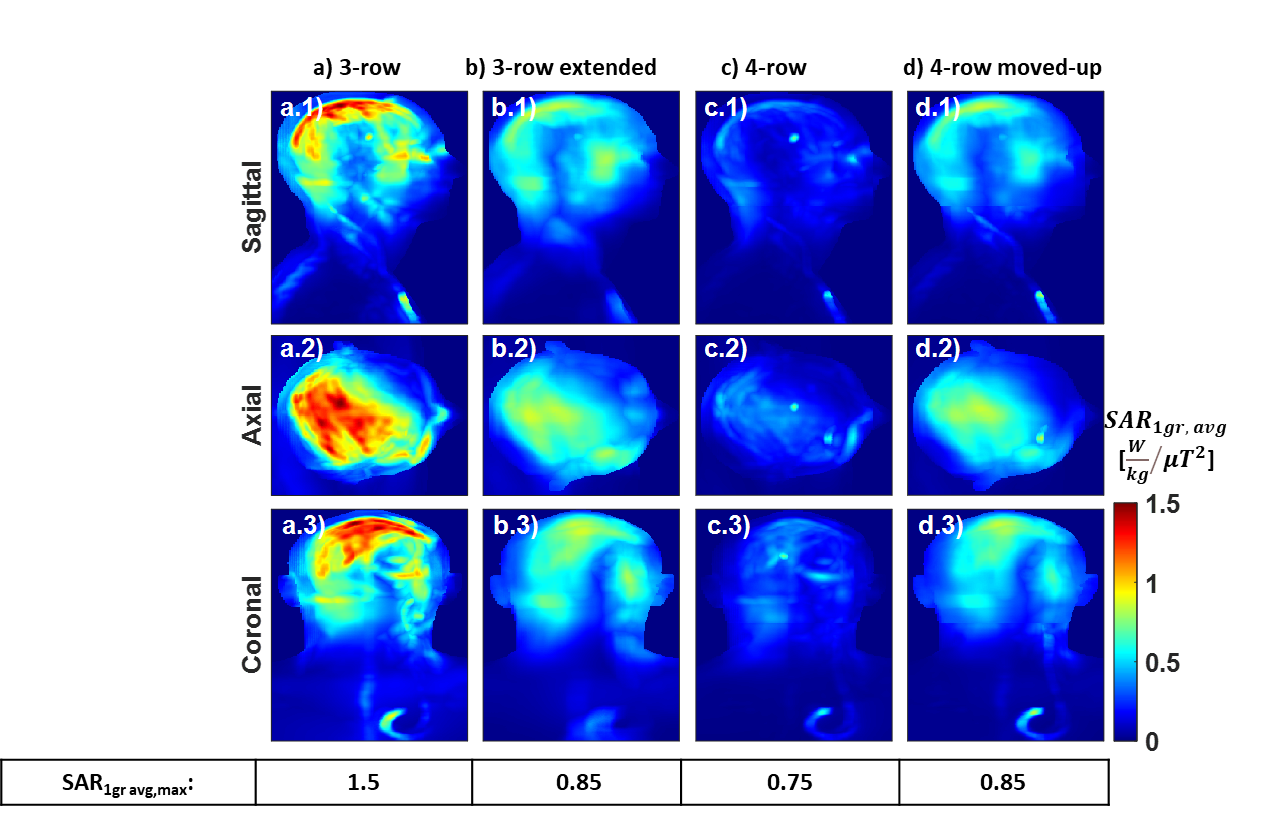
The tuned coils exhibited maximum reflection coefficients of -16dB for the 3-row and -15dB for the 3-row (extended), 4-row, and 4-row(elevated) configurations(Fig.2), while the maximum coupling coefficients were: -6dB for the 3-row and -7dB for other configurations.The L-curves for the longer coils are coincident, and all are shifted to the left compared to the shorter baseline coil(Fig.3), indicating a capability to reduce local SAR for the same transmit field homogeneity. The corresponding B1+ MIP maps show approximately equal performance(Fig.4), but the MIP SARmax,1g avg maps(Fig.5) show systematically lower values with the high SAR region at the top of the head(Fig.5a arrows) eliminated by the longer coils. The max SARmax,1g avg values are marginally lower for the 4-row coil in head centred position(0.75W/kg)(Fig.4.c), and this also leads to the lowest whole head averaged SAR: 0.11W/kg vs. ~0.27W/kg for the other long coils and 0.33W/kg for the shorter coil. Matching the shorter coil head-centred position with the longer coil having the same loop sizes preserved the benefits of the extra length (Fig. 3,Fig. 4d,and 5d).
Discussion
This study examines the performance of pTx coils with 3 and 4 rows, exploring the effect of overall coil length for the Duke human model with a realistic DBS lead, targeting homogenous B1+ fields and minimized local SAR at 3T. The longer pTx coils achieve substantially lower local SAR for the same B1+ homogeneity when considering whole-head shimming. More rows of coils provided marginally lower peak local SAR, but this difference was smaller in magnitude. Whole head SAR was notably improved for the 4 row coil in its optimal position. Shifting the longer coil to match the head-centred position for the shorter coil so that all lower rows matched in geometry confirmed the importance of ensuring adequate spatial coverage overall.Conclusion
The length of head-sized pTx coils is an important parameter to consider when designing arrays intended to provide homogeneous B1+ fields over the whole brain while mitigating the risk of elevated SAR secondary to the presence of DBS electrodes in the brain. This small study suggests that ensuring adequate spatial extent is more important than increasing coil complexity for this specific application since 3 and 4-row designs had similar performance.Acknowledgements
This work was supported by DTP, by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.References
[1] N. Karadeniz, J. Hajnal, & Ö. Ipek. Uncompromised Safe Imaging of Patients with Deep Brain Electrodes at 3 Tesla with Multi-Row Parallel Transmit Coil Arrays: Electromagnetic Simulation Study. ESMRMB 40th Scientific Meeting, Basel, 2023.
[2] B. Guerin, L. M. Angelone, D. Dougherty, and L. L. Wald, 'Parallel transmission to reduce absorbed power around deep brain stimulation devices in MRI: Impact of number and arrangement of transmit channels', Magn. Reson. Med., vol. 83, no. 1, pp. 299–311, Jan. 2020, doi: 10.1002/MRM.27905.
[3] N. Karadeniz, J. Hajnal, & Ö. Ipek. Comparison of the transmit performance and Local SAR for multi-row parallel transmit coil arrays at 3 Tesla human brain MRI. 31st ISMRM Scientific Meeting, Toronto, 2023.
[4] M.-C. Gosselin et al., 'Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0', Phys. Med. Biol., vol. 59, no. 18, pp. 5287–5303, Sep. 2014, doi: 10.1088/0031-9155/59/18/5287.
[5] Ö. Ipek, A. J. Raaijmakers, J. J. Lagendijk, P. R. Luijten, and C. A. T. van den Berg, 'Intersubject local SAR variation for 7T prostate MR imaging with an eight-channel single-side adapted dipole antenna array', Magn. Reson. Med., vol. 71, no. 4, pp. 1559–1567, 2014, doi: 10.1002/mrm.24794.
[6] G. Eichfelder and M. Gebhardt, 'Local specific absorption rate control for parallel transmission by virtual observation points', Magn. Reson. Med., vol. 66, no. 5, pp. 1468–1476, 2011, doi: 10.1002/MRM.22927.
[7] A. Sbrizzi, H. Hoogduin, J. J. Lagendijk, P. Luijten, G. L. G. Sleijpen, and C. A. T. van den Berg, ‘Fast design of local N-gram-specific absorption rate–optimized radiofrequency pulses for parallel transmit systems’, Magn. Reson. Med., vol. 67, no. 3, pp. 824–834, 2012, doi: 10.1002/mrm.23049.
Figures